
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Mediastinal thoracic duct cyst: A rare entity
Shah Omair1*; Gojwari Tariq2; Shah Aamir3; Jan Suhail1
1 Senior Resident, Department of Radiology, Skims Soura, J&K, India.
2 Professor, Department of Radiology, Skims Soura, J&K, India.
3 Department of Radiology, Skims Soura, J&K, India.
*Corresponding Author: Omair Shah
Senior Resident, Department of Radiology, Skims Soura,
J&K, India.
Email: shahomair133@gmail.com
Received : Aug 30, 2021
Accepted : Oct 01, 2021
Published : Oct 08, 2021
Archived : www.jcimcr.org
Copyright : © Omair S (2021).
Abstract
Thoracic Duct Cysts (TDCs) are exceedingly rare benign masses of the posterior mediastinum. They are thought to arise from congenital or degenerative weakening in the thoracic duct wall. We bring to light an incidentally detected posterior mediastinal cystic lesion that caused dysphagia in our patient and was found to be a thoracic duct cyst.
Citation: Omair S, Tariq G, Aamir S, Suhail J. Mediastinal thoracic duct cyst: A rare entity. J Clin Images Med Case Rep. 2021; 2(5): 1351.
Case presentation
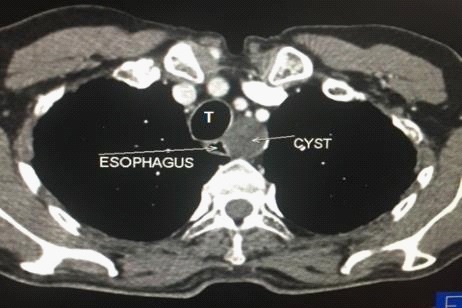
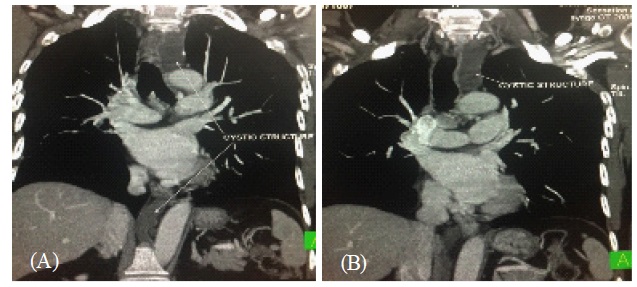
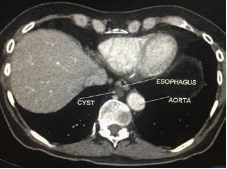
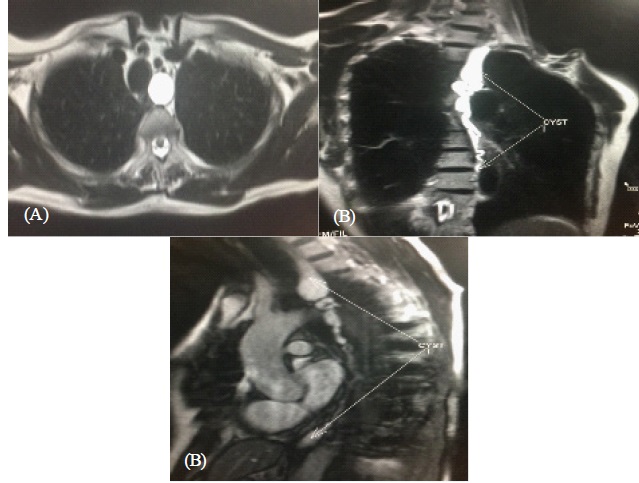
During evaluation of 45 yr old male for dysphagia with barium swallow showing smooth posterior indentation of the esophagus, possibilities of duplication cyst and leiomyoma were made. Clinical examination and routine blood baseline investigations were normal. PA Chest radiograph was reported as normal with no mediastinal mass evident. UGI endoscopy showed smooth posterior narrowing of mid thoracic esophagus, no obvious mass or stricture was seen. A contrast enhanced CT chest & abdomen was done in our department on CT SOMATOM SENSATION 64, which revealed a well defined water density lesion in the posterior mediastinum in posterior relation to esophagus (Figure 1). Diagnostic possibilities of bronchogenic cyst, esophageal duplication cyst and neurogenic cyst were made. However on evaluation of 3D multiplanar images continuation of the cystic structure both caudally and cranially in the form of narrow tubular non opacified structure terminating at the junction of SCV and IJV was noted giving credence to the rare diagnosis of thoracic duct cyst (Figure 2). The cyst was seen indenting the posterior wall of the esophagus (Figure 3). Bilateral lung fields, trachea and main stem bronchi were unremarkable. There was no evidence of significant mediastinal lymphadenopathy. No cervical nodes or bone lesions were seen. Mediastinal vasculature was normal. No pleural effusion was seen ruling out rupture. MRI of the patient was advised to assess the character of the cyst and we found a T2 hyperintense cystic lesion in the posterior mediastinum in close relation to esophagus which connected to a T2 hyperintense elongated structure extending from the abdomen to the neck region in keeping with thoracic duct cyst (Figure 4).
