
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Impact of acne variables on Egyptian patients’ psychometric and quality of life
Azza M Abdel-Meguid1; Emad A Taha1; Ahmed A Abdelrahman2; Fatma M Soltan3; Doaa AE Abou-Taleb1*
1 Department of Dermatology, Venereology and Andrology, Faculty of Medicine, Assiut University, Assiut, Egypt.
2 Department of Neuropsychiatry, Faculty of Medicine, Assiut University, Assiut, Egypt.
3 Mental Health Hospital, Assiut, Egypt.
*Corresponding Author: Doaa AE Abou-Taleb
Department of Dermatology, Venereology, and Andrology, Assiut University, Assiut, Arab Republic of Egypt.
Email: doaa_aboutaleb@aun.edu.eg & dodda_aboutaleb@yahoo.com
Received : Aug 30, 2021
Accepted : Oct 04, 2021
Published : Oct 11, 2021
Archived : www.jcimcr.org
Copyright : © Abou-Taleb DAE (2021).
Abstract
Background: Acne vulgaris is a common skin disease which has a major impact on quality of life and common psychiatric co-morbidities.
Objective: was to assess Quality Of Life (QOL) and depression in Egyptian acne patients and the effect of acne variables such as clinical severity, disease duration, type of treatment and presence of complications on patients’ psychometric using objective scales.
Patients and methods: Four hundred acne patients and one hundred healthy participants as controls were included in the study. The patients were subjected to clinical examination with assessment of acne severity by Global Acne Grading Scale (GAGS) and patient selffulfillment of 2 psychometric questionnaires: Cardiff Acne Disability Index (CADI) and Beck depression inventory (BDI).
Results: There was significant impairment of QOL in Egyptian acne patients. Impairment of QOL was significantly correlated with acne severity and its complications. Moreover, increase in depression scores was also found to be significantly correlated with acne severity and its complications.
Conclusion: There is strong positive correlation between the severity and complications of acne and the psychiatric condition of the patients. Psychiatric assessment and early management of the acne patients is necessary.
Keywords: acne; quality of life; depression; questionnaire.
Citation: Abdel-Meguid AM, Taha EA, Abdelrahman AA, Soltan FM, Abou-Taleb DAE. Impact of acne variables on Egyptian patients’ psychometric and quality of life. J Clin Images Med Case Rep. 2021; 2(5): 1354.
Introduction
Acne vulgaris is a common chronic inflammatory skin disease of the pilosebaceous unit with a multifactorial etiology. It is one of the most frequent cutaneous diseases, affecting more than 80% of individuals at some stage of their life [1].
Although acne is not life threatening or physically debilitating disease, it can lead to significant psychological stress and can affect all aspects of an individual’s health-related Quality Of Life (QOL) [2].
Previous studies reported significant impairment of QOL in acne patients among different populations. The results seemed to be affected by acne variables like disease severity in addition to patient variables as age and sex [3-6].
Global Acne Grading Scale (GAGS) is a simple, accurate, fast method for assessment of acne severity. Its personal and interpersonal differences are low [7].
Many of the published studies which assessed QOL in acne patients used the Dermatology Life Quality Index (DLQI) questionnaire [3]. The (DLQI) is a questionnaire that evaluates QOL in patients with different dermatological diseases, while Cardiff Acne Disability Index (CADI) is a disease specific questionnaire for acne. CADI is a well validated acne psychometric test that can be easy self-fulfilled by the patient quickly [5,8].
Most of studies about depression in acne patients used to evaluate it as a part of general psychological assessment that evaluated also other psychological problems such as phobia, anxiety, somatization, hostility and psychoticism [3,9]. Some other studies discussed the depression related to isotretinoin therapy in acne [10]. Beck Depression Inventory (BDI) is one of the most famous, reliable and valid questionnaires in diagnosis and scoring of depression [11,12].
In the current study, we aimed to assess QOL and depression in Egyptian acne patients using 2 psychometric scales (CADI and BDI). In addition, to assess the effect of acne variables such as clinical severity, disease duration, type of treatment and presence of complications on these psychometric scales.
