
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Anesthetic management “Abdominal Aortic Aneurysm” in the well-known case with Wolff-Parkinson-White syndrome
Sogol Asgari1; Arash Tafrishinejed1; Faranak Behnaz2*
1 Assistant Professor, Department of Anesthesiology, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2 Associate Professor, Department of Anesthesiology, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Faranak Behnaz
Associate Professor, Anesthesiology Department.
Shohada-e-Tajrish Hospital, Shahid Beheshti University
of Medical Sciences, Tehran, Iran.
Email: Faranak.Behnaz@gmail.com
Received : Aug 23, 2021
Accepted : Sep 24, 2021
Published : Oct 01, 2021
Archived : www.jcimcr.org
Copyright : © Behnaz F (2021).
Abstract
Wolff-Parkinson-White syndrome is an electrophysiological disorder of the heart caused by pre-stimulation of an abnormal lateral pathway that can be asymptomatic or may be accompanied by palpitations or shortness of breath. We reported a case of a 66-yearold man with a history of Wolff-Parkinson syndrome who was transferred to the operating room for simultaneous nephrectomy due to RCC and abdominal aortic aneurysm. Managing the anesthesia of these patients is challenging because they are prone to life-threatening tachyarrhythmias. Observance of all necessary precautions to prevent tachyarrhythmias, balanced anesthesia, careful monitoring and preparation with the necessary drugs and equipment to treat any complication, is the cornerstone of a positive surgical outcome.
Keywords: Wolff Parkinson white syndrome; abdominal aortic aneurysm; electrophysiological disorder; anesthetic management.
Citation: Asgari S, Tafrishinejed A, Behnaz F. Anesthetic management “Abdominal Aortic Aneurysm” in the well-known case with Wolff-Parkinson-White syndrome. J Clin Images Med Case Rep. 2021; 2(5): 1338.
Introduction
Wolff-Parkinson-White syndrome (WPW) is caused by prestimulation of an abnormal lateral pathway between the atrium and ventricle by crossing the normal atrioventricular pathway. The incidence rate is 0.9-3% of the general population [1]. Diagnosis is made by history and Electrocardiography (ECG), which shows a shorter PR interval, wider delta waves and wider QRS [2]. Patients may be asymptomatic or may have palpitations or Due to changes in the physiology of conduction by anesthetics and cardiovascular changes due to the response to surgical stress and the effects of pneumoperitoneum, life-threatening tachyarrhythmias may occur, so it is important to consider this in the case of preoperative management [3]. Nearly all anesthetics have different effects on the conduction system of the heart. In addition, invasive interventions and surgery exacerbate sympathetic stimulation. Therefore, the main goal of anesthesiologists is to manage postoperative anesthesia in patients with the syndrome [4]. WPW should prevent sympathetic stimulation and prevent tachyarrhythmias [5].
Patients with WPW are prone to sympathetic activity. Therefore, these patients are at risk for fatal postoperative arrhythmias [4]. All precautions should be taken to prevent and treat postoperative tachyarrhythmias. In patients with stable hemodynamics, supraventricular tachyarrhythmias can be medically treated with drugs such as adenosine, phenylephrine and betablockers [6]. However, cardiac ablation is necessary if the patient is hemodynamically unstable. To prevent elevated blood catecholamine levels in the postoperative period, preferential anesthetics should have minimal hemodynamic effects. Accordingly, the use of regional anesthesia techniques will be useful to reduce sympathetic activity [7]. However, if general anesthesia is the choice, the supraglottic airway is recommended to prevent stress response to laryngoscopy and intubation if possible [8]. In our patient, general anesthesia was considered according to the type of surgery.
Case presentation
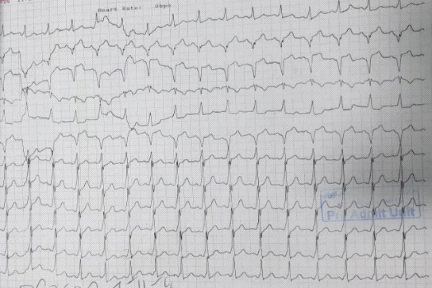
A 66-year-old man with 75 kg presented for simultaneous nephrectomy due to RCC and abdominal aortic aneurysm. The patient has a history of WPW heart disease but does not complain of chest pain, palpitations, and exercise-induced shortness of breath. He also has no history of other diseases such as hypertension and diabetes. He does not take any medicine and has not been referred for a heart examination. His general and systemic examination was normal with a regular heart rate of 85 beats per minute and a blood pressure of 125/80 mm Hg. However, his ECG shows a shortening of the PR distance and the “Delta” wave (Figure 1). Echocardiography showed grade I LV diastolic dysfunction and EF = 55%.
