
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Cancer and tuberculosis: A lethal duo
Gyanshankar Mishra1*; Neha Pachbhai2
1 Associate Professor, Department of Respiratory Medicine, Indira Gandhi Government Medical College, Nagpur, Maharashtra, India.
2 Junior Resident, Department of Respiratory Medicine, Indira Gandhi Government Medical College, Nagpur, Maharashtra, India.
*Corresponding Author: Gyanshankar Mishra
Associate Professor, Department of Respiratory
Medicine, Indira Gandhi Government Medical College,
Nagpur, Maharashtra, India -440018.
Email: gpmishra81@gmail.com
Received : Aug 26, 2021
Accepted : Sep 22, 2021
Published : Sep 29, 2021
Archived : www.jcimcr.org
Copyright : © Mishra G (2021).
Abstract
Cancer patients are at an increased risk of developing active Tuberculosis (TB) disease. Immunosuppression because of cancer or its treatment modalities, including chemo-radiotherapy, places these patients at an increased risk of developing active TB. We describe the case of a fifty-eight-year-old male patient who was diagnosed and treated for carcinoma larynx but later succumbed to pulmonary TB. Active screening and treatment for Latent TB Infection (LTBI) at the start of cancer treatment in these patients may potentially help reduce the reactivation risk of active TB disease among them.
Keywords: tuberculosis; TB; cancer; malignancy; mortality; LTBI; chemo-radiotherapy
Citation: Mishra G, Pachbhai N. Cancer and tuberculosis: A lethal duo. J Clin Images Med Case Rep. 2021; 2(5): 1331.
Introduction
Tuberculosis (TB) is a major public health issue around the world. A person with Latent Tuberculosis Infection (LTBI) is infected with Mycobacterium Tuberculosis (MTB) but does not have active tuberculosis disease. Patients with cancer may have impairments in cell-mediated immunity due to chemotherapy, either directly or indirectly. As a result, many people who have LTBI and cancer develop active tuberculosis [1]. We herein describe one such case report of a patient diagnosed and treated with malignancy, developing tuberculosis later.
Case report
A fifty-eight-year-old male patient was admitted from the emergency department with complaints of chronic cough with expectoration for three months, fever for 3 days and sudden onset breathlessness since morning. The patient was on home oxygen therapy for the last one day. The patient was a known diabetic and hypertensive on medications. One year back patient was diagnosed with histopathologically confirmed laryngeal carcinoma. The patient had completed chemo-radiotherapy with 6 cycles of injection cisplatin and 36 sessions of radiotherapy, 6 months back, following which the patient had not received any chemo-radiotherapy in the last six months. In the emergency department, the patient was drowsy with an oxygen saturation of 50% on room air. Blood Pressure was 70/60 mm of Hg.
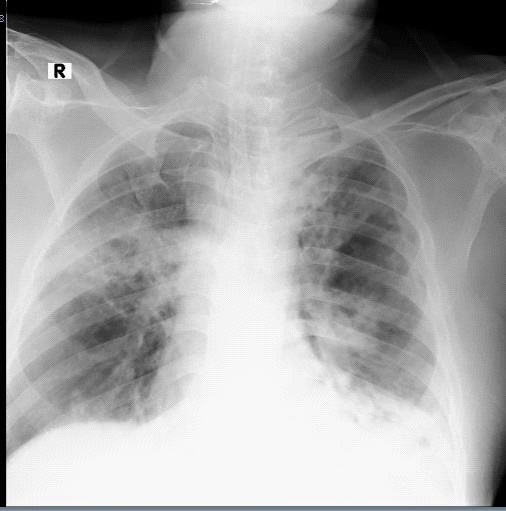
The patient was immediately intubated and put on invasive mechanical ventilator support with a SpO2 of 96% on a mechanical ventilator with 100% FiO2 requirement. The patient’s two RTPCR Covid tests, 24 hours apart on the day of admission, were negative. On admission, the patient’s chest radiograph revealed right mid-zone cavity with consolidation, left upper zone fibrosis, and left lower zones patchy consolidation, as shown in Figure 1. A review of reports revealed a one and a half months back, Contrast-Enhanced Computed Tomography (CECT) scan of abdomen, pelvis, and thorax report suggestive of 1. Calcifications in tunica albuginea and corpus cavernosa, bilaterally suggestive of probable peyronie’s disease. 2 Scattered reticulonodular infiltrates with patchy consolidation and thick-walled cavity in lower lobes of both lungs with mediastinal lymphadenopathy (Largest lymph node size 2 X 1.5 cm).