Patients and methods
This prospective cross-sectional study was carried out on 400 acne patients with variable degree of severity and 100 healthy participants as controls. They were randomly recruited from the outpatient clinics of dermatology department of Assiut Universty Hospital. Exclusion criteria included patients with trunkal acne only and those with any associated chronic dermatological disease such as vitiligo, psoiasis and pemphigus. Those with primary psychic disorders, pregnant and lactating women were also excluded.
The study design was approved by the Institutional Ethics and Research Committee of the Faculty of Medicine, Assiut University and was carried out in accordance with the guidelines of the Helsinki Declaration. From all patients informed consent was obtained prior to the study.
Patients were subjected to full history taking and dermatologic examination was done to assess the acne type, severity by the (GAGS) [7] and presence of any complications such as acne scars and pigmentations.
Fulfillment of the Arabic version of (CADI) [8]:
CADI is acne-specific five-item questionnaire. Each question has four possible answers. The CADI score is calculated as the sum of score of five questions. The CADI score is calculated by summing the score of each question resulting in a possible maximum score of 15 and a minimum score of 0. A score of 0~5 translates to mild QOL impairment, 6~10 indicates moderate impairment, and 11~15 demonstrates severe impairment.
Fulfillment of the Arabic version of (BDI) [12]:
The BDI scale includes a 13 items using a four-points scale ranging which ranges from 0 (symptom not present) to 3 (symptom very intense). The BDI score is calculated as the sum of score of 13 questions. In males, if the age is 17 years or less a score of 0-6 translates to non or minimal depression, 7-13 indicates mild depression, 14-23 demonstrates moderate depression, and +24 indicates severe depression. In males aged more than 17 till 24 years a score of 0-7 indicates none or minimal depression, a score of 8-11 indicates mild depression, a score of 12-20 indicates moderate depression, and a score of 21 or more indicates severe depression. In males above the age of 24 years, a score of 0-6 indicates none or minimal depression, a score of 7-12 indicates mild depression, a score of 13-18 indicates moderate depression, and a score of 19 or more indicates severe depression.
In females, if the age is 17 years or less a score of 0-9 translates to non or minimal depression, 10-16 indicates mild depression, 17-23 demonstrates moderate depression, and +24 indicates severe depression. In females aged more than 17 till 22 years a score of 0-8 indicates non or minimal depression, a score of 9-14 indicates mild depression, a score of 15-23 indicates moderate depression, and a score of 24 or more indicates severe depression. In females above the age of 22 years, a score of 0-8 indicates non or minimal depression, a score of 9-14 indicates mild depression, a score of 15-20 indicates moderate depression, and a score of 21 or more indicates severe depression.
Statistical analysis
The data were analyzed using the Statistical Package of Social Science (SPSS version 19; SPSS Inc., Chicago, IL) software program. Data analysis started by descriptive statistics (frequencies, percentages, mean and standard deviation). Then application of tests of significance was done for group comparison as Chi- square (x) 2 in comparing qualitative variables and mann-whitny test to compare quantitative variables in different groups. Finally, correlation was done using Spearman correlation test between quantitative variables. P-value ≤ 0.05 was considered significant.
Results
Demographic data of the study
The study included 400 acne patients, 95 were males and 305 were females with mean age ± SD was (18.13 ± 3.5 years) and 100 controls, 22 were males and 78 were females with mean age18.66 ± 4.3 years). There was no significant difference in socio-demographic data between patients and controls as regards age, sex, occupation, residence and marital status.
Regarding acne patients group, the majority had progressive disease course (55.8%), followed by intermittent course (26.5%) then stationary course (12.5%), while (5.5%) had regressive course. The mean acne duration was 5.4 ± 1.5 years. About acne severity, the mean of GAGS in patients was 19.51 ± 8.1 with 51% of cases had mild acne severity, 35% had moderate acne and 14% had severe acne. Concerning complications, about (46%) had acne scars mostly atrophic, about 33% had post-inflammatory hyperpigmentation and about 2% had both. Regarding treatment, 197 (49.2%) were receiving acne treatment among them, 195 (99 %) were receiving topical and 91 (46.2%) were receiving systemic treatment (antibiotics or retinoids or both). 44 (22.3%) were receiving other treatment modalities (laser, chemical peel or microdermabrasion).
