
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Gossypiboma: A case report
KO Alabi1; SB Fayose2; AI Akinwumi1; A Adeyeye3*
1 Department of Family Medicine, Afe Babalola University, Ado-Ekiti, Nigeria
2 Department of Surgery, Afe Babalola University Multi-System Hospital, Ado-Ekiti, Nigeria.
3 Department of Surgery, Afe Babalola University, Ado-Ekiti, Nigeria.
*Corresponding Author: A Adeyeye
Department of Surgery, Afe Babalola University,
Ado-Ekiti, Nigeria.
Email: adeyeye_ademola@yahoo.com &
adeyeyea@abuad.edu.ng
Received : Sep 03, 2021
Accepted : Oct 06, 2021
Published : Oct 13, 2021
Archived : www.jcimcr.org
Copyright : © Adeyeye A (2021).
Abstract
This case underscores the need for clinicians to bear the possibil‑ ity of gossypiboma in mind when patients who have had abdominal surgery in the recent past present with unresolving abdominal pain.
This 46 year old woman who had an elective hysterectomy done three months earlier presented with unresolving abdominal pain of three months and lower abdominal distension of a day duration. Fol‑ lowing exploratory laparotomy, an 18 cm by 18 cm towel was recov‑ ered from her peritoneal cavity. She subsequently developed fecal fistula which was successfully managed conservatively and was dis‑ charged in good condition on 20th post-operative day.
Gossypiboma is a rare but grave complication of abdominal and pelvic surgeries with attendant significant morbidity or even mortal‑ ity. Adequate attention to patient care processes may reduce its oc‑ currence and high index of suspicion is needed for its diagnosis.
Keywords: abdominal sponge; gossypiboma; intra‑abdominal.
Citation: Alabi KO, Fayose SB, Akinwumi AI, Adeyeye A. Gossypiboma: A case report. J Clin Images Med Case Rep. 2021; 2(5): 1359.
Introduction
Retained surgical item is a term used to describe any surgi‑ cal sponge, instrument, tool or device left unintentionally in a patient after a surgical procedure is completed and the wound closed [1]. A surgical sponge accidentally retained inside the body of a patient after surgery is referred to as gossypiboma [2] and pathologically, it may lead to two types of foreign body reaction - exudative reaction leading to abscess formation or granuloma formation from aseptic fibrinous response [3].
Reporting this case serves to remind clinicians of retained surgical item as a possible cause of unrelenting post-operative abdominal pain.
Case report
This was a 46 year old multiparous woman who had total abdominal hysterectomy in a peripheral hospital three months prior to presentation. Post-operatively, she had presented sev‑ erally to the hospital on account of a nagging abdominal pain which defiled conventional treatment. The pain became severe a day prior to presentation with lower abdominal distention and fever. There was no history of vomiting, diarrhea, constipa‑ tion or abnormal vaginal discharge. She had no known under‑ lying chronic medical condition or any psycho-social or family history of note.
On examination, she was ill-looking and in obvious painful distress. She was febrile (T- 40.30C), dehydrated, pale but an‑ icteric. Her abdomen was moderately distended and tender especially at the lower part around the previous pfannenstiel incision scar (Figure 1). Digital rectal examination revealed a bulging and tender anterior rectal wall.

The results of the initial laboratory work-up showed a septic picture and an abdomino-pelvic ultrasound scan done reported a cystic intra-abdominal mass with reduced bowel movement.
An initial diagnosis of post-operative intra-abdominal abscess was made to keep in view Gossypiboma. She was placed on nil per os, intravenous fluids, intravenous antibiotics, parenteral antipyretics and she was prepared for an urgent exploratory laparotomy.