In the operating room, standard monitors were attached. Before anesthesia, an epidural catheter was inserted to control postoperative pain. Under local anesthesia with 2% lidocaine, arterial catheterization of the radial artery and central right jugular venous catheter were implanted. A defibrillator with Adenosine, Osmolol, lidocaine, Procainamide and Amiodarone was placed on the patient's bedside. The patient was preoxygenated with 100% oxygen for 3 minutes. Premedication with midazolam 2.5 mg IV Fentanyl 200 μg was given in the titrate, then induction of anesthesia with 100 mg Propofol and 40 mg Atracurium was given. After intubation, a slight increase in heart rate and blood pressure was observed, and on the ECG, "Delta waves" were prominent. Anesthesia was maintained by injecting propofol at a rate of 200-100 μg / kg / min. Vital signs were stable during the operation (HR = 85 / min IBP = 120/65 mmHg ETCO2 = 35). After surgery, the patient was reversed and extubated by spontaneous breathing, then and transferred to recovery conscious awakening.
Discussion
Many cases of WPW syndrome are described as asymptomatic, but such patients are always at risk for recurrent tachyarrhythmias, even ventricular fibrillation, and sudden death during the postoperative period [1]. The lateral conduction pathway between the atria and the ventricle allows electrical conduction at a site other than the AV node. Medications and anesthesia techniques further alter the physiology of AV conduction. The goal of postoperative anesthesia is to prevent increased sympathetic pressure from pain, anxiety, intubation stress response, and intubation reflex, light anesthesia, and hypovolemia. Propofol is preferred because it has no side effects. Isoflurane and sevoflurane also have no effect on AV node conduction and provide the desired hemodynamic status. Fentanyl provides adequate hemodynamic stability. Muscle relaxants that have better cardiac stability, such as Vecuronium and Rocuronium, are preferred to Pancuronium and Atracurium [2]. Propofol is thought to be a suitable anesthetic for these patients. Although studies have been conducted on the idea that propofol has no direct effect on Sinus Node (SA), AV node, and cardiac conduction, a recent study suggested that cardiac conduction could be suppressed with propofol [3]. Nesdonal is considered safe, but has negative hemodynamic effects. Ketamine should be avoided due to sympathetic stimulation. Etomidate may be preferred due to its ability to maintain a stable cardiovascular profile. Volatile anesthetic agents have different effects on the cardiac conduction system. Volatile anesthetics may cause dysrhythmias or act as class III antiarrhythmics [6]. Among the volatile agents, sevoflurane has been shown to have no effect on SA node, AV conduction in adult patients with WPW syndrome. And sevoflurane can be used without any side effects [2]. In the case of narcotics, it is best to avoid pethidine because of its atropine-like effect. Alfentanil, Sufentanil and Fentanyl do not have any effect on the refractory period of AP [9]. Remifentanil may inhibit both atrial and sinus node conduction, but does not affect conduction through the AV node. Also, the combination of Fentanyl and Propofol has been shown to increase cardiac vagal tone [10].
Muscle relaxants, Succinylcholine, have an arrhythmogenic effect on the heart. Among non-depolarized muscle relaxants, Atracurium may cause autonomic instability due to the release of histamine, and Pancuronium may stimulate supraventricular tachycardia by accelerating AV conduction and heart rate. Rocuronium, Vecuronium and Cisatracurium may be better options for general anesthesia. Reverse musculoskeletal block is a challenge for anesthesiologists. The combination of anticholinesterase and anticholinergic drugs may cause severe arrhythmias. Atrial fibrillation with a broad QRS complex has been reported after neostigmine administration in a patient with WPW syndrome [2]. Atropine and glycopyrrolate lead to tachycardia. Studies have reported the use of Shogamadex for the reversal of safe neuromuscular block [11,12].