CADI and impact of different variables on its score
The mean of CADI was 7.69 ± 3.1. Acne severity and disease course had significant negative impact on QOL while acne duration had not. Those with severe GAGS had significantly higher CADI score as shown in (Table 1).
Table 1: Effect of disease variables on (CADI) in the study group. (n=400).
Item |
Mild CADI score |
Moderate/Severe CADI score |
P-value |
|
GAGS score |
Mean ± SD |
16.02 ± 7.5 |
20.60 ± 8.0 |
< 0.001* |
Severity (grades) |
|
59 (29.1%) |
144 (70.9%) |
|
|
|
36 (25.7%) |
104 (74.3%) |
< 0.001** |
|
|
0 (0%) |
57 (100%) |
|
Course |
|
53 (23.8%) |
170 (76.2%) |
|
|
|
15 (14.2%) |
91 (85.8%) |
|
|
|
18 (36.7%) |
31 (63.3%) |
0.007** |
|
|
9 (40.9%) |
13 (59.1%) |
|
Duration/years |
Mean ± SD |
1.63 ± 0.2 |
1.63 ± 0.1 |
0.988* |
*T-test was used to compare the mean difference between groups **Chi-square test was used to compare the difference in proportions between groups
The final logistic regression model for CADI predictors showed that adjusted odds ratio is significantly higher among patients with severe GAGS (AOR=31.21), thus acne severity was the first significant predictor for poor QOL. The second predictor was the female sex (AOR=5.62) and the third was the presence of mixed post-acne complications (AOR=5.01) (Table 2).
Table 2: Final Logistic Regression Model for CADI Disability Predictors.
Predictor |
AOR** |
95% CI** |
LRT+ P-value |
Course |
|
|
|
|
1 (Reference) |
|
0.017 |
|
1.54 |
0.69 – 3.15 |
0.094 |
|
0.79 |
0.29 – 0.92 |
0.031 |
|
0.61 |
0.09 – 5.55 |
0.899 |
GAGS Score |
1.92 |
1.07 – 3.06 |
< 0.001 |
Severity (Mild) |
1 (Reference) |
|
0.012 |
Severity (Moderate) |
1.01 |
0.06 – 4.65 |
0.896 |
Severity (Severe) |
31.21 |
4.81 – 68.21 |
0.003 |
Post-acne complications |
|
|
|
|
1 (Reference) |
|
0.048 |
|
0.78 |
0.04 – 14.92 |
0.868 |
|
1.09 |
0.46 – 2.63 |
0.841 |
|
5.01 |
1.60 – 15.73 |
0.006 |
**AOR=Adjusted Odds Ratio, CI= Confidence Interval +LRT=Likelihood Ratio Test
BDI and impact of different variables on its score
Egyptian acne patients had significantly higher mean BDI value than controls. Patients also had higher frequencies of severe and moderate depression grades (Table 3).
Table 3: Comparison between cases and controls regarding BDI score.
|
Cases |
Controls |
P-value |
|
BDI |
Mean ± SD |
12.56 ± 6.9 |
6.92 ± 4.2 |
< 0.001* |
Median & Range |
11 (0-32) |
6 (0- 19) |
||
BDI grades |
|
138 (34.5%) |
64 (64%) |
< 0.001** |
|
121 (30.2%) |
30 (30%) |
||
|
95 (23.8%) |
6 (6%) |
||
|
46 (11.5%) |
0 (0%) |
||
*Mann-Whitney-U test was used to compare the median difference between groups **Chi-square test was used to compare the difference in proportions between groups
Acne patients taking systemic retinoids alone or combined with systemic antibiotics had significantly higher frequencies of depression compared to those taking systemic antibiotics only or topical acne treatment (Table 4).
