
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Dramatic demise of a pregnant woman in third trimester after presenting with persistent headache: An iatrogenic
Islam Tarek Elkhateb1*; Mennah Hisham Aldamsisi2; Abdalla Mousa3
1 Department of Obstetrics & Gynecology, New Giza University School of Medicine, Egypt.
2 New Giza University School of Medicine, Egypt.
3 Department of Obstetrics & Gynecology, Kasr Alainy Hospital, Cairo University, Egypt.
*Corresponding Author: Islam Tarek Elkhateb
Department of Obstetrics & Gynecology, Room 2.7.
Building A, School of medicine, New Giza University.
New Giza, Km 22 Cairo-Alex Road, Giza, Egypt.
Email: islamtarekhamed@gmail.com
Received : Aug 25, 2021
Accepted : Sep 30, 2021
Published : Oct 07, 2021
Archived : www.jcimcr.org
Copyright : © Elkhateb IT (2021).
Abstract
A 31-years-old patient, pregnant at 32 weeks of gestation presented to our triage unit with complaint of gradually progressive persistent headache that started 1 day earlier and was unresponsive to all analgesics. Her history was insignificant for any major medical or surgical events and the pregnancy course was smooth as well. Her lab results and obstetric ultrasound were reassuring. During magnetic resonance imaging examination, the patient suddenly deteriorated after giving her an inhalational anaesthesia for sedation. She became unconscious. She was intubated, mechanically ventilated, and put-on cardiovascular support. Brain imaging then revealed Brain Stem (BS) herniation and diffuse brain oedema. She was announced dead with intrauterine foetal death. A late diagnosis of cerebral venous thrombosis was established. This caused BS herniation through increased intracranial pressure, which was iatrogenically augmented by administering inhalation anaesthesia.
Keywords: cerebral vein; thrombosi; thrombophilia; pregnancy; headache; magnetic resonance imaging; brain stem herniation.
Citation: Elkhateb IT, Aldamsisi MH, Mousa A. Dramatic demise of a pregnant woman in third trimester after presenting with persistent headache: An iatrogenic. J Clin Images Med Case Rep. 2021; 2(5): 1346.
Background
Headache is a very common complaint that is encountered by almost 60% of women in their childbearing age. Secondary headache is a type of headache that is due to an underlying medical condition. Headaches with new/subacute onset, persisting course, or not responding to analgesics suggest serious underlying disorder that require urgent management. Preeclampsia is the most common cause of new onset as well as secondary headache seen in pregnant women after 20 weeks of gestation [1]. Pregnancy is a physiological pro-coagulant state that poses an increased risk of thrombosis. Cerebral venous thrombosis (CVT) is a very rare but serious disease that presents essentially with headache [2].
Case presentation
A 31-year-old, gravida 2, para 1, with one living offspring born secondary to an elective caesarean section (CS) presented to the triage unit of our hospital with a complaint of persistent headache that had an acute onset 28 hours earlier. Headache became worse from 7 hours and she vomited twice since then. Headache was generalized and unresponsive to analgesics. It was associated with mild nausea and blurry vision. The patient was pregnant at +/- 32 weeks of gestation with smooth uneventful pregnancy course. Her past history was insignificant for any chronic or pregnancy induced medical disorder. No history of major abdominal surgeries or known drug allergies. She used to attend to her regular antenatal care visits and take antenatal vitamins. Patient was fully conscious, alert, and oriented. Her blood pressure (BP) was normal at 110/70 with no albuminuria by urine strips. Her fundal level corresponded to 32 weeks gestation.
Investigations
Bedside obstetric Ultrasound (US) revealed a single living foetus, appropriate for gestational age, with average liquor, and normal placenta. Routine labs were done in the form of: Complete Blood Count (CBC), Renal Function Tests (RFTs), Liver Function Test (LFTs), coagulation profile, and electrolytes. Cardiac enzymes were requested by the Emergency Medicine (EM) registrar. All labs came back within normal ranges for a gravid female in the third trimester, except for mild anaemia (Table 1).
