
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Inflammatory myoglandular colonic polyp with adenomatous changes mimicking malignant tumor
Sneha R Adidam1; Seenath M2; Chalapathi R Adidam Venkata3*
1 Resident Internal Medicine, Howard University Hospital, Washington DC, USA.
2 Consultant Surgeon, Eric Williams Medical Sciences Complex, Trinidad, WI
3 Professor of Pathology, University of the West Indies, Trinidad, WI.
*Corresponding Author: Chalapathi Rao Adidam
Venkata
Professor of Pathology, UWI, St.Augustine Trinidad,
West Indies.
Email: avcraouwi@gmail.com
Received : Sep 03, 2021
Accepted : Oct 06, 2021
Published : Oct 13, 2021
Archived : www.jcimcr.org
Copyright : © Chalapathi RAV (2021).
Abstract
Inflammatory Myoglandular polyps (IMGPs) are rare intestinal polyps that occur frequently in the left colon and may present with hematochezia. Only a small number of cases have been reported in the right colon (2%). We present a case of IMGP in the proximal ascending colon. A 46-year-old woman of mixed ethnicity presented with a history of abdomino-pelvic pain and constipation. CT scan suggested possibility of malignancy. On colonoscopy, a non- obstructive polyp in proximal ascending colon was biopsied followed by right hemicolectomy. Patient also underwent total abdominal hysterectomy at the same time for fibroids. The colonic polyp revealed features of IMGP with focal adenomatous changes. The polyp was characterized by epithelial erosion, inflamed granulation tissue, hyperplastic and dilated glands, and proliferating smooth muscle. IMGP needs to be distinguished from other non-neoplastic colonic polyps, which includes Peutz-Jeghers polyps, inflammatory pseudopolyps, juvenile polyps, and inflammatory fibroid polyps. We report a large sized inflammatory myoglandular polyp with suspicious imaging findings and presence of adenomatous changes that mimicked malignancy that requires comprehensive evaluation and follow up.
Keywords: inflammatory myoglandular polyp; adenomatous changes; non-neoplastic; malignancy
Citation: Adidam SR, Seenath M, Chalapathi RAV. Inflammatory myoglandular colonic polyp with adenomatous changes mimicking malignant tumor. J Clin Images Med Case Rep. 2021; 2(5): 1358.
Introduction
Inflammatory Myoglandular Polyp (IMGP) is an uncommon but distinct, non-neoplastic type of colorectal polyp with a predilection for distal localization and with rare occurrence in proximal (right) colon [1-6,11]. The distinctive histopathological features of the polyp were first described in 1992 by Nakamura and his colleagues [2]. The typical endoscopic appearance looks like a ripe strawberry with areas of redness, smooth rounded surface and has a stalk [10]. Patchy mucous exudates may be visualized. Till date fewer cases have been reported. The aetiopathogenesis and natural history remains unclear [1,3]. Inflammatory myoglandular polyps have similar presenting features of juvenile polyps, inflammatory polyps, Peutz-Jegher-type polyps, inflammatory polyps, and polyps associated with mucosal prolapse. Therefore, inflammatory myoglandular polyps have to be distinguished as a distinct entity and must also exclude malignant polyps. We describe clinical and histological features of an inflammatory myoglandular polyp in the proximal ascending colon that mimicked a malignant polyp.