Table 4: Relationship between type of systemic treatment and depression (n=197).
Item |
None/Minimal |
Depressed |
P-value |
Systemic treatment |
|
|
0.020* |
|
40 (38.5%) |
64 (61.5%) |
|
|
16 (27.6%) |
42 (72.4%) |
|
|
2 (20.0%) |
8 (80.0%) |
|
|
2 (8.0%) |
23 (92.0%) |
*Chi-square test was used to compare the difference in proportions between groups
The frequency of depression was significantly higher with higher grades of acne severity according to GAGS. The mean duration of acne was significantly higher in depressed patients. The frequency of depression was significantly higher in nontreated patients compared to treated patients and in patients with positive family history of acne compared to those without (Table 5).
Table 5: Clinical Predictors of BDI in Acne Patients (n=400).
Item |
Non/Minimal |
Depressed |
P-value |
||
GAGS Score |
Mean ± SD |
17.16 ± 5.8 |
20.75 ± 8.9 |
< 0.001* |
|
Severity grades |
|
84 (41.4%) |
119 (58.6%) |
|
|
|
|
53 (37.9%) |
87 (62.1%) |
< 0.001** |
|
|
|
1 (1.8%) |
56 (98.2%) |
|
|
Duration/years |
Mean ± SD |
1.16 ± 0.1 |
1.87 ± 0.1 |
< 0.001* |
|
Treatment |
|
60 (30.5%) |
137 (69.5%) |
0.049** |
|
|
78 (38.4%) |
125 (61.6%) |
|||
|
36 (22.5%) |
124 (77.5%) |
|||
Post-acne complications (n=242) |
|
23 (20.9%) |
87 (79.1%) |
0.490** |
|
|
1 (50%) |
1 (50%) |
|
||
|
23 (28.8%) |
57 (71.2%) |
|
||
|
11 (22%) |
39 (78%) |
|
||
*T-test was used to compare the mean difference between groups **Chi-square test was used to compare the difference in proportions between groups
The final logistic regression model for BDI depression predictors, the adjusted odds ratio is significantly higher among patients with severe GAGS (AOR=41.7), thus, acne severity is the first significant predictor. The second predictor was systemic retinoid (AOR=4.09). Presence of complications wasn’t a significant predictor for depression (Table 6).
Table 6: Final Logistic Regression Model for BDI Predictors.
Predictor |
AOR** |
95% CI** |
LRT+ P-value |