Table 1:Laboratory work up done and test results.
laboratory test |
Result |
Reference value |
||
LFTs& RFTs |
ALT (IU/L) |
21 |
(10- 45) |
|
AST (IU/L) |
21 |
< 35 |
||
Direct bilirubin (mg/dl) |
0.1 |
< 0.2 |
||
Total bilirubin (mg/dL) |
0.4 |
(0.3- 1.2) |
||
ALP (U/L) |
130 |
(30- 120) |
||
Serum total protein (g/dL) |
6 |
(5.6- 7.2) |
||
Albumin (g/dL) |
3.2 |
(2.5- 5.2) |
||
A\G ratio |
1.14 |
(1- 2) |
||
Urea (mg/dL) |
27 |
(17- 43) |
||
Creatinine (mg/dL) |
0.55 |
(0.5- 0.9) |
||
Uric acid (mg/dl) |
4.5 |
(2.6- 6) |
||
Electrolytes and cardiac enzymes |
Na (mmol/ L) |
137 |
(134- 146) |
|
K (mmol/ L) |
3.7 |
(3.5- 5.1) |
||
Total Ca (mg/dl) |
8.1 |
(8.2- 9.7) |
||
Ionized Ca (mmol/ L) |
1.1 |
(1.1- 1.3) |
||
Ph (mg/dl) |
2.8 |
(2.5- 4.5) |
||
Mg (mg/dl) |
2 |
(1.9- 2.5) |
||
Creatinine kinase (CK) total (U/L) |
90 |
<145 |
||
CK- myocardial band (MB) (U/L) |
19 |
<24 |
||
Highly sensitive troponin T (pg/ml) |
3.2 |
<5: low risk |
||
CBC |
Hb (gm/dL) |
9.4 |
(9.5- 13) |
|
HCT (%) |
28.9 |
(28- 39) |
||
TLC (K/µL) |
11.37 |
(5.6- 16) |
||
PLT (K/µL) |
176 |
(150- 400) |
||
INR |
|
0.93 |
≤1 |
|
Treatment
We did not give any treatment till then, except for analgesics and narcotics with no improvement.
Outcome
As the patient became drowsy with no improvement in headache, neurology registrar was called for assessment. He evaluated the patient as having a Glasgow Coma Scale (GCS) of 13. She had normal motor examination, sensory examination, and intact reflexes. He ordered a Magnetic Resonance Imaging (MRI) with Magnetic Resonance Arteriography (MRA) and Magnetic Resonance Venography (MRV).
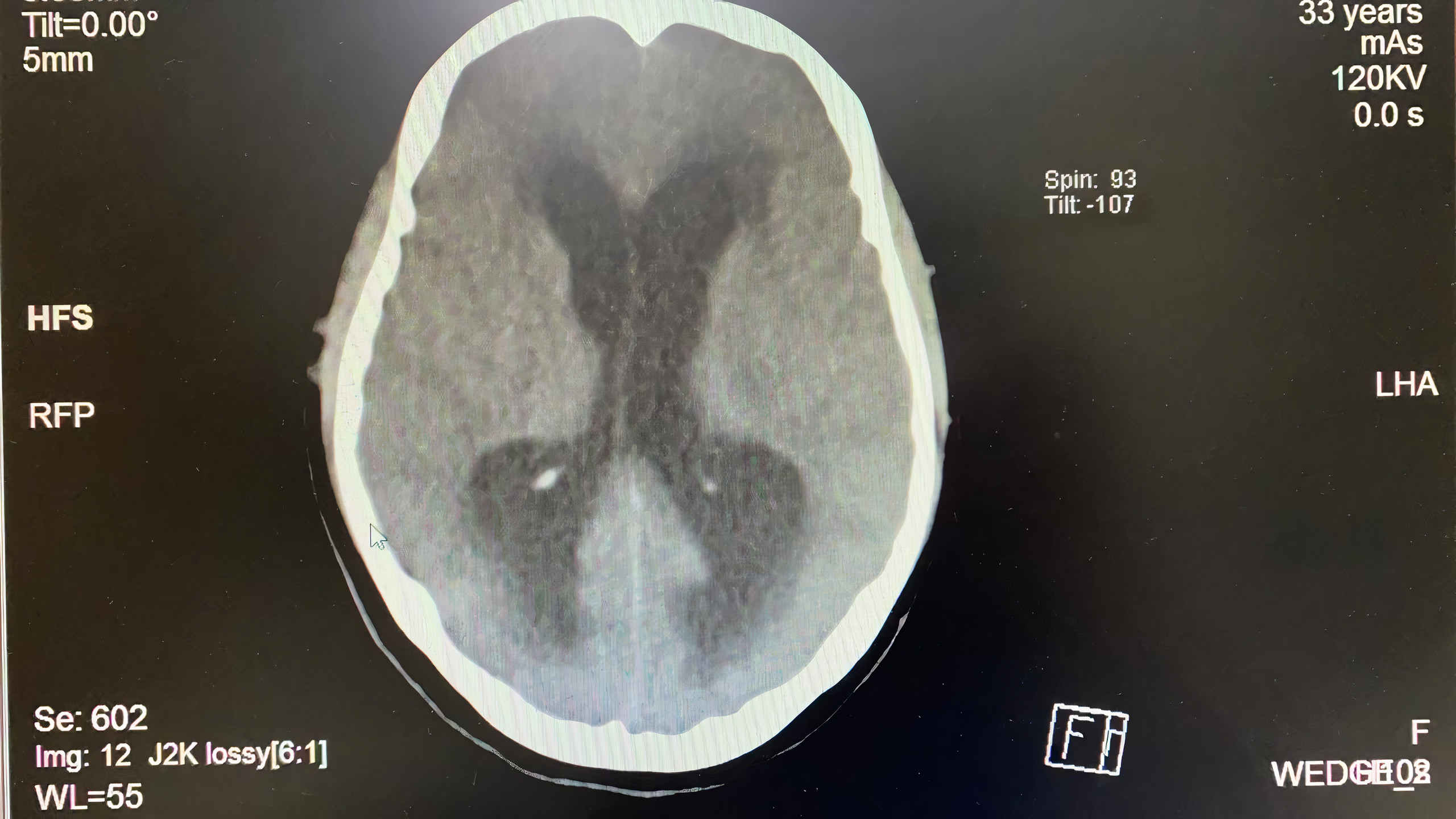