Case report
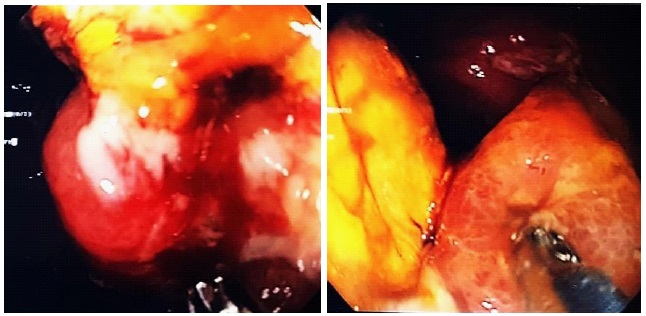
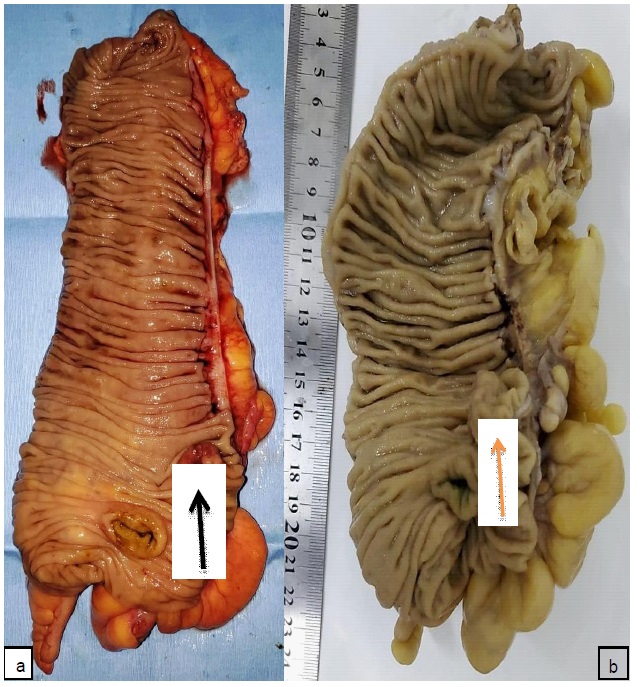
A 46-year-old woman of mixed ethnicity presented with a history of constipation and change in bowel habit. Past medical and family history did not reveal chronic colitis, diverticular disease or polyposis. Laboratory blood tests revealed normal CBC; Hb: 11.1 g/dL, WBC: 8.41 X 103 /µL, normal differential count and Platelet: 385 X 103 /µL. Physical examination revealed no abnormal findings. CT scan of chest and abdomino-pelvis was performed. Chest findings were normal. A mildly enhancing mass in the ascending colon just distal to the ileo- cecal junction was noted. It appeared to involve the muscularis propria and subserosa but mesenteric fat stranding or nodularity was not seen. Three sub-centimeter mesenteric nodes ranging in size from 2 mm to 7 mm were identified. Overall radiological findings suggested likely malignant tumor. Pelvis revealed enlarged uterus measuring 15.6 X 10.2 cm containing intramural fibroids. Both adnexa were normal. The colonoscopy revealed ascending colon was displaced due to large uterine fibroids. A non-obstructing malignant-appearing mass was identified (Figure 1) and multiple biopsies were taken. Remainder of the colorectum had NO polyps or significant findings. Biopsy was reported as tubular adenoma with erosion along with additional findings of hyperplastic crypts, inflamed granulation tissue and necro- inflammatory debris. There was NO evidence of malignancy or high grade dysplasia. Patient underwent Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy and Right Hemicolectomy. Gross and microscopy of hysterectomy confirmed leiomyomata. Both adnexa and cervix had no significant findings. The colon measured 18.5 cm in llength ileum measured 2.8 cm and appendix was 5.5cm in length. A polypoid growth with a short stalk, which measured 2 X 2 X 1.3 cm, was identified 1 cm distal to ileo-cecal opening. Cut sections of the polyp showed grey-white areas and thickening of wall of the colon at the site of growth. Appendix, ileum and rest of the colon and cecum appeared normal (Figure 2a,b&c). Microscopy of the polyp showed focal mucosal erosion, granulation tissue, and dense mixed inflammatory cells in the lamina propria with predominance of lympho-plasmacytic cells.