Disease duration |
1.22 |
1.01 – 1.48 |
0.046 |
Systemic retinoids |
4.09 |
1.38 – 12.18 |
0.011 |
GAGS score |
1.07 |
1.03 – 1.11 |
0.001 |
Severity (Mild) |
1 (Reference) |
|
0.004 |
Severity (Moderate) |
1.09 |
0.46 – 2.56 |
0.845 |
Severity (Severe) |
41.70 |
3.45 – 91.76 |
0.003 |
Post-acne complications |
|
|
|
|
1 (Reference) |
|
0.570 |
|
0.25 |
0.02 – 3.50 |
0.353 |
|
0.66 |
0.34 – 1.28 |
0.214 |
|
0.94 |
0.42 – 2.11 |
0.867 |
**AOR=Adjusted Odds Ratio, CI= Confidence Interval +LRT=Likelihood Ratio Test
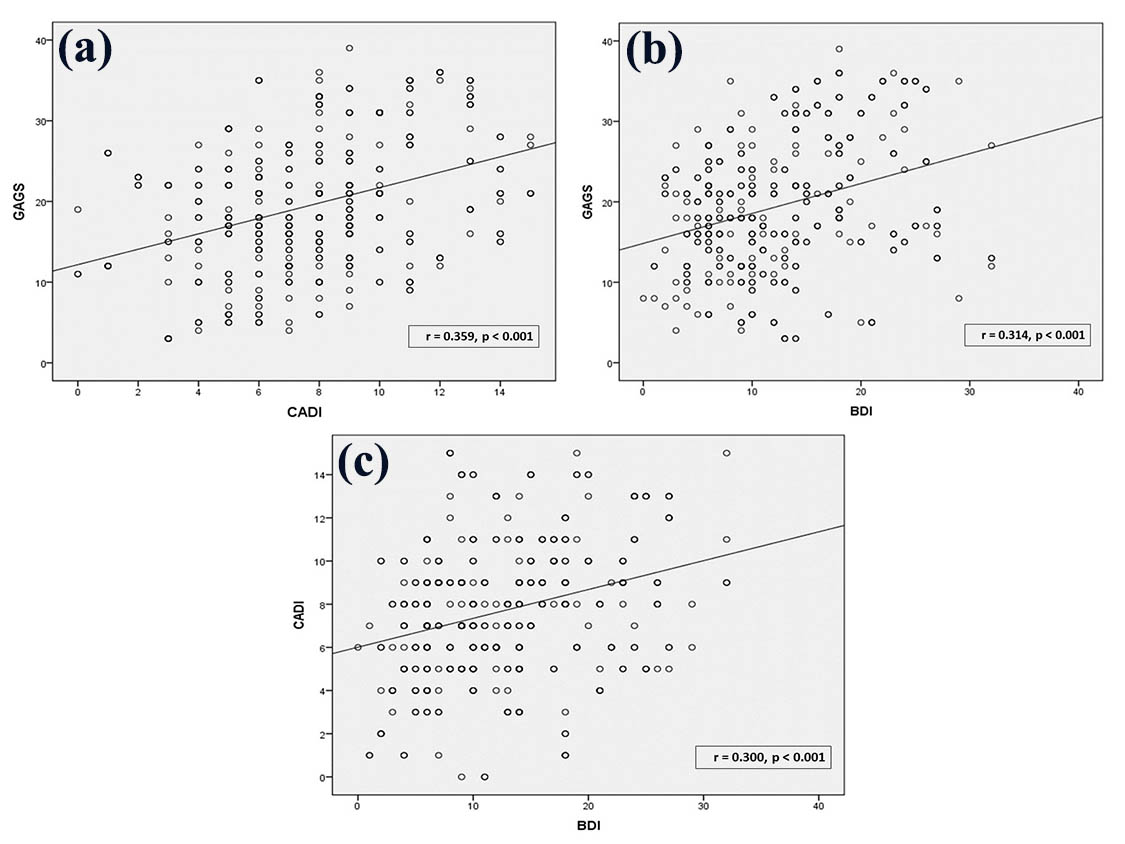
In our study, we found significant positive correlations between GAGS and CADI scores, GAGS and BDI scores and CADI and BDI scores (r= 0.359; p< 0.001, r= 0314; p< 0.001and r=0.300; p< 0.001 respectively) (Figure 1).
Discussion
Acne vulgaris is a common chronic skin disease among adolescents and young adults of both sexes [13]. The psychological and social impacts of acne are a matter of serious concern. This occurs in view of the fact that acne affects adolescents at a crucial stage of life when they are developing their personalities [14].
Most of published studies assessing QOL and depression in acne patients used the less specific questionnaire (DLQI index) rather than the more specific CADI3 or focused on depression with isotretinoin therapy [10].
This study was a cross sectional study aimed to determine the effect of acne and its severity in addition to some other acne variables on QOL and depression among affected Egyptian patients in Upper Egypt. We assessed QOL in acne patients using CADI the specific acne questionnaire in acne patients and depression using BDI in both patients and controls. In addition we objectively assessed acne severity with GAGS score in acne patients.
On the basis of our findings, the total mean of CADI score was 7.69. It was higher than that reported in other previous studies using the same scale where they reported a mean CADI score of less than 6.5 [8,15-17].