During MRI examination, the patient became increasingly agitated and we could not continue the examination. The radiology registrar gave the patient an infusion of dormicum in a trial for sedation, but it was not effective. Anaesthesiology registrar was called. He obtained consent from the patient husband and gave her sevoflurane by inhalation. The patient became adequately sedated, and we continued the MRI examination under monitoring. The patient then suddenly developed shooting Hypertension (HTN) (BP was 170/110) then profound hypotension (BP was 50/20) that was followed by respiratory collapse. MRI examination was called off. The patient was urgently intubated and mechanically ventilated. She was transferred to Neurology Intensive Care Unit (NICU), where she was put on parenteral epinephrine and norepinephrine infusions for Cardiovascular (CV) support with foetal surveillance by Cardiotocogram (CTG). The radiology and neurology registrars assessed the few hazy MRI cut images that could be saved before the patient collapsed. They found the images were suggestive of supratentorial obstructive hydrocephalous. Accordingly, we made an urgent neurosurgical consultation. A neurosurgery consultant assessed the patient and decided that it was late for any decompression intervention. The patient lost most reflexes, she had a GCS of 5, and her pupils became unreactive. Computed Tomography (CT) scan of the brain was done while she was administered parenteral frusemide and mannitol in an attempt to lower Intracranial Pressure (ICP). CT showed diffuse brain oedema on transverse view (Figure 1) and Brain Stem (BS) herniation on sagittal view (Figure 2). The condition was getting worse, with CV support medications infusion rate increased to maximum, and CTG became non-reassuring. The patient husband was counselled about rescue CS but he declined it. The patient progressively lost all reflexes; her GCS was 3, with bilateral dilated fixed pupils. Blood pressure continuously declined and CTG showed long bradycardia. Both the patient and her fetus died. Of note, the patient did not have seizures or focal neurological deficits at any time during her hospital course.

