
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Case report: Adenocarcinoma of the larynx with later hepatocellular differentiation
David G Symeonidis1; Alexandros-Nikolaos D Liatsos2; George I Papageorgiou1; Loukas Karelis3; Evangelos Lianos4; Christos Kosmas5
1 Resident of Medical Oncology, Metaxa Cancer Institute of Piraeus, Greece.
2 Resident of Nephrology, Evangelismos General Hospital, Athens, Greece.
3 Consultant Pathologist, Pathology Department, Metaxa Cancer Institute of Piraeus, Greece.
4 Consultant of Medical Oncology, Oncology Department, Metaxa Cancer Institute of Piraeus, Greece.
5 Medical Oncologist, Director of Oncology Department, Metaxa Cancer Institute of Piraeus, Greece.
*Corresponding Author: David G Symeonidis
Resident of Medical Oncology, Metaxa Cancer Institute of Piraeus, Symeonidis, Sparti 5 Keratsini, 18755,
Piraeus, Greece.
Email: davidsymeonidis@yahoo.com
Received : Sep 06, 2021
Accepted : Oct 06, 2021
Published : Oct 13, 2021
Archived : www.jcimcr.org
Copyright : © Symeonidis DG (2021).
Abstract
Head and neck cancer accounts for 3.5% of annual worldwide cancer diagnoses with the larynx being part of it. The main methods of treatment include laryngectomy, but mainly a combination of radiation with chemotherapy and then combinations of chemotherapy with immunotherapy in more advanced stages of the disease. Histologically it is mostly squamous cell carcinoma, but cases of glandular differentiation have been reported that favor the entry of these patients into clinical trials. In our case we discuss a patient diagnosed with adenocarcinoma to the larynx area treated initially with laryngectomy and radiotherapy. In metastatic setting, he received multiple treatment lines with chemotherapy and immunotherapy and a later biopsy from a paraspinal mass which pathology resulted in an adenocarcinoma from the larynx, with hepatocellular differentiation. We performed upper endoscopy which revealed a high-grade dysplasia and the initiation of irinotecan led to a rapid clinical deterioration.
Keywords: adenocarcinoma; larynx; hepatocellular; treatment.
Citation: Symeonidis DG, Liatsos AND, Papageorgiou GI, Karelis L, Lianos E, et al. Case report: Adenocarcinoma of the larynx with later hepatocellular differentiation. J Clin Images Med Case Rep. 2021; 2(5): 1360.
Introduction
Head and neck cancer accounts for 3.5% of annual worldwide cancer diagnoses with the larynx being part of it. There are 3 areas anatomically, supraglottis area, glottis which is the most common site of cancer and subglottis [1]. Fortunately, due to the symptoms (hoarseness), the diagnosis is often made in the early stages of the disease, and to a significant extent it is a curable disease. In fact, in the early stages of T1.2 there is rarely lymph node involvement, which gives additional benefit to the patient. On the other hand, supraglottis region cancer has a worse prognosis due to the late diagnosis but also because at the time of diagnosis there is already metastasis to local lymph nodes, which changes the treatment plans. The main methods of treatment include laryngectomy, but mainly a combination of radiation with chemotherapy and then combinations of chemotherapy with immunotherapy in more advanced stages of the disease [2,3]. Histologically it is mostly squamous cell carcinoma, but cases of glandular differentiation have been reported that favor the entry of these patients into clinical trials.
Case report
A 58-year-old patient with a 3-month hoarseness came to the hospital where, after an MRI scan, a tumor was found in the area of the larynx (T3) without abnormal lymph nodes, neither imaging nor clinically. The finding was confirmed by laryngoscopy. Laryngectomy was performed by local removal of 2 lymph nodes that were tumor naive. The tumor occupied the area of the tongue with extension to the sublingual space and with clear excision margins from above in the lower jaw and lower in the humerus and trachea. Irradiation followed in the area.
From the rest of his medical history was a 60 pack year smoker, without other diseases. Other clinical examination and laboratory findings without pathological findings.
Histological diagnosis confirmed the presence of low differentiation adenocarcinoma with positivity in the epithelial markers CK7, CK8-18 and negative expression of the markers CK5 / 6. The patient underwent follow-up and after 3 months presents a PET-scan that reveals a hypermetabolic lesion in the surgical field at the level of the larynx with supraclavicular lymph nodes, existence of metabolic activity in the mesothoracic pilar lymph nodes and pulmonary metastases, bone lesions with osteolysis in the left pelvic bone, all indicative of metastatic actively metabolic disease.