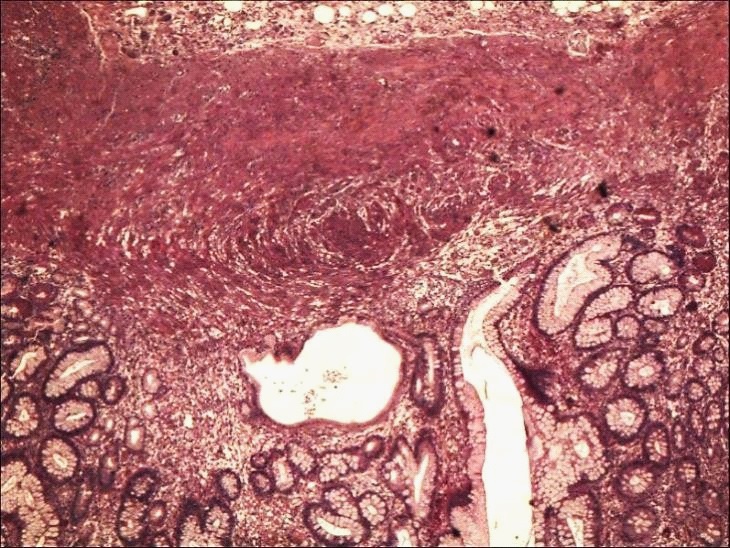
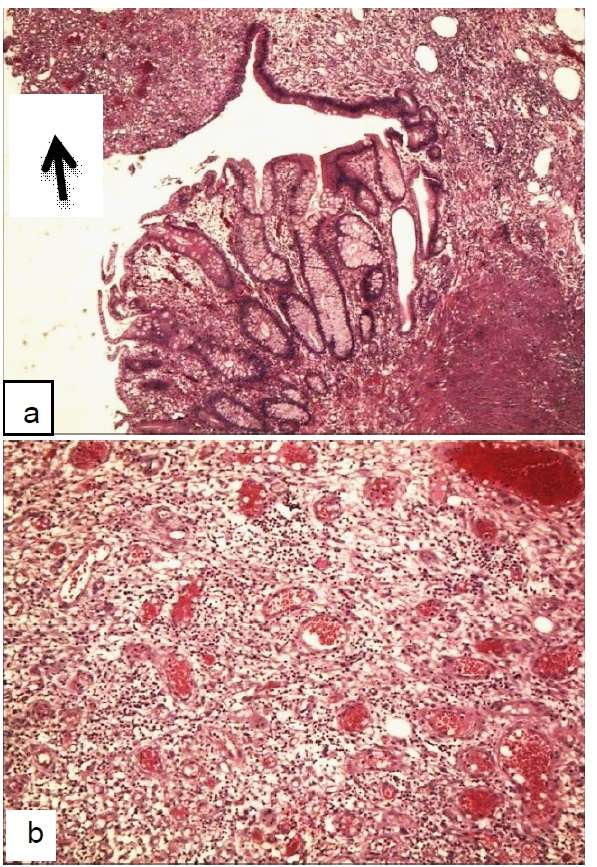
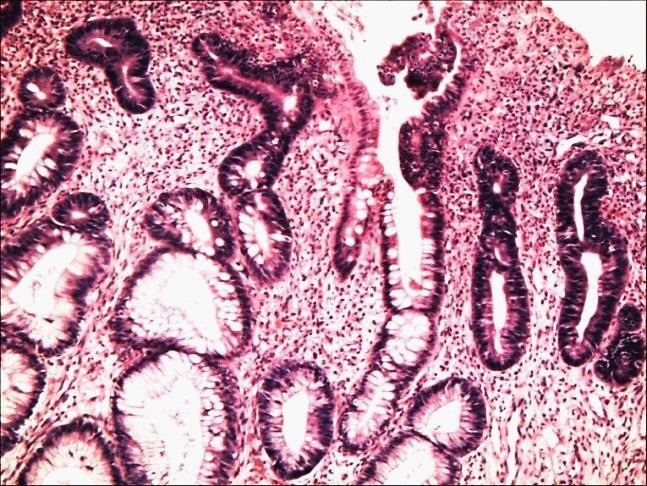
Foamy histiocytes and a few eosinophils were noted. Inflammation extended to submucosa. Mucosa of the polyp, adjacent to erosion, showed hyperplasia and focal dilated crypts. Muscularis mucosa showed marked thickening. Muscularis propria was also hypertrophic. Focal adenomatous changes with mild dysplasia were noted. There was NO evidence of malignancy or high grade dysplasia. A diagnosis of Inflammatory Myoglandular Polyp with Adenomatous changes was made (Figure 3-5).