The patient tested negative for the Widal test. Complete blood count: Total leukocyte count: 6490/mm3 , Differential Counts: Neutrophil: 85%, Lymphocytes: 9%, Eosinophils: 3%, Monocyte: 3%, Platelet Counts: 1,50,000/mm3 & Hemoglobin: 10.7 gm/dl. C-reactive protein was 41.09 mg/Litre, and Erythrocyte Sedimentation Rate (ESR) was 46 mm/1 hr. The patient was started on antibiotics, vasopressor, and other supportive therapy, including corticosteroid and anticoagulant. The patient’s endotracheal aspirate was sent for Cartridge Based Nucleic Acid Amplification (CBNAAT) testing, which detected M. TB complex in low concentration, and rifampicin resistance was absent. It was negative for malignant cells. However, the patient deteriorated and succumbed to his illness within twenty-four hours of admission.
Discussion
Our patient was a case of carcinoma of the larynx, having received chemo-radiotherapy for the same, in a known case of diabetes mellitus, systemic hypertension and peyronie's disease with recently diagnosed microbiologically confirmed pulmonary TB with probable addisonian crisis. The presence of comorbidities viz. diabetes, systemic hypertension and peyronie's disease with a prior history of malignancy having received chemo-radiotherapy, extensive bilateral pulmonary radiological involvement of tuberculosis at presentation & delayed seeking of healthcare advice eventually contributed to the unfortunate poor outcome of the patient. The history of symptoms since three months reflected the delayed presentation of the patient to the healthcare system. Diabetes alone has been associated with poor treatment outcomes in tuberculosis [2]. The presence of lymphopenia (Lymphocytes: 9%) suggested the immunocompromised condition of the patient at presentation. This could potentially be related to the chemo-radiotherapy that the patient had received for cancer treatment in the past [3,4]. The pulmonary parenchyma, pleura, airways, pulmonary vascular system, mediastinum, or the neuromuscular system that controls breathing can all be affected by chemotherapy-induced lung damage [5].
Our patient had lymphopenia. Lymphopenia in cancer patients might be functional or caused by treatment [4]. Because lymphocytes are essential in the anti-tumour immune response; cancer treatments can typically suppress reservoir lymphoid organs, resulting in lymphopenia, linked to an increased risk of opportunistic infections and worse oncologic outcomes. Although Chemotherapy (CT) is the most common cause of Haematological Toxicity (HT), radiotherapy also contributes to hematologic cell line damage. Lymphocytes are particularly radiosensitive, and their number decreases exponentially as irradiation progresses. In the covid pandemic, the pro-inflammatory micro-environment can also cause lymphocyte deficiency by apoptosis, compromising immune-homeostasis and inflammatory-response in individuals with covid-19 infection. Lymphopenia is a crucial predictor of severe COVID-19. A lymphocyte count <1.5 × 10/L has been linked to a three-fold increased risk of severe COVID-19 [3]. All lymphocyte subpopulations are suppressed significantly and for a long time after Radiotherapy (RT) alone or radiotherapy with concurrent chemotherapy with cisplatin (RT-CHT). RT-CHT, but not RT alone, causes NK-cells and T-suppressor cells to be suppressed for a long time [6].
Natural Killer (NK) cells and macrophages are essential components of the body's innate immune system, and they play a key role in the body's ability to limit M.TB growth synergistically in immuno-compromised people who don't have a sufficient T cell response. The secretory products perforin, granulysin, and granzymes and numerous membrane-bound death receptors that permit target guided lysis are mostly responsible for direct control mechanisms. NK cells also play a role in indirectly generating an immune response by activating macrophages and monocytes through a variety of signalling pathways that include both reactive oxygen species and reactive nitrogen species.7 NK cells help limit mycobacterial growth by helping in the death of M.TB-infected cells via degranulation. In TB patients, NK cells show significant declines in interferon expression and degranulation [8].