Radiation to the pelvis was planned and chemotherapy with cisplatin + paclitaxel was started, where after 6 cycles with stable disease there was a change to next line treatment with nivolumab. The patient showed satisfactory clinical improvement, complete remission of the pathological lesions in the larynx and continued for 10 months before the progression of the disease with new nodular peritoneal lesions and increase in pulmonary nodules.
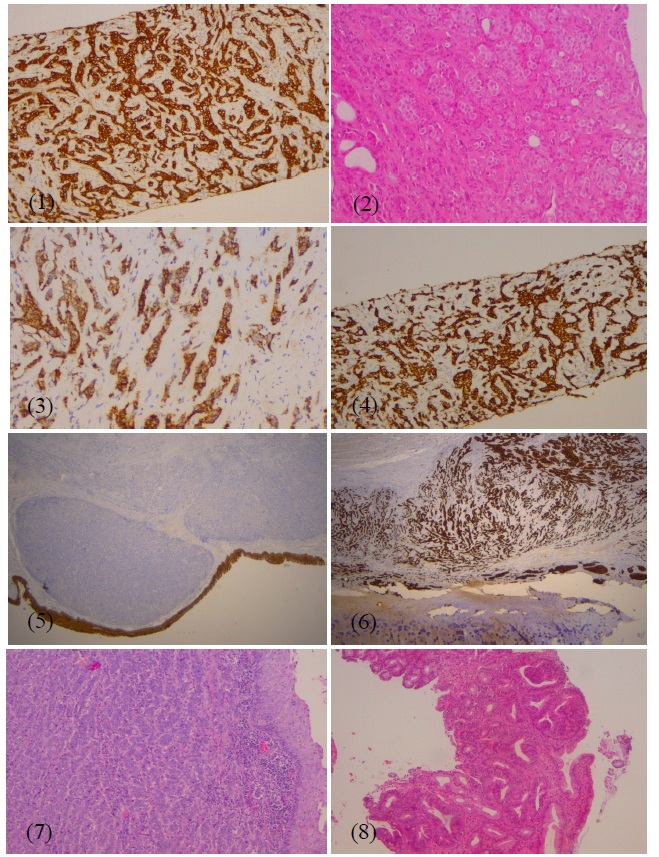
This was followed by the next line of treatment with cisplatin + 5-Fluorouracil where after 3 cycles he had an improvement but the benefit was not maintained, as in the 6 cycles it had a mixed response with an increase in pulmonary foci and lymph nodes in the mediastinum, but a decrease in lateral abdominal nodules. It is noteworthy that in the area of the cervix no pathological area was depicted, neither in the context of recurrence nor lymph nodes. Due to the overall deterioration in the clinical picture, it was deemed necessary to change the treatment with the addition of immunotherapy-pembrolizumab- together with cisplatin. This combination was well tolerated for 4 months before the further aggravation of the disease with an increase in nodules in the abdominal muscles and the appearance of new ones in the soft tissues of the abdomen, resulting in the start of the next line of treatment with paclitaxel + cetuximab on a weekly basis. After 5 months of treatment the patient shows worsening of the overall pain with new lesions in the soft tissues, of which left paraspinal, where a new biopsy was performed. The finding described moderate carcinoma with incomplete glandular formations and individual epithelial characters. Positive staining in CKAE1 / AE3, CK7, TTF-1, Heppar-1 and less in EMA. The conclusion leads to adenocarcinoma with hepatocellular differentiation with the most probable cause being the recurrence of the known laryngeal or gastric adenocarcinoma. The reason we were led to a new biopsy was the fact that there was no disease in the cervix, only metastatic foci, something that generally does not follow the natural course of head and neck metastatic disease.