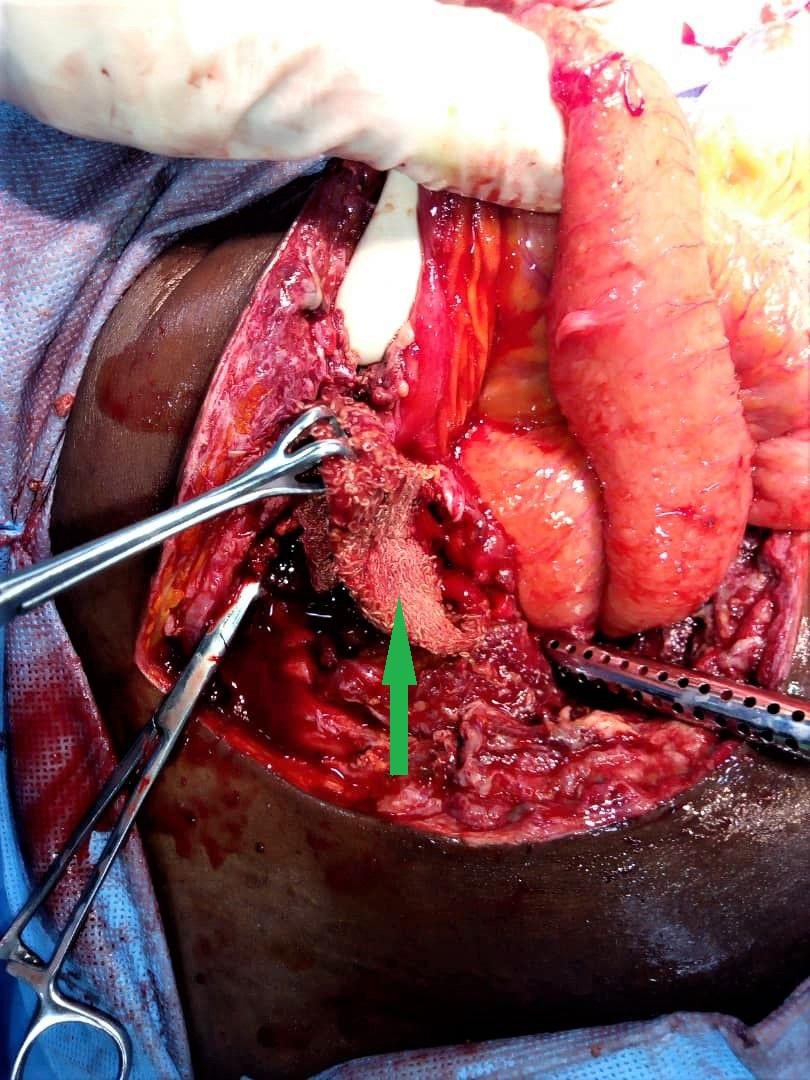
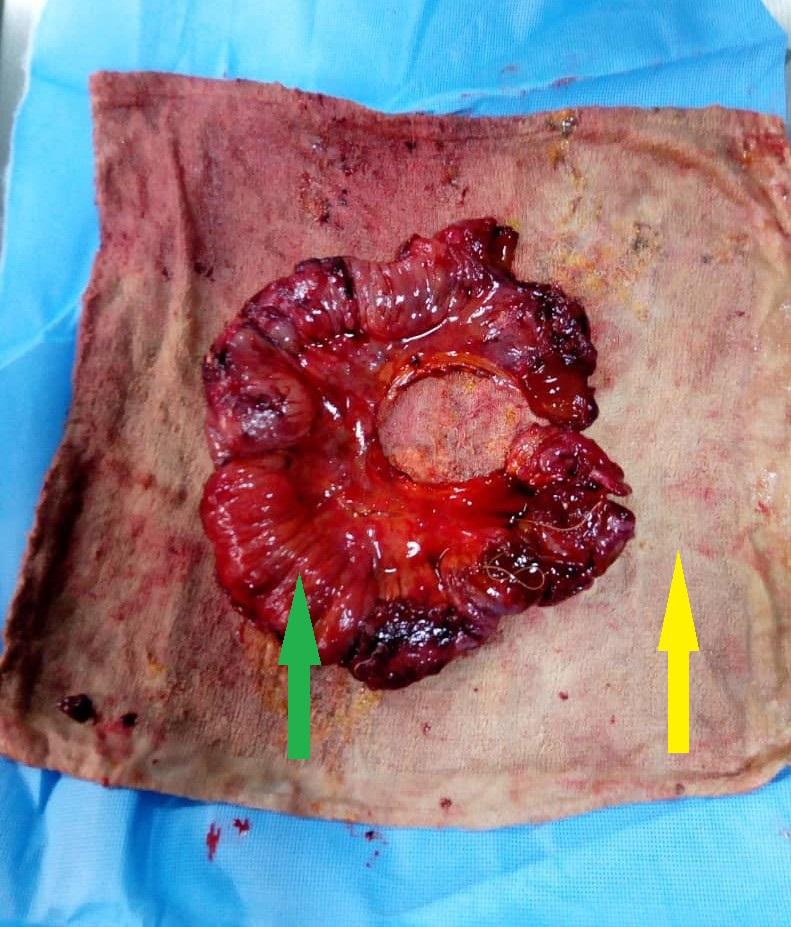
At laparotomy, about 500 mls of purulent peritoneal fluid was suctioned out. There was a complex mass comprising of multiple matted loops of ileum, caecum, part of the omentum and an abdominal sponge measuring 18 X 18 cm (Figure 2). Af‑ ter the retained sponge was carefully dissected out and other components of the mass separated, three areas of perforation were noted on the distal part of the ileum at 54 cm, 66 cm and 70 cm from the ileo-caecal junction respectively.
A resection of about 20 cm of ileum with end-to-end anasto‑ mosis was done to establish bowel continuity (Figure 3).
She had a fairly stable post-operative state but developed a low-output entero-cutaneous fistula which was managed conservatively with complete cessation of faecal discharge two weeks later. She was thereafter discharged to continue wound dressing on outpatient basis. Two weeks later, she was seen in the clinic with a completely healed wound.