Disscusion
The first reported case was found during an autopsy examination by Carbone in 1892 and the first ante mortem description of this disease was made by Emerson in 1950 [1]. Cysts of the thoracic duct can occur either above or below the diaphragm. Supradiaphragmatic thoracic duct cysts are typically found in the neck. Mediastinal thoracic duct cysts are quite uncommon [2-4]. The cysts are symptomatic because of the pressure on adjacent structures. Symptoms such as coughing, dyspnea, and chest discomfort may be experienced. Symptoms of dysphagia are often associated with ingestion of fatty foods. Furthermore, acute respiratory insufficiency after ingestion of a fatty meal can be seen in some patients [4-6]. Thoracic duct cysts are totally benign and carry an excellent prognosis after adequate surgical excision. No cases of malignant transformation have been reported so far [7]. Conservative management is generally advocated for lymphocoeles of the thoracic duct [8]. In summary, our patient was incidentally diagnosed with a mediastinal cystic tumor during evaluation for dysphagia. Initially, the possibility of a thoracic duct cyst was not considered, due to unfamiliarity and very rare (In fact the first case of its kind in our state) occurrence. These benign lesions are diagnostically challenging with distinct clinical significance, since they can be easily mistaken for other, more common mediastinal tumors.
Informed consent: Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Emerson GL. Supradiaphragmatic thoracic duct cyst: an unusual mediastinal tumor. New Engl J Med. 1950; 242: 575-8.
- Mattila PS, Tarkkanen J, Mattila S. Thoracic duct cyst: A case report and review of 29 cases. Ann Otol Rhinol Laryngol. 1999; 108: 505–50.
- Okabe K, Miura K, Konishi H, et al. Thoracic duct cyst of the mediastinum. Scand J Thorac Cardiovasc Surg. 1993; 27: 175–177.
- Karajiannis A, Kruegetb T, Stauffer E, et al. Large thoracic duct cyst. Eur J Cardiothorac Surg. 2000; 17: 754–756.
- Morettin LB, Allen TE. Thoracic duct cyst: Diagnosis with needle aspiration. Radiology. 1986; 161: 437–438.
- Gottwald F, Iro H, Zenk J, et al. Thoracic duct cysts: A rare differential diagnosis. Otolaryngol Head Neck Surg. 2005; 132: 330–333.
- Kumar A, Ramakrishnan TS, Sahu S. Primary cervical thoracic duct cyst: a case report and review of the literature. Ear Nose Throat J. 2014; 93: E17-21.
- Offiah CE, Twigg S. Lymphocoele of the thoracic duct: A cause of left supraclavicular fossa. The British journal of radiology. 84: e27-30.