We found a significant correlation between impairment of QOL based on CADI score and acne severity measured by GAGS. Furthermore, severe acne was also found to be the main risk factor for poor QOL with acne patients. This was also inconsistent with other studies using CADI score [4,18]. Similarly, Abdelhafez et al., 2009, reported significant positive correlation between the severity of illness and Dermatology Life Quality Index (DLQI) scale [3]. On the other hand, a study done by Ogedegbe and henshaw in 2014 found that severity of acne measured with GAGS had weak correlation with QOL measured with CADI. However, most of included patients in that study were adolescents with mild acne vulgaris that may have a mild impact on QOL [17].
The presence of mixed acne complications including scars and pigmentation was the third predictor for impairing QOL of acne patients in our study. Similarly, a study using DLQI scale showed that post-acne scars have a significant negative effect on the QOL of young adults and highlighted the need to increase public awareness of acne vulgaris and its sequelae through education programs and advocating early treatment to reduce the risk of scarring [19]. A previous study reported the negative effect of post-inflammatory hyperpigmentation by acne on selfimage and QOL measured by CADI scale [20]. Another study using CADI scale in Nigeria reported poor QOL and impaired self-esteem in acne associated with facial hyperpigmentation and recommended that dermatologists should routinely assess the QOL and give attention to treatment of acne complications of facial post-inflammatory hyperpigmentation [21].
In our study, the mean of BDI scale reported in acne patients was 12.56 which was significantly higher than that of controls 6.92. Our mean BDI is less than that mentioned in acne patient by Jagtiaini et al [22]. which was 22.57 and higher than that reported in another previous study [23]in acne patients taking systemic retinoids and was 3.57. Furthermore, Hughes et al, 1983, found a higher prevalence of psychiatric disorders including depression in acne patients compared to general populations [24]. On the other hand, the results of some other studies that measured the degree of depression with acne by Hospital Anxiety and Depression Scale (HADS) were contradictory [25].
In the present study, BDI scale was significantly correlated with acne severity by GAGS and acne severity was the most significant predictor for presence and severity of depression with acne. Similar results were also reported in other previous studies [26-28].
We found depression in more than 80% of acne patients on systemic retinoids, a percentage that was significantly higher than in those on topical or on systemic antibiotics without retinoids. This percentage of depression was also higher than that reported in other study with average of 50% [31]. Furthermore, systemic retinoids are the third most significant predictor for depression in our study. However, we can't conclude if the increase in depression in group of systemic retinoids is related to isotretinoin intake or other significant factors especially higher acne severity in those patients since, systemic treatment in general was also a significant positive predictor for depression in the present study.
Depression and suicidal ideation with isotretinoin therapy in acne was a matter of a major concern in published studies with controversial results [10]. There are some studies which have shown the relation between isotretinoin and depression but have called it an idiosyncratic phenomenon and some others have suggested treating patients for both acne and depression [32,33]. In contrast, both Ng et al., 2002 and Simic et al, 2017, found no increase in depressive symptoms in patients on oral isotretinoin therapy [23,34]. Furthermore, some studies stated that isotretinoin, via its therapeutic benefits, improves mood and decreases depression with acne [35,36].
Prolonged acne duration in our study correlated with frequency of severe depression. Thus, acne chronicity can be a factor contributing to depressive features as demonstrated in other studies [26,27].
Despite its significant impact on QoL in our study, presence of acne complications showed higher but insignificant increase in frequency of depression that didn't predict depression with other variables in logistic regression analysis. However, other studies found that acne complications especially scarring are major predictors for depression with acne [28,30,36]. Again, the difference between studies may be due to variation in selection criteria and other stronger patient and disease factors between studies.
Our study combined two psychometric scales in evaluating the effect of acne and its severity on both QOL which was assessed by CADI and depression which was assessed by BDI. We found a positive significant correlation between the 2 psychometric tests and also between the tests and the severity scale. This indicates that patients with high CADI score (worse QOL) are more susceptible to have more depression than patient with lower CADI score. Also, the degree of both patterns of psychiatric illness correlated with acne severity.
Conclusion
Severity of acne and its complications have strong positive correlation with psychiatric condition of the patients that necessitate psychiatric assessment and early management of the affected patients.
