
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Hypertriglyceridemia induced pancreatitis: An increasing cause of acute pancreatitis: A district hospital experience
Hnin Sanda1; Bashir Mahamud1,2*; Shrini Patel1; Noha Meneissy1; Hassan Rehmani1; Suhier Elshowaya1; Gideon Mlawa1,2
1 Queens Hospital, Romford-London.
2 Trakia University, Stara Zagora- Bulgaraia.
*Corresponding Author: Bashir Mahamud
Queens Hospital, Romford-London.
Email: mahamudbashir7@gmail.com
Received : Jul 16, 2021
Accepted : Sep 30, 2021
Published : Oct 07, 2021
Archived : www.jcimcr.org
Copyright : © Mahamud B (2021).
Abstract
Hypertriglyceridemia is becoming an increasing causative factor of acute pancreatitis. HTG is characterised by the presence of serum triglyceride greater than 1.7 mmol/l (>150 mg/dL). HTG induced acute pancreatitis is associated with high morbidity and mortality and if not treated timely
Citation: Sanda H, Mahamud B, Patel S, Meneissy N, Rehmani H, et al. Hypertriglyceridemia induced pancreatitis: An increasing cause of acute pancreatitis: A district hospital experience. J Clin Images Med Case Rep. 2021; 2(5): 1347.
Introduction
Acute pancreatitis is an inflammatory disease of the pancreas and a common medical emergency that requires immediate hospital admission. The inflammation caused by acute pancreatitis can lead to necrosis of pancreas or may progress to multisystem organ failure. It is important to determine the cause of the pancreatitis to deliver prompt management. The main causes of acute pancreatitis are excessive alcohol consumption and gallstones [1-4].
Hypertriglyceridemia (HTG) is an established etiological cause of acute pancreatitis, which is increasing in incidence. HTG induced acute pancreatitis is associated with significant morbidity and mortality. HTG is classified based on serum Triglyceride (TG) levels. Mild HTG - >1.7 mmol/l- 2 mmol/l (normal, <1.7 mmol/l or 150 mg/dL), moderate- >2 .3 -11.2 mmol/l, severe – >11.2- 22.4 mmol/l. Severely elevated has strong correlation with causing acute pancreatitis [5,1,6,7].
Often HTG provoked pancreatitis occurs in patients with uncontrolled chronic metabolic conditions such as diabetes and hypothyroidism; and pre-existing lipid abnormality such as type I dyslipidemia (Friedrickson’s classification) [3,8,9,10].
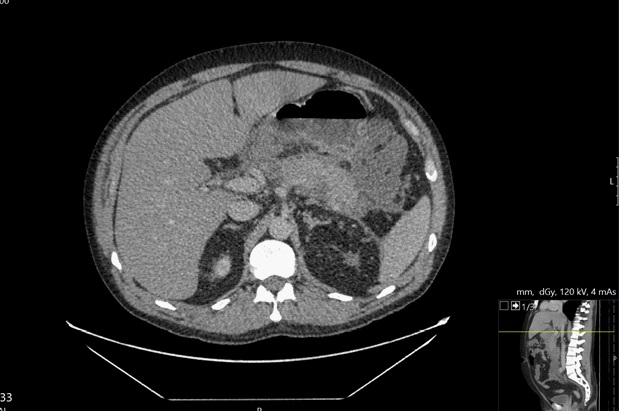
Case 1
At time presentation the patient presented with signs of acute pancreatitis characterised by fever, worsening abdominal pain of epigastric nature. Bloods on admission showed raised C-reactive protein (CRP) (399 mmol/l) and lipid profile showed low HDL (0.71 mmol/l) and high Cholesterol (5.8 mmol/l) and TG (14.34 mmol/l). Physical examination determined abdominal tenderness and guarding. Radiological examination using Computed Tomography (CT) performed on admission showed signs of acute pancreatitis depicted in the image below (Figure 1). The patient was kept at the district general hospital for observation for 6 days and following improvement in the patient’s condition was discharged with recommendations for lifestyle changes and atorvastatin as a preventative measure.