Active TB is more likely to occur in those who have cancer. This is likely due to both intrinsic immunosuppression caused by cancer and the immunosuppressive effects of chemotherapy and other host variables that may increase cancer and TB susceptibility [9]. Reactivation of TB occurs in immunocompromised persons. Therefore, before starting radiation or chemotherapy for solid-tumour malignancy, patients with solid organ malignancy should be screened for LTBI with either a tuberculin skin test or an interferon-gamma release assay (IGRA) from whole blood [10]. Lung cancer, oesophageal cancer, pancreatic cancer, hematologic malignancy, and head and neck cancer patients are at an increased risk of contracting TB. These patients with high-risk cancers should mainly be targeted for LTBI screening and treatment [1]. The compliance of TB preventive therapy in immunocompromised patients like people living with Human immunodeficiency virus (PLHIV) already on antiretroviral therapy has been demonstrated to be good [11]. Similarly, both anti-cancer and anti TB medications can be safely administered in patients with malignancy [12]. Thus, immunocompromised patients like those with malignancy should be considered for targeted LTBI treatment before or with the initiation of chemoradiotherapy for the same and drug interactions, adverse drug reactions or compliance should not be a hindrance in these patients, but should be closely monitored for in them. The World Health Organisation (WHO) maintains that evidence on the risks of at-risk populations like cancer patients for progression from LTBI to active disease is crucial for determining the potential benefits of LTBI treatment and designing appropriate public health interventions [13]. With the current lack of high-quality evidence, the WHO has not recommended the mandatory screening and treatment of LTBI in cancer patients. Future research for evidence-based recommendations on LTBI diagnosis and treatment in cancer patients is the need of the hour.
Conclusion
To prevent increased morbidity and death in these cancer patients, clinicians must be aware of and include active TB disease in the differential diagnosis of pulmonary toxicity suspected in a patient undergoing chemotherapy with unexplained pulmonary symptoms [5]. Reactivation of TB can be potentially eliminated with thorough and consistent screening efforts for LTBI and initiating treatment for the same at the time of initiation of treatment for malignancy [10].
References
- Cheon J, Kim C, Park EJ, Ock M, Lee H, Ahn JJ, et al. Active tuberculosis risk associated with malignancies: an 18-year retrospective cohort study in Korea. J Thorac Dis. 2020; 12: 4950.
- Mishra G, Munje R, Dawkore M. Diabetes and Tuberculosis – Tackling Double Trouble. Indian J Basic Appl Med Res. 2018; 8: 256–60.
- Iorio GC, Ricardi U, Dal Pra A. Radiation-Induced Lymphopenia Beyond the COVID-19 Pandemic. Front Oncol. 2020; 18–20.
- Patil VM, Singh GK, Noronha V, Joshi A, Menon N, Lashkar SG, et al. Lymphopenia during chemoradiation-foe or friend. Ecancermedicalscience. 2020; 1–11.
- Ahmed G, Saif MW. Pulmonary Tuberculosis Versus Recurrent Chemotherapy-Induced Pneumonitis: A Clinical Dilemma. Cureus. 2017; 9: e1742.
- Bachtiary B, Herbacek I, Zideck T, Knocke TH, Dimopoulos J, Poetter R, et al. Impact of radiotherapy with and without concurrent cisplatin on lymphocyte subpopulations in cervical cancer patients. Anticancer Res. 2005; 25: 4673–8.
- Allen M, Bailey C, Cahatol I, Dodge L, Yim J, Kassissa C, et al. Mechanisms of Control of Mycobacterium tuberculosis by NK Cells: Role of Glutathione. Front Immunol. 2015; 508.
- Garand M, Goodier M, Owolabi O, Donkor S, Kampmann B, Sutherland JS. Functional and Phenotypic Changes of Natural Killer Cells in Whole Blood during Mycobacterium tuberculosis Infection and Disease. Front Immunol. 2018; 9: 257.
- Cheng MP, Chakra CNA, Yansouni CP, Cnossen S, Shrier I, et al. Risk of active tuberculosis in patients with cancer: A systematic review and metaanalysis. Clin Infect Dis. 2017; 64: 635–44.
- Jacobs REA, Gu P, Chachoua A. Reactivation of pulmonary tuberculosis during cancer treatment. Int J Mycobacteriology. 2015; 4: 337–40.
- Mishra G. High compliance of six-month INH preventive therapy in HIV patients: A stepping stone for the future. IP Indian J Immunol Respir Med. 2019; 4: 161–3.
- Chai M, Shi Q. The effect of anti-cancer and anti-tuberculosis treatments in lung cancer patients with active tuberculosis: a retrospective analysis. BMC Cancer. 2020; 20: 1–7.
- World Health Organisation. Latent TB Infection : Updated and consolidated guidelines for programmatic management. Geneva, Switzerland. 2018.