References
- Martin A, Lookingbill D, Botek A, Light J, Thiboutet D, Girman C. Health-related quality of life among patients with facial acne assessment of a new acne-specific questionnaire. Clinical and experimental dermatology. 2001; 26: 380-385.
- Walker N, Lewis-Jones MS. Quality of life and acne in Scottish adolescent schoolchildren: use of the Children’s Dermatology Life Quality Index and the Cardiff Acne Disability Index. JEADV. 2006; 20: 45–50.
- Abdel-Hafez K, Mahran AM, Hofny ER, Mohammed KA, Darweesh AM, Aal AA. The impact of acne vulgaris on the quality of life and psychologic status in patients from Upper Egypt. International journal of dermatology. 2009; 48: 280-285.
- Ismail KH, Mohammed-Ali KB. Quality of life in patients with acne in Erbil city. Health and quality of life outcomes. 2012; 10: 60.
- Yap FBB. The impact of acne vulgaris on the quality of life in Sarawak, Malaysia. Journal of Saudi Society of Dermatology and Dermatology Surgery. 2012; 16: 57-60.
- Tasoula E, Gregoriou S, Chalikias J, Lazarou D, Danopoulou I, et al. The impact of acne vulgaris on quality of life and psychic health in young adolescents in Greece: Results of a population survey. Anais brasileiros de dermatologia. 2012; 87: 862-869.
- Doshi A, Zaheer A, Stiller MJ. A comparison of current acne grading systems and proposal of a novel system. International journal of dermatology. 1997; 36: 416-418.
- Motley RJ, Finlay AY. Practical use of a disability index in the routine management of acne. Clinical and experimental dermatology.1992; 17: 1-3.
- Grahame V, Dick DC, Morton CM, Watkins O, Power KG. The psychological correlates of treatment efficacy in acne.Dermatology and Psychosomatics Dermatologie und Psychosomatik. 2002; 3: 119-125.
- Kontaxakis VP, Skourides D, Ferentinos P, Havaki-Kontaxaki BJ, Papadimitriou GN. Isotretinoin and psychopathology: A review. Annals of General Psychiatry. 2009;8(1):2.
- Arnau RC, Meagher MW, Norris MP, Bramson R. Psychometric evaluation of the Beck Inventory-II with primary care medical patients. Health Psychology. 2001; 20: 112. 12. Beck AT, Steer RA, Brown GK. Manual for Beck Depression Inventory-II. San Antonio, TX. Psychological corporation. 1996.
- Knutsen-Larson S, Dawson AL, Dunnick CA, Dellavalle RP. Acne vulgaris: pathogenesis, treatment, and needs assessment. Dermatologic Clinics. 2012; 30: 99-106.
- Sharmila TB, Antony JV, Jayakrishnan MP, Beegum PS, Thachil ET. Mechanical, thermal and dielectric properties of hybrid composites of epoxy and reduced graphene oxide/iron oxide. Materials & Design. 2016; 15: 66-75.
- Gupta A, Sharma YK, Dash KN, Chaudhari ND; Jethani S. Quality of life in acne vulgaris: Relationship to clinical severity and demographic data. Indian Journal of Dermatology, Venereology and Leprology. 2016; 82: 292.
- El-Khateeb EA, Khafagy NH, Elaziz KA, Shedid AM. Acne vulgaris: prevalence, beliefs, patients’ attitudes, severity and impact on quality of life in Egypt. Public health. 2014; 128: 576-578.
- Ogedegbe EE, Henshaw EB. Severity and impact of acne vulgaris on the quality of life of adolescents in Nigeria. Clinical, cosmetic and investigational dermatology. 2014; 7: 329.
- Abu El-Hamd M, Nada EE, Moustafa MA, Mahboob-Allah RA. Prevalence of acne vulgaris and its impact of the quality of life among secondary school-aged adolescents in Sohag Province, Upper Egypt. Journal of cosmetic dermatology. 2017; 16: 370- 373.