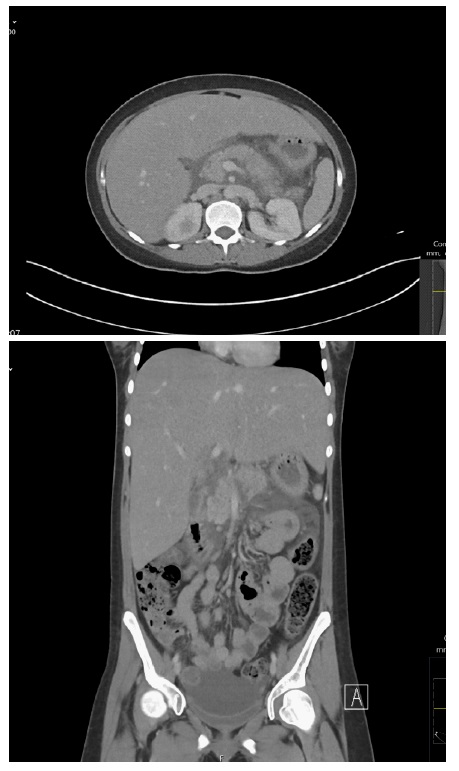
Case 2
A 38-year-old man with previous history of depression, alcohol dependence and fatty liver attended ED with a 2 day complaint of epigastric pain and vomiting. During the initial assessment the patient indicated he was unable to eat and drink and had episodes of haematemesis. On physical examination, the patient had distended abdomen and tenderness in the epigastric region and a Glasgow Coma Scale Score (GCS) of 4. Once the patient was stabilised a CT scan was performed which indicated acute pancreatitis (Figure 2). In ED the patient was treated for alcohol withdrawal and admitted to a High Dependency Unit (HDU) for monitoring and treatment.
Blood test on admission showed high TG (77.89 mmol/l), CRP (212 mmol/l) and Lactate Dehydrogenase (LDH) (619 mmol/l). As a consequence of elevated inflammatory markers a CTAP was performed, this showed increased fluid collection and small necrosis in the tail of the pancreas.
The patient was started on fenofibrate for HTG and US-guided drainage of the intra-abdominal fluid collections was done. This treatment alleviated the patients’ pain and was discharged with follow up with the gastroenterology team.
Case 3
A 17-year-old girl with type 1 diabetes mellitus was admitted with two-day history of epigastric pain, persistent vomiting and unable to eat and drink. On examination, she had tenderness and guarding in the abdomen. Blood test on admission showed high amylase (1184 mmol/l) TG (19.65 mmol/l) which raised clinical suspicion of HTG induced acute pancreatitis. CT confirmed the diagnosis of acute pancreatitis (Figure 3). The patient was admitted and treated conservatively. She was started on fenofibrate for HTG.
Discussion
HTG is a common form of dyslipidaemia, which result from a combination of genetic variations and environmental factors. HTG has a strong correlation with underlying conditions such as obesity, uncontrolled diabetes and excessive alcohol consumption. Also, elevated triglyceride levels are a major risk factor for several cardiovascular diseases such as atherosclerosis and hypertension. The exact mechanism of how HTG causes acute pancreatitis is not clear but it is believed to involve lipotoxicity due to disorder of lipoprotein metabolism which results in excessive levels of fatty acids that ultimately damages pancreatic tissue and results in prolonged inflammation. When triglycerides are > 10 mmol/l chylomicrons are present in the circulation and they are large enough to occlude the pancreatic capillaries, leading to ischemia and necrosis. As a result of necrosis, the pancreas can become infected and which can be spread haematogenous causing multi-organ failure. The main affected organs are the lungs, kidneys and cardiovascular system [8,11,12].
Diagnosis of acute pancreatitis is based on presence of at least 2 of the following factors clinical factors including abdominal pain, elevated pancreatic enzymes and radiologic features of acute pancreatitis [13]. It is important to determine lipid profile as part of the diagnostic workup to determine HTG as causative factor in patients presenting with signs and symptoms of acute pancreatitis, predominantly, serum triglycerides and cholesterol [14]. As part of initial workup a thorough family history of lipid abnormalities should also be obtained [15]. Mild to moderate elevations in triglycerides (2-10 mmol/L) is seen in early stages of acute pancreatitis of any cause [11].