Box 1:
• Headache with encephalopathy, fits, focal signs, or papilledema. |
• Headache unresponsive to analgesics. (our case) |
• Sudden severe headache. |
• Headache with history of head trauma. |
• Headache during an exertion, example: during sexual activity, cough, Valsalva manoeuvre. |
• Headache with fever, with or without neck stiffness. |
• Headache with history of exposure to toxic substance, unknown drug, and anaesthesia. |
• Positional headache; that increases with lying down or just after waking up. |
• New onset migraine headache, or change in pattern of a previous known tension or cluster type headache. |
• Headache with history of venous thrombosis, CVT, or any thrombophilic factor. |
Differential diagnoses
Preeclampsia is responsible for >30% of cases presenting with new onset headache after 20 weeks of gestation, which is why preeclampsia was a major diagnosis to exclude first. However, the patient had no albumin in urine by testing with urine strips twice. Her BP was measured manually twice and it read within 110/70 range each time. Finally, the patient had no history of HTN in this pregnancy or in the previous one.
Intracranial Haemorrhage (ICH) was one of the differentials giving the progressive persistent headache that is associated with symptoms of increased ICP (vomiting and blurry vision). That’s why CT brain was ordered after the incomplete MRI examination. CT failed to detect any ICH, but it detected BS herniation and diffuse brain oedema. This was logical as the patient had not had any risk factor for ICH like: trauma, old age, HTN or anticoagulation therapy [3]. Furthermore, she had not had any neurological deficits or seizures occurred at any time during her hospital course.
Idiopathic increase ICP (Pseudotumor Cerebri (PTC)), although rare, was one of differentials given that our patient was a childbearing obese female, who is a common PTC type of patients [4]. Even though our patient showed signs of high ICP, but the short duration of headache as well as the acute onset, rapid progression, and failure to respond to diuretics excluded this diagnosis.
Amniotic fluid embolism was one of differentials that was excluded as well, as it commonly develops peripartum or after an obstetric accident like ROM or antepartum haemorrhage [5]. In addition, the patient lab results did not suggest any Disseminated Intravascular Coagulopathy (DIC) and her main symptom was headache.
Finally, a diagnosis of exclusion of CVT was made after reviewing the literature, imaging findings as well as the patient presentation and clinical progression.
Discussion
Headache is a very common complaint during pregnancy. There are certain symptoms and signs associated with headache that suggests an underlying serious disorder and requires prompt evaluation (Table 1). Preeclampsia is responsible for one third of these after 20 weeks of gestation. If excluded, approximately half the other cases would have migraine headache and the other half would have a variety of other causes, like: CVT, infection, mass lesion, stroke, ICH, medication withdrawal, and post-dural puncture headache [1].
CVT is a very uncommon but serious disease which commonly affects women of childbearing age. It has an incidence of 1.5 per 100,000/year. The major risk factors for CVT are all known pro-thrombotic conditions like oral contraceptives, pregnancy, peri-partum state, malignancy, infection, head injury, and mechanical precipitants [2]. This patient’s only known pro-thrombotic factor were pregnancy, mild obesity and may be prolonged recumbence. Due to the seriousness and rapid progression of her condition, we could not get detailed family or contraceptive history. The clinical presentation of CVT is highly variable, especially that it more commonly develops during post-partum period than during pregnancy period. However, headache (of gradual, acute, subacute, or thunderclap onset) is the most frequent symptom. It occurs in almost 90% of cases with or without vomiting, papilledema, and visual symptoms like blurry vision. In some cases, it can be accompanied by focal neurologic deficits, seizures, and encephalopathy with altered mental status or coma. Parenchymal brain lesions, including brain swelling, oedema, venous infarction, and haemorrhagic venous infarction may occur secondary to venous occlusion [2].
Our patient reported headache that started acutely from 28 hours, was progressing, and not responding to analgesics. She also vomited twice and had blurry vision. This triad of symptoms should raise suspicion of increased ICP. We were more concerned with preeclampsia as it is clinically and theoretically more common, with the fact that blurry vision and vomiting can also be symptoms of preeclampsia. That’s why we measured BP manually and tested albuminuria twice.
MRI brain with MRV is the imaging of choice for diagnosis of CVT. The presence of abnormal signs in a venous sinus in T2 weighted image in MRI as well as the absence of venous flow in MRV confirm the diagnosis. In some cases, absence of venous flow in MRV is the only finding and is sufficient for diagnosis. CT venography is the alternative if MRV is not available, but plain CT is nonspecific, normal in 30% of patient patients, and it shows direct signs in 30% only of patients. These are: empty delta sign, cord sign, and dense triangle sign [2].