Discussion
Patil et al., in a review reported the incidence of retained surgical sponge to be one per 100–3000 operations [4], how‑ ever, this might be underreported to avert adverse publicity and medico-legal problems, thus, the true incidence of gossypibo‑ ma may never be known.
The risk for gossypiboma has been found to be higher in emergency surgeries, prolonged surgeries, surgeries involv‑ ing more than one major procedure or more than one surgical team, improper or incorrect surgical swab counts, unexpected intraoperative occurrences and high intraoperative blood loss [5]. Since practically nothing was known about the initial sur‑ gery the patient had (except that it was an elective hysterec‑ tomy), the occurrence of any of these risk factors could not be ascertained.
Patients with gossypiboma may have early or delayed pre‑ sentation or at times be asymptomatic. Possible clinical pre‑ sentations and complications include pain or irritation in the abdomen, palpable mass, fever, sepsis, visceral perforation, penetration, obstruction, abscess formation, fistulae formation, intraluminal migration and death [6,7]. The index patient had many of these complications but survived them.
Imaging is of great significance in diagnosing retained for‑ eign objects following surgery. Computed tomography scan might report a well circumscribed mass with a thick wall, with or without gas in cases of gossypiboma, although, changes such as calcifications, air-bubbles and oedema may lead to confusion in its appearance [8,9]. An abdomino-pelvic ultrasound scan done in this patient reported a cystic mass with reduced bowel movement; this finding did not heighten the suspicion of gos‑ sypiboma before the surgery but was somewhat consistent with intraperitoneal fluid collection found intra-operatively. Accord‑ ing to a review by Malhotra [6], abdominal ultrasound is less sensitive (34%) when compared with CT scan (61%) as a way of detecting gossypiboma. The choice of abdomino-pelvic scan in this patient was premised on affordability and need for urgent intervention.
As demonstrated in this case report, the definitive way of managing suspected or confirmed gossypiboma is to reopen the cavity where the sponge was retained. In a report by BaniHani et al., in order to remove the retained surgical sponge and manage the resulting complications (bowel obstruction and fis‑ tulae), ten out of eleven (91%) patients required a reoperation [7].
Although human errors cannot be totally eliminated, very strict adherence to safety regulations can reduce the incidence of gossypiboma to a barest minimum [7]. Efforts to improve care processes, standardized count protocols, deliberate wound ex‑ ploration by the surgeon before closure and resolving count dis‑ crepancies should be put in place [1]. Also, the use of radiologi‑ cally detectable sponges (Ray‑tec sponges) and towels should be encouraged as much as possible [2]. Furthermore, the use of electronic article surveillance system and barcode scanner in relation to intra-operative surgical sponge use have been advo‑ cated [10]. However, because of paucity of these technologies in many developing countries, manual surgical sponge counting is still valuable and should be meticulously done before and af‑ ter surgical procedures and abdominal packs should always be tagged [1].
Conclusion
Gossypiboma is rare but has debilitating consequences in‑ cluding death and an unrelenting post-operative abdominal pain may signal its presence. However, paying adequate atten‑ tion to patient care processes and operating room environment may reduce its occurrence.
References
- Roberts OA, Afuwape OO. Intra abdominal gossypiboma with feacal fistula, laparotomy, removal and drainage. Trop J Obstet Gynaecol. 2016; 33: 250-253.
- Boghratian AH, Al-Taee AM. Gossypiboma masquerading as small bowel malignancy. Middle East J Dig Dis. 2020; 12: 123.
- Choi BI, Kim SH, Yu ES, Chung HS, Han MC, Kim CW. Retained surgical sponge: diagnosis with CT and sonography. AJR Am J Roentgenol. 1988; 150: 1047-1050.
- Patil KK, Patil SK, Gorad KP, Panchal AH, Arora SS, Gautam RP. Intraluminal migration of surgical sponge: gossypiboma. Saudi J Gastroenterol. 2010; 16: 221.
- Maranya G, Maganga H, Mwero B. Gossypiboma of the Abdo‑ men and Pelvis; A Recurring Error. Ann. Afr. Surg. 2017; 14.
- Malhotra MK. Migratory Surgical Gossypiboma - Cause of Iatro‑ genic Perforation: Case Report with Review of Literature. Niger J Surg. 2012; 18.
- Bani-Hani KE, Gharaibeh KA, Yagha RJ. Retained surgical sponges (gossypiboma). Asian J. Surg. 2005; 28: 109-115.
- Umunna JI. Gossypiboma and its implications. J West Afr Coll Surg. 2012; 2: 95.
- Malik A, Jagmohan P. Gossypiboma: US and CT appearance. In‑ dian J. Radiol. Imaging. 2002; 12: 503.
- Fabian CE. Electronic tagging of surgical sponges to prevent their accidental retention. Surgery. 2005; 137: 298-301.