To prevent hypertriglyceridemia induced pancreatitis, it is important to achieve a fasting serum TG <4.5mmol/L, this can be achieved through pharmacological interventions and lifestyle modifications. In patients with mild to moderate HTG the main mode of therapy involves lifestyle modification through a balanced diet and increased physical activity in the form of exercise.
Patient with severe HTG management involves lifestyle modification in combination with drug treatment to reduce the risk of pancreatitis associated complications. In most National health service hospitals (NHS) trust in the United Kingdom the first-line drug therapy for HTG are fibrates (Fenofibrate) and second-line therapy using Statins (atorvastatin) is added in situations where TG remains >4.5 mmol/L after Fibrates therapy. Through this management protocol risk of concomitant cardiovascular disease and distant organ failure due to HTG is also prevented.
Conclusion
The case series presented here has highlighted the increase in the incidence of acute pancreatitis due to HTG. An increase in sedentary lifestyle worldwide will only increase the frequency with which HTG linked acute pancreatitis is encountered in the emergency department. Therefore it is important to carry out lipid profile analysis as part of the initial workup, currently, this is not a widely practised protocol. This would enable HTG mediated therapy to be initiated earlier, thereby limiting both the progression of pancreatitis and prevent complications such as multi-organ failure.
References
- Zerem E. Treatment of severe acute pancreatitis and its complications. World Journal of Gastroenterology. 2014; 20: 13879.
- Gapp J, Chandra S. Acute Pancreatitis. [online] PubMed. 2020.
- Yang A, McNabb-Baltarb J. Hypertriglyceridemia and acute pancreatitis. Pancreatology. 2020; 20: 795–800.
- Gimenez T, Calvo A, Vicent J. Etiology of acute pancreatitis. Open Medicine. 2014; 9.
- de Pretis N, Amodio A, Frulloni L. Hypertriglyceridemic pancreatitis: Epidemiology, pathophysiology and clinical management. United European Gastroenterology Journal. 2018; 6: 649–655.
- Munoz MA, Sathyakumar K, Babu BA. Acute pancreatitis secondary to hypertriglyceridemia. Cleveland Clinic Journal of Medicine. 2020; 87: 742–750.
- Wan J, He W, Zhu Y, Zhu Y, Zeng H, et al. Stratified analysis and clinical significance of elevated serum triglyceride levels in early acute pancreatitis: a retrospective study. Lipids in Health and Disease. 2017; 16.
- Kota S, Kota S, Krishna SVS, Modi K, Jammula S. Hypertriglyceridemia-induced recurrent acute pancreatitis: A case-based review. Indian Journal of Endocrinology and Metabolism. 2012; 16: 141.
- Scherer J, Singh VP, Pitchumoni CS, Yadav D. Issues in Hypertriglyceridemic Pancreatitis. Journal of Clinical Gastroenterology. 2014; 48: 195–203.
- Mitchell-Brown F. Hypertriglyceridemia-induced acute pancreatitis. Nursing Critical Care. 2020; 15: 18–23.
- Gan SI. Hypertriglyceridemia-induced pancreatitis: A case-based review. World Journal of Gastroenterology. 2006; 12: 7197.
- Kiss L, Fűr G, Mátrai P, Hegyi P, Ivány E, et al. The effect of serum triglyceride concentration on the outcome of acute pancreatitis: systematic review and meta-analysis. Scientific Reports. 2018; 8: 14096.
- Berglund L, Brunzell JD, Goldberg AC, Goldberg IJ, Sacks F., et al. Evaluation and Treatment of Hypertriglyceridemia: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism. 2012; 97: 2969–2989.
- Garg R, Rustagi T. Management of Hypertriglyceridemia Induced Acute Pancreatitis. [online] BioMed Research International. 2018.
- Bae JH, Baek SH, Choi HS, Cho KR, Lee HL, et al. Acute pancreatitis due to hypertriglyceridemia: report of 2 cases. The Korean journal of gastroenterology = Taehan Sohwagi Hakhoe chi. 2014; 46.