Discussion
IMGP is a rare benign polyp of unknown etio-pathogenesis (also termed “Nakamura polyp”), usually presenting as a solitary mass in the gastrointestinal tract [1-6]. More often, it is seen in adults of both sexes ranging from 20-60 years and rarely in children [14]. Three main histological features of IMGP were first described in 1992 by Nakamura and colleagues. They include “1) inflammatory granulation tissue in the lamina propria; 2) proliferation of smooth muscle from the muscularis mucosae; 3) hyperplastic glands with occasional cystic dilatation” [2]. These findings were typically observed in our case. 68 cases were reported in the literature according to Becheanu G et al in 2011 [4]. Literature review of Medline/Pubmed revealed an additional fourteen (14) cases reported until 2021. IMGPs can be asymptomatic and are identified incidentally [1], whereas the most common symptom is hematochezia [1,5,7-10,12,13], or positive fecal occult blood [1], and anemia [1]. Other presenting symptoms may include abdominal pain and constipation [1,8]. In our case, the patient was an adult female investigated for abdomino-pelvic pain, constipation and altered bowel habits.
L Jiang and Y F Jiao studied 1190 cases of non-neoplastic colorectal polyps. Inflammatory myoglandular polyps accounted for 0.6% [13]. IMGP is typically described as a solitary lesion involving large bowel, mostly located in the left colon with the exception of the polyp in the terminal ileum reported by Griffiths et al [6,8,15]. Incidence of IMGP in ascending colon ranges from 1.5-3% [4]. Our case was a solitary lesion with a short stalk in the proximal ascending colon. Multiple inflammatory myoglandular polyps occurring in a single patient have been reported [8].
Pathogenesis and natural history of IMGP is unclear. It is hypothesized to be associated with local trauma, mucosal prolapse, ischemia, chronic inflammation due to fecal stasis and abnormal colonic motility [2,4,7]. IMGP is not associated with inflammatory bowel disease [8].
Endoscopic findings of IMGP include short or distinct peduncle, a red, smooth, rounded, and patchy reddish surface. Patchy mucosal exudation and erosion may be present [5,7,8,10].
According to the reports in the literature, IMGP is considered clinically and histologically benign with no malignant potential hence endoscopic treatment is currently the gold standard. Kayhan et al. had performed a left hemicolectomy due to the large polyp size of more than 6cm and is an exceptional case [1,12,9]. In our case, considering the size of the polyp and CT scan findings, which mimicked malignant polyp, an initial biopsy followed by right hemicolectomy was performed along with hysterectomy. The diagnosis of IMGPs could often be made by biopsy, as in two of the reported cases. Biopsy alone may not provide accurate diagnosis as specimen would be superficial and does not reflect muscular proliferation [1,3,4]. Histological findings in the present case reflected features of IMGP with adenomatous changes. Examination of the polypectomy specimen is ideal to delineate definitive histological features.
The differential diagnosis includes other non-neoplastic polyps, which could have some common histological features with IMGP: Inflammatory polyp, juvenile polyp, polyp secondary to prolapse syndrome, inflammatory “Cap” polyp, Peutz-Jeghers polyp and inflammatory fibroid polyp [7]. In our case in addition to typical histological findings of IMGP, focal adenomatous changes were noted (Figure 5). This is an unusual finding not reported hitherto and thus warrants comprehensive evaluation and surveillance.
