
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Type A aortic dissection in a young 37 weeks pregnant lady successfully treated by Bentall procedure: A case report
Rehan Shahid1; Adnan Izhar1; Ali Husnain2*; Anum Sohail2; Muhammad Umar Hassan2; Maham Mushtaq2; Faizan Liaqat Ch3
1 Punjab Institute of Cardiology, Lahore, Pakistan.
2 King Edward Medical University, Lahore, Pakistan.
3 Ameer ud din Medical College, Lahore, Pakistan.
*Corresponding Author: Ali Husnain
Street No. 10, Madina Town, Housing colony, Nankana
Sahib, Pakistan.
Email: alihusnain9292@gmail.com
Received : Aug 28, 2021
Accepted : Sep 27, 2021
Published : Oct 04, 2021
Archived : www.jcimcr.org
Copyright : © Husnain A (2021).
Citation: Shahid R, Izhar A, Husnain A, Sohail A, Hassan MU, et al. Type A aortic dissection in a young 37 weeks pregnant lady successfully treated by bentall procedure: A case report. J Clin Images Med Case Rep. 2021; 2(5): 1340.
Introduction
Aortic dissection is intimal tear in aorta and collection of blood in between the layers of aortic wall. The incidence of acute type A aortic dissection is between 2.1 and 16.3 per 100,000 persons [1]. Aortic dissection is an infrequent but potentially life threatening complication of pregnancy with most of the cases occurring in third trimester and post-partum period [2]. The most important predisposing factors to aortic dissection are Marfan, Ehlers-Danlos, Turner and Loeys-Dietz syndromes [3]. However, the non sporadic cases can also occur in pregnancy [4].
In non sporadic cases, pregnancy itself predisposes to development of aortic dissection due to several physiologic hormonal and blood pressure changes. Still, the incidence of aortic dissection is very low in pregnancy with a study reporting it to be nearly 0.0004% [5]. Though aortic dissection is rare in pregnancy, its urgent treatment is mandatory due to very high risk of maternal and fetal death. The mortality rate increases 1 to 2% every hour in the first 48 hours if the necessary intervention is not done [6]. Bentall procedure is a surgical modality to repair aortic root and ascending aortic arch anomalies such as aneurysms and dissections. It is the treatment of choice for treating proximal aortic dissection [7].
Cases of successful treatments of postpartum and early pregnancy aortic dissections have been reported around the world. However, there are a very few case reports of successful management of aortic dissections in third trimester or nearterm pregnancy. Here are the details of first of its kind case in our tertiary care hospital.
Case presentation
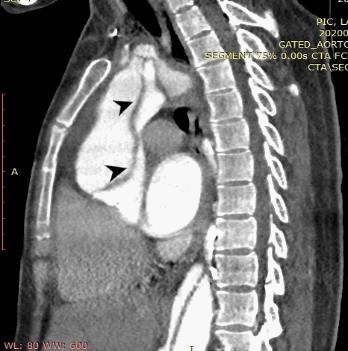
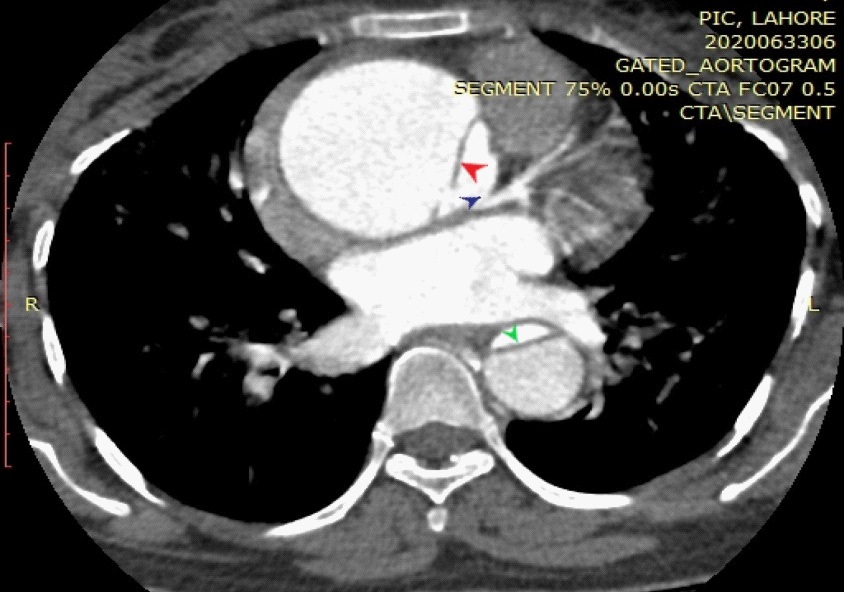
A 31 years old 37 weeks pregnant primagravida female presented to emergency department of Punjab Institute of Cardiology, Lahore, Pakistan with presenting complaints of shortness of breath and severe chest pain radiating towards back. Blood pressure at the time of presentation was 130/90 mmHg with heart rate of 108/min. Respiratory rate of patient was 23/min and temperature was noted to be 98.2° F. The abdomen was distended and consistent with age of fetus. There were no visible abdominal pulsations. Auscultation of chest revealed normal first and second heart sounds with a diastolic murmur. ECG showed regular sinus rhythm with no notable abnormalities in all leads. Lab reports of the patient were non-significant with normal values of CBC, electrolytes, cardiac markers, LFTs and RFTs. Echocardiography was done which revealed aortic dissection flap. Aortic dissection was suspected but the surgical team needed contrast enhanced CT aortogram for confirming the diagnosis. The risk of contrast infusion was duly explained to the patient and her husband. After informed consent, CT aortography was done which confirmed the diagnosis (Figure 1,2).