- Chuah SY, Goh CL. The impact of post-acne scars on the quality of life among young adults in Singapore. Journal of cutaneous and aesthetic surgery. 2015; 8: 153.
- França K and Keri J. Psychosocial impact of acne and post-inflammatory hyperpigmentation. Anais Brasileiros de Dermatologia. 2017; 92: 505-509.
- Akinboro AO, Ezejiofor OI, Olanrewaju FO, Oripelaye MM, Olabode OP, et al. The impact of acne and facial post-inflammatory hyperpigmentation on quality of life and self-esteem of newly admitted nigerian undergraduates. Clinical, cosmetic and investigational dermatology. 2018; 11: 245.
- Jagtiani A, Nishal P, Jangid P, Sethi S, Dayal S, Kapoor A. Depression and suicidal ideation in patients with acne, psoriasis, and alopecia areata. Journal of Mental Health and Human Behaviour. 2017; 22: 50.
- Ng CH, Tam MM, Celi E, Tate B, Schweitzer I. Prospective study of depressive symptoms and quality of life in acne vulgaris patients treated with isotretinoin compared to antibiotic and topical therapy. Australasian Journal of Dermatology. 2002; 43: 262–268.
- Hughes JE, Barraclough BM, Hamblin LG, White JE. Psychiatric symptoms in dermatology patients. The British Journal of Psychiatry. 1983; 143: 51-54.
- Golchai J, Khani SH, Heidarzadeh A, Eshkevari SS, Alizade N, et al. Comparison of anxiety and depression in patients with acne vulgaris and healthy individuals. Indian J Dermatol. 2010; 55: 352-354.
- Do JE, Cho SM, In SI, Lim KY, Lee S. Psychosocial aspects of acne vulgaris: a community-based study with Korean adolescents. Annals of dermatology. 2009; 21: 125-129.
- Kang L, Liu J, An R, Huang J, Huang H. Depression in patients with facial acne vulgaris and the influential factors. Zhong nan da xue xue bao. Yi xue ban Journal of Central South University. Medical sciences. 2015; 40: 1115-1120.
- Prakash P, Mohite A, Gautam P. A study of presence of depression in acne vulgaris patients. Global journal for research analysis. 2016; 5: 73-76.
- Niemeier V, Kupfer J, Demmelbauer-Ebner M, Stangier U, Effendy I, et al. Coping with acne vulgaris. Dermatology. 1998; 196: 108-115.
- Yazici K, Baz K, Yazici AE, Köktürk A, Tot S, Demirseren D, Buturak V. Disease-specific quality of life is associated with anxiety and depression in patients with acne. Journal of the European Academy of Dermatology and Venereology. 2004; 18: 435-439.
- Fakour Y, Noormohammadpour P, Ameri H, Ehsani AH, Mokhtari L, et al. The effect of isotretinoin (roaccutane) therapy on depression and quality of life of patients with severe acne. Iranian journal of psychiatry. 2014; 9: 237.
- Goodfield MJ, Cox NH, Bowser A, McMillan JC, Millard LG, Simpson NB, Ormerod AD. Advice on the safe introduction and continued use of isotretinoin in acne in the UK. British Journal of Dermatology. 2010; 162: 1172-1179.
- Misery L. Consequences of psychological distress in adolescents with acne. Journal of Investigative Dermatology. 2011; 131: 290- 292.
- Šimić G, Leko MB, Wray S, Harrington CR, Delalle I, JovanovMilošević N, Bažadona D, Buée L, de Silva R, Di Giovanni G, Wischik CM. Monoaminergic neuropathology in Alzheimer’s disease. Progress in neurobiology. 2017; 151: 101-138.
- Rubinow DR, Peck GL, Squillace KM and Gantt GG. Reduced anxiety and depression in cystic acne patients after successful treatment with isotretinoin. J. Am. Acad. Dermatol. 1987; 17: 25-32.
- Kellett SC, Gawkrodger DJ. The psychological and emotional impact of acne and the effect of treatment with isotretinoin. British Journal of Dermatology. 1999; 140: 273-282.