Conclusion
The aim of this paper is to report the first case of IMGP with adenomatous changes at an uncommon location of ascending colon. It is usually a solitary benign lesion of unknown etiopathogenesis and natural history affecting adults and has distinct histopathological features. It must be distinguished from neoplastic and other non-neoplastic polyps of the large bowel. Symptomatic IMGP should preferably be removed endoscopically, whereas surgical resection may be reserved for select patients, as in our case, where large size of polyp with suspicious imaging findings and presence of adenomatous changes mimicked malignancy and required comprehensive evaluation.
Declarations
Consent: All authors have consented for publication.
Funding: Not funded by any external source.
Contributions
1. SA: was involved in the literature search, review of manuscript, proof reading and referencing
2. MS: was involved in the review of the manuscript and in the surgical management of the case.
3. CRAV: Conceptualization, diagnosis, and preparation of the manuscript.
References
- Roberto L Meniconi, Roberto Caronna, Michele Benedetti, et al. Inflammatory myoglandular polyp of the cecum: case report and review of literature. BMC Gastroenterology. 2010; 10: 10.
- S Nakamura, I Kino, T Akagi. Inflammatory myoglandular polyps of the colon and rectum. A clinicopathological study of 32 pedunculated polyps, distinct from other types of polyps. Am J Surg Pathol. 1992; 16: 772-9.
- Shoji Hirasaki, Hiromitsu Kanzaki, Minoru Matsubara et al. Inflammatory Myoglandular Polyps: A Case Series of Four Patients and Review of the Literature”, Gastroenterology Research and Practice. 2010; 984092.
- Becheanu G, Gheorghe C, Dumbravă M, et al. Inflammatory myoglandular colorectal polyps: A series of seven cases and review of literature. Chirurgia (Bucur. 2011; 106: 613-7.
- Moriyama T, Matsumoto T, Hizawa K. Tada S. Fuchigami T. et al. Inflammatory Myoglandular Colorectal Polyps: A Case Series of Nine Patients. Endoscopy. 2003; 35: 363 - 365
- Arslan Ahmad, Sonali Lanjewar, Khurram Shafique et al. Inflammatory Myoglandular Polyp of the Ascending Colon: Case Report and Review of Literature. American Journal of Clinical Pathology. 2016; 146.
- M Tashiro, I Yoshikawa, T Matsuhashi, et al. Gastrointestinal: Inflammatory myoglandular polyp of the colon. Journal of gastroenterology and hepatology. 2005; 20: 7.
- WH Siow, G Hawken, A Russell et al. Gastrointestinal: Multiple inflammatory myoglandular polyps in a single patient. Journal of gastroenterology and hepatology. 2015.
- Kayhan B, Kucukel F, Akdogan M, et al. Inflammatory myoglandular polyp: a rare cause of hematochezia. Turk J Gastroenterol. 2004; 15: 117- 119.
- Sook Hee Chung, Byoung Kwan Son, Young Sook Park. et al. Inflammatory Myoglandular Polyps causing Hematochezia. Gut and Liver. 2010; 4: 146-148.
- Gabriel Becheanu, BernhardStamm. Inflammatory Myoglandular Polyp – A Rare but Distinct Type of Colorectal Polyps. Pathology - Research and Practice. 2003; 199: 837-839
- Kanzaki H, Hirasaki S, Okuda M, et al. Lobulated inflammatory myoglandular polyp in the ascending colon observed by magnifying endoscopy and treated with endoscopic polypectom y. World J Gastroenterol. 2008; 14: 4838 - 484.
- Jiang L, Jiao YF. Clinicopathological features of non-neoplastic colorectal polyps. Zhonghua Bing Li Xue Za Zhi. 2019; 48: 98- 101.
- Mitra S, Sable M, Sahoo SK, et al. Rectal Inflammatory Myoglandular Polyp with Osseous Metaplasia in a Child. Fetal Pediatr Pathol. 2020; 10: 1-5.
- Griffiths AP, Hopkinson JM, Dixon MF: Inflammatory myoglandular polyp causing ileo-ileal intussusception. Histopathology. 1993; 23: 596-598.