Indeed, a gastroscopy was performed where 3 ulcers were found in the esophagus and in the dome of the stomach with sites of low-grade dysplasia and focal throughout the lesion high-grade dysplasia, grade III / IV based on the revised Vienna classification. The possibility of malignancy in an adjacent position was possible, but due to the patient's difficulty in repeating gastroscopy, but also the exhaustion of basic treatment options in combination with the rapid clinical deterioration, it was decided to administer irinotecan every 14 days. At the end of 4 doses of treatment, the patient showed significant clinical improvement and reduction in the size of the paravertebral mass where the new biopsy was performed. The performance status in combination with the findings of the clinical examination confirmed the correctness of our choice and the patient continued the same treatment. Unfortunately, he was hospitalized before the scheduled staging test at our hospital due to an ischemic stroke from which he died after a total of 2 months of irinotecan treatment.
Discussion
Laryngeal cancer is a part of group of head and neck cancer.
Depending on the location is divided into three different subgroups:
• Supraglottis: 35% of laryngeal cancer
• Glottis: More than half of laryngeal cancer cases (60%)
• Subglottis: About 5% of the cases
The most common histologic type of laryngeal cancer is squamus cell carcinoma (about 95 % of cases) followed by synovial sarcoma, chondrosarcoma, adenoid cystic carcinoma and adenocarcinoma which is our case report and not otherwise specified.
The most common presented symptoms to patients with laryngeal cancer are hoarseness, cough , difficulty with breathing, dysphagia, throat pain and neck swelling.
Adenocarcinoma of larynx is a rare type of laryngeal adenocarcinoma (6%-8% of laryngeal cancer cases) with poor prognosis. These lesions show specific histopathologic patterns of the other savilary gland tumor types and can occur in both parotid and minor savilary glands and typically are presented in sixth to eighth decades of life. Pathologic analysis can show tubular, papillary patterns. It is important that adenocarcinoma from another part of body to be excluded since savilary gland adenocarcinoma can mimic adenocarcinoma from other organs [4,5]. Like in our case, we did not find any other side, that could be the side of origin and as we mentioned before the absence of any tumor in the neck area made the origin of a salivary gland tumor the least possible.
Hepatoid adenocarcinoma is an extremely rare type of extrahepatic adenocarcinoma with morphologic similarities of hepatocellural carcinoma. These two type of cancer cannot be differentiated of the morphological pattern alone. Immunochemistry stains positive for alpha-fetoprotein, CK8, CK18, and the membranous, canalicular staining for polyclonal carcinoembryonic antigen underline its hepatoid nature . On the contrary, positivity for CK19 and CK20 and negative stains for HepPar1 in tumors and are distinctive features of HAC. The negative stain for CK 7 differentiates it from hepatocellular cholangiocarcinoma [6]. In our case the most important site to examine was the gastrointestinal system.
Tumor cells show a centrally located nucleus and abundant, eosinophilic cytoplasm, resembling hepatocellular carcinoma cells. This rare type of adenocarcinoma is most commonly found in the stomach (63%), followed by the ovary (10%), gallbladder, pancreas and endometrium while only 22 cases have been reported in the literature, with pulmonary localization (7). Like in our patient the findings of high grade dysplasia could include tumor cells if another gastroscopy had been performed.
References
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020 CA Cancer J Clin. 2020; 70: 7-30
- Rodel RM, Steiner W, Muller RM, et al. Endoscopic laser surgery of early glottic cancer: involvement of the anterior commissure. Head Neck. 200; 31: 583-592.
- Zouhair A, Azria D, Coucke P, et al. Decreased local control following radiation therapy alone ine early stage glottic carcinoma with anterior commissure extension. Strahlenther Onkol 2004; 180: 84-90.
- Luo YT, Gou X, Jiang XJ. [Primary mucinous adenocarcinoma of the larynx: a case report]. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2019; 33: 80-81.
- Spinazzi EF, Abboud MT, Dubal PM, Verma SP, Park RC, et al. Laryngeal adenocarcinoma not otherwise specified: A populationbased perspective. Laryngoscope. 2017; 127: 424-429.
- Terracciano LM, Glatz K, Mhawech P, Vasei M, Lehmann FS. et al. Hepatoid Adenocarcinoma With Liver Metastasis Mimicking Hepatocellular Carcinoma. The American Journal of Surgical Pathology. 2003; 27: 1302–1312.
- Roberts CC, Colby TV, Batts KP. Carcinoma of the Stomach With Hepatocyte Differentiation (Hepatoid Adenocarcinoma). Mayo Clinic Proceedings. 1997; 72: 1154–1160.