For multidisciplinary approach, obstetrics and gynecology colleagues were involved in the management of this patient. They performed an emergency C section and heathy baby was delivered. After that patient was shifted to cardiac surgery and remained ventilated overnight.
After taking informed consent from her husband, our surgical team proceeded for bentall procedure to repair aortic dissection. Under general anesthesia femoral vessels were exposed and femoral cannulation was done. After sternotomy right atrial cannulation was done and patient was shifted to cardiopulmonary bypass machine. Aorta was clamped proximal to the origin of neck vessels. After aortotomy, antegrade cardioplegia was given. Dissection flap was noted arising from sinotubular junction. Aortic valve along with area of dissection was excised and coronary buttons were mobilized. On-X 21 mm aortic root prosthesis was applied and coronary buttons were re-attached. On deep hypothermic circulatory arrest distal anastomosis was done. After securing hemostasis, patient was shifted off from cardiopulmonary bypass machine. Two mediastinal drains were placed and routine closure was done. Patient stayed in ICU for 3 days and recovered uneventfully. Patient was discharged from hospital at 7th post-operative day in stable condition. One month follow up was highly encouraging for the surgical team as the patient was living a normal healthy life without any sort of complications.
Discussion
Acute aortic dissection is responsible for nearly 14% of the maternal mortalities in pregnancy, usually in the third trimester. The mortality risk increases to upto 80% within 2 weeks of presentation [8]. Mean age of presentation during pregnancy is 31 years and patients usually present with unexplained chest or epigastric abdominal pain often radiating to back [9]. The risk factors responsible for aortic dissection in pregnant women are Marfan syndrome, bicuspid aortic valve, dilated aortic root, hypertension, pre-eclampsia and also pregnancy itself is considered a major risk factor for aortic dissection. Those patients having aortic diameter less than 4.0 mm have less than 1% risk of develop aortic dissection and risk increases with increasing diameter. Type A dissections are more common (79%-89%). The reported mortality is higher in type B dissections [10]. Stanford type A dissection was seen in our case.
European guidelines suggest that women with Marfan syndrome should not become pregnant with aortic diameter >4.5 cm. Aortic wall remodeling is the major event occurring in pregnancy primarily due to hormones and angiogenic factors. This remodeling predisposes to development of fatal aortic dissection even in the absence of any other connective tissue disorders. The safest time to perform surgery in high risk patients is second trimester but emergency surgery can be done in any trimester [11].
The management approach in patients with high risk factors is multidisciplinary. Team of specialists from cardiology, cardiac surgery, anesthesiology, pediatrics, obstetrics and gynecology departments should be there to manage the case. During pregnancy, pregnant ladies should undergo echocardiography monthly or bimonthly. MRI without contrast is recommended but CT aortography is the investigation of choice in urgent cases to avoid radiation exposure and due to its rapid availability. Genetic prenatal testing can be performed in cases of a positive family history of aortic dissection [12]. The use of contrast in pregnancy is largely debatable. The contrast fluid being a category B pregnancy drug is mostly avoided in pregnancy. However, in emergent conditions such as aortic dissection, the benefit is believed to outweigh the risks and can be used for diagnosis [13]. In our case, contrast enhanced CT aortogram was done.