Supraventricular tachycardia during anesthesia should be controlled by cardioversion or medication depending on hemodynamic stability. Vagal maneuvers can be tried. The preferred drugs are lidocaine, adenosine, and class I beta-blockers. Antiarrhythmic drugs such as Digoxin and Verapamil should be avoided because they may increase anterograde conduction through a lateral pathway [3]. American Heart Association Recommends the use of propranolol Metoprolol has also been recommended for adenosine failure to control arrhythmias. In case of AF, procaine amide and propranolol are useful and verapamil and digoxin should be avoided [3,4].
Purpose of WPW Anesthesia Management: Hypovolemia, hypoxia, hypothermia, hypotension and tachycardia should be avoided. In case of hypotension, phenylephrine is useful [4].
To conclude, patients with WPW syndrome undergoing surgery can be well controlled under general anesthesia with adequate precautions to prevent and manage arrhythmias.
Conclusion
Wolff-Parkinson-White syndrome is an electrophysiological disorder of the heart caused by pre-stimulation of an abnormal lateral pathway that can be asymptomatic or may be accompanied by palpitations or shortness of breath. Due to changes in the physiology of conduction by anesthetics and cardiovascular changes due to surgical stress response, life-threatening tachyarrhythmias may occur. Therefore, the goal in anesthesia is to avoid sympathetic stimulation, hemodynamic stability, and prevent arrhythmia. Drug treatment or ablation and stabilization of the patient before surgery is necessary. These patients are also at risk of sudden death after surgery, so postoperative care is important
Acknowledgements: The authors would like to acknowledge the kind support of all physicians and nurses, Shohada-e Tajrish Hospital, Tehran, Iran.
Ethical approval: Written informed consent was obtained from the patient for the publication of this case report.
References
- Kabade SD, Sheikh S, Periyadka B. Anaesthetic management of a case of Wolff-Parkinson-White syndrome. Indian journal of anaesthesia. 2011; 55: 381.
- Kiran Kumar KC, Hyoju S, Raya P. Anesthetic Management of a Patient with Wolff-Parkinson-White Syndrome for Laparoscopic Cholecystectomy: A Case Report. JNMA: Journal of the Nepal Medical Association. 2020; 58: 699.
- Leung LW, Gallagher MM. Review paper on WPW and athletes: Let sleeping dogs lie? Clinical Cardiology. 2020; 43: 897-905.
- Aytuluk HG. Infraclavicular Brachial Plexus Block and Sugammadex Use in a Paediatric Patient with Wolff–Parkinson–-White Syndrome. Romanian Journal of Anaesthesia and Intensive Care. 2020; 27: 19-22.
- Nisar P, Rajadhyaksha N. Anesthetic Challenges in the Management of Parturient with Wolff-Parkinson-White Syndrome Posted for Elective Cesarean Section. Journal of Clinical Research in Anesthesiology. 2020; 3: 1-3.
- Bengali R, Wellens HJ, Jiang Y. Perioperative management of the Wolff-Parkinson-White syndrome. Journal of cardiothoracic and vascular anesthesia. 2014; 28: 1375-86.
- Staikou C, Stamelos M, Stavroulakis E. Perioperative management of patients with pre-excitation syndromes. Romanian journal of anaesthesia and intensive care. 2018; 25: 131.
- Sato Y, Nagata H, Inoda A, Miura H, Watanabe Y, Suzuki K. Cardioversion for paroxysmal supraventricular tachycardia during lung surgery in a patient with concealed Wolff-Parkinson-White syndrome. Masui. The Japanese journal of anesthesiology. 2014; 63: 1106-10.
- Udaybhaskar V, Sreemayee C, Ingley P. Wolff–Parkinson–White syndrome: Implications for an anaesthesiologist. Journal of Neuroanaesthesiology and Critical Care. 2017; 4: 049-52.
- Sabuncu Ü, Yağar S, Yömen Vy. Normalization of Electrocardiography Pattern Due to Anesthesia in a Patient with Wolff-Parkinson-White Syndrome During Non-Cardiac Surgery. Turkiye Klinikleri J Cardiovasc Sci. 2018; 30: 82-5.
- Strawbridge AR, Connor T, Liu M. Sugammadex Reversal in the Anesthetic Management of Wolff-Parkinson-White. 59 MDW San Antonio United States. 2019.
- Şahin SH, Öztekin İ, Kuzucuoğlu A, Aslanoğlu A. Sugammadex use in a patient with Wolff-Parkinson-White (WPW) Syndrome. Balkan medical journal. 2015; 32: 327.