Our patient could not complete the MRI or even start the MRV exam as she severely deteriorated after administration of sevoflurane inhalation anaesthesia for sedation. It turned out iatrogenic as, after reviewing literature, sevoflurane is a potent volatile drug that decreases cerebral metabolism through affecting cerebral blood flow and thus increasing ICP [6]. This may explain the sudden severe deterioration that happened after its administration that could not be reversed, as BS herniated from iatrogenically augmented high ICP. Most inhalation anaesthetics, except nitrous oxide (N2 O), are potent volatile agents that should never be used in an agitated or drowsy patient, especially if suspecting high ICP.
For pregnant women with CVT, immediate full dose of therapeutic anticoagulation with Low Molecular Weight Heparin (LMWH) should be administered immediately. This should be followed by measures to lower ICP, such as diuretics, and interventions like decompression craniotomy and spinal tapping. Seizure prophylaxis was not indicated here. Prophylaxis is only indicated in patients having seizures more than once with positive MRI or CT scan findings of cerebral supratentorial focal lesion like oedema, haemorrhage or infarction [7]. Considering our patient’s rapid state of progressive deterioration, perhaps, starting full dose LMWH earlier would have decreased the rate of progression and prolonged the time for further investigations that may have ended in a better outcome. Furthermore, intervening through taping or craniotomy after BS herniation was futile and would have just added an extra burden on the patient and her family, as brain stem herniation is irreversible.
CVT is associated with good outcome in more than 80% of cases with complete resolution or minor residual signs. 10% has long term morbidity and mortality, and 5% die in the acute phase as our patient [7]. In this patient, we think that multiple interventions could have led to better outcome, like: 1- Early suspicion of increased ICP from its triad of symptoms: Headache, vomiting and blurry vision. 2- Bedside fundus examination through an ophthalmoscope could have detected papilledema and diagnosed an increased ICP instead of waiting for long MRI scan. However, an ophthalmoscope was unavailable in our triage. 3- Early immediate full dose therapeutic anticoagulation with LMWH could have been beneficial. The EM registrar was very keen on excluding ICH through brain imaging however before we can give heparin. 4- Early spinal tapping could have diagnosed and lowered the very high ICP. Possibly, early diuretics could have been of help as well. 5- Not administering sevoflurane; this was an absolute iatrogenic error. 6- Knowledge of headache characteristics that indicate serious underlying aetiology (Table 1) necessitating urgent management.
Our case represents a model for an unusual presentation and progression of a rare disease, as well as opportunity to learn from our medical errors. It highlights that certain headache characteristics mentioned earlier in Table 1, such as new onset headache unresponsive to analgesics in this case, suggest a serious underlying disorder and should be immediately and carefully investigated.
Learning points/conclusion
• CVT is a rare disease that can be triggered by pro-thrombotic factors like pregnancy.
• Headache is the most frequent symptom of CVT, with or without signs of increased ICP like vomiting and papilledema.
• Acute onset of progressive persistent headache that is unresponsive to analgesics is a sign of CVT and is one of the criteria of secondary headache (Table 1) that may be associated with a serious underlying disorder and needs an immediate assessment.
• Potent inhalation anaesthesia including Sevofluorane are known to raise the ICP. Hence, it should not be administered to any patient suspected to have increased ICP as this can be fatal.
• MRV is the gold standard for diagnosis of CVT, and its management includes emergency anti-coagulation followed by decompression measures, with or without seizure prophylaxis.
Conflict of interest: The authors declare they do not have any conflict of interest
References
- Lee M, Guinn D, Hickenbottom S. Headache in pregnant and postpartum women. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. 2020.
- Ferro JM, Canhao P. Cerebral venous thrombosis: Etiology, clinical features, and diagnosis. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. 2020.
- Rodorf G, Mcdonald C. Spontaneous intracerebral hemorrhage: Pathogenesis, clinical features, and diagnosis. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. 2020.
- Lee AG, Wall M. Idiopathic intracranial hypertension (pseudotumor cerebri): Epidemiology and pathogenesis. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. 2020.
- Baldisseri MR, Clark SL. Amniotic fluid embolism. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. 2020.
- Hays SR. Inhalation anesthetic agents: clinical effects and uses. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. 2020.
- Ferro JM, Canhao P. Cerebral venous thrombosis: treatment and prognosis. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. 2020.