Gestational age and type of aortic dissection is responsible for considering surgery. Before 28 weeks, surgical repair is performed with continuation of pregnancy. Between 28 and 32 week, C section depends on mother and fetus condition. After 32 weeks, C section along with surgical aortic dissection repair is offered to the patient [14]. Hysterectomy is indicated with peripartal haemorrhage occurring after surgery but it carries poor prognosis so only recommended in selected cases [12]. With hemodynamically stable patients, C section is to be performed first otherwise aortic surgery is performed in unstable patients and it carries the greater risk of maternal and fetal mortality [15]. Different methods are available to treat aortic dissection. The choice of procedure depends upon the type of aortic dissection and the extent of involvement of aorta. Bentall procedure, Cabrol technique and ‘button’ techniques are various options available for treatment of ascending aortic dissections [16]. Bentall procedure with repairing of coronary ostia by ‘button’ technique was done in our case and outcomes were highly desirable.
Conclusion
Aortic dissection is a rare complication of pregnancy. Several congenital syndromes predispose to aortic dissection. However, non sporadic cases can also develop due to pregnancy being an independent risk factor. In fatal emergent conditions, contrast enhanced CT is preferable choice of diagnosis. Through Multidisciplinary approach this case was managed and C section and Bentall procedure were performed. Bentall procedure proves to be a life saving procedure for acute type A aortic dissection.
References
- Wundram M, Falk V, Eulert-Grehn JJ, Herbst H, Thurau J, Leidel BA, Göncz E, Bauer W, Habazettl H, Kurz SD. Incidence of acute type A aortic dissection in emergency departments. Sci Rep. 2020; 10: 7434.
- Yuan SM. Postpartum aortic dissection. Taiwan J Obstet Gynecol. 2013; 52: 318-22.
- Silvestri V, Mazzesi G, Mele R. Postpartum aortic dissection. A case report and review of literature. International journal of surgery case reports. 2019; 56: 101–106.
- Mariscalco G, Debiec R, Elefteriades JA, Samani NJ, Murphy GJ. Systematic review of studies that have evaluated screening tests in relatives of patients affected by nonsyndromic thoracic aortic disease. Journal of the American Heart Association. 2018; 7: e009302.
- Zhu JM, Ma WG, Peterss S, Wang LF, Qiao ZY, et al. Aortic dissection in pregnancy: management strategy and outcomes. The Annals of thoracic surgery. 2017; 103: 1199-1206.
- Tsai TT, Nienaber CA, Eagle KA. Acute aortic syndromes. Circulation. 2005; 112: 3802–13.
- Cherry C, DeBord S, Hickey C. The modified Bentall procedure for aortic root replacement. AORN J. 2006; 84: 52-5.
- Johnston C, Schroeder F, Fletcher SN, Bigham C, Wendler R. Type A aortic dissection in pregnancy.Int J Obstet Anesth. 2021; 21: 75-97.
- Sawlani N, Shroff A, Vidovich MI. Aortic dissection and mortality associated with pregnancy in the United States. J Am Coll Cardiol. 2015; 65: 1600-1.
- Lee SH, Ryu S, Choi SW, Kim HJ, Kang TK, et al. Acute Type A Aortic Dissection in a 37-Week Pregnant Patient: An Unusual Clinical Presentation. J Emerg Med. 2017; 52: 565-568.
- Lansman SL, Goldberg JB, Kai M, Tang GH, Malekan R, et al. Aortic surgery in pregnancy. J Thorac Cardiovasc Surg. 2017; 153: S44-S48.
- Poniedzialek-Czajkowska E, Sadowska A, Mierzynski R, Leszczynska-Gorzelak B. Aortic dissection during pregnancy - obstetric perspective. Ginekol Pol. 2019; 90: 346-350.
- Abo-Salem E, López-Candales A. Diagnosis of asymptomatic aortic dissection during pregnancy using contrast echocardiography. Journal of cardiology cases. 2014; 9: 200-202.
- Akhmerov A, D’Attellis N, Shah AS. Successful Outcomes following Repair of a Type A Aortic Dissection during Pregnancy. Aorta (Stamford). 2020; 8: 14-17.
- Sumiyoshi R, Morita H, Fujii K, Shirasughi T, Kawaura H, et al. A patient with Marfan’s syndrome who developed an acute aortic dissection at 28 weeks of pregnancy treated with aortic root replacement. Gen Thorac Cardiovasc Surg. 2021.
- Bachet J, Termignon JL, Goudot B, et al. Aortic root replacement with a composite graft. Factors influencing immediate and longterm results. European Journal of Cardio-thoracic Surgery: Official Journal of the European Association for Cardio-thoracic Surgery. 1996; 10: 207-213.