
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Fatal attraction: A case of multiple magnet ingestion in an infant
Neehar Patil1; Abhishek Chaturvedi2; Padmalatha S Kadamba3; Jeevak Shetty1; Manjiri Somashekhar1*
1 Assistant Professor, Department of Paediatric Surgery, Ramaiah Medical College and Hospital, Bangalore, India.
2 Postgraduate, Department of General Surgery, Ramaiah Medical College and Hospital, Bangalore, India.
3 Professor, Department of Paediatric Surgery, Ramaiah Medical College and Hospital, Bangalore, India.
*Corresponding Author: Manjiri Somashekhar
Associate Professor, Department of Paediatric
Surgery, Ramaiah Medical College and Hospital,
Bangalore, 560054, India.
Email: manjiris@yahoo.com
Received : Sep 13, 2021
Accepted : Oct 18, 2021
Published : Oct 25, 2021
Archived : www.jcimcr.org
Copyright : © Somashekhar M (2021).
Abstract
Background: Foreign body ingestion is common amongst young children, and they tend to pass spontaneously in most. Multiple magnet ingestion, though not very common, requires early intervention to avoid serious complications.
Case presentation: A 1 year old infant was brought to us with symptoms of bilious vomiting and abdominal pain. A plain abdominal x ray revealed presence of multiple radio opaque foreign bodies adherent to each other, lying in the small bowel. This raised the suspicion of accidental ingestion of multiple magnets, which was confirmed on detailed interrogation of the parents. An exploratory laparotomy revealed volvulus with pressure necrosis causing multiple perforations of the small bowel, for which a bowel resection with anastomosis and a loop ileostomy was performed, also all the magnetic beads were removed intact. The stoma was reversed after 4 weeks. At follow up the child has grown well with no residual complaints.
Conclusion: The importance of early detection and intervention in a case of multiple magnet ingestion in children should be emphasised amongst the parents of young children. Spread of awareness by the primary paediatricians would help in reducing the morbidity and mortality.
Keywords: multiple magnets; intestinal obstruction; perforation.
Citation: Patil N, Chaturvedi A, Kadamba PS, Shetty J, Somashekhar M. Fatal attraction: A case of multiple magnet ingestion in an infant. J Clin Images Med Case Rep. 2021; 2(5): 1379.
Introduction
Foreign body ingestion is common amongst children, and less than 1% of them require surgical interventions [1]. Multiple magnet ingestion in children, may cause serious complications and must be recognized early by paediatricians. Neodymium magnets are more powerful than traditional ferrite magnets and if ingested, cause serious complications in children [2]. We detail the presentation and management of a 1-year-old infant, with ingestion of multiple neodymium magnets and propose a simple algorithm for management of similar cases in our daily practice.
Case presentation
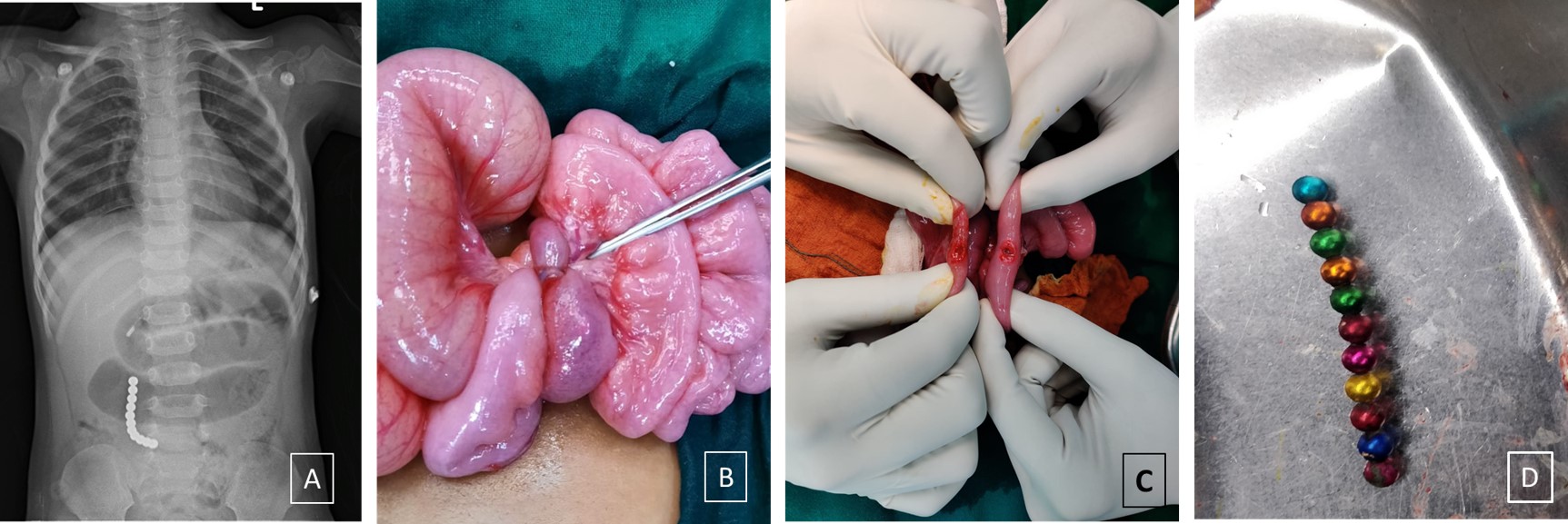
A 1-year-old infant was brought to the emergency department with 8-10 episodes of bilious vomiting and upper abdominal discomfort for 48 hours. Child had not passed stools for 2 days. No other significant history was obtained from the parents. Child was developmentally normal as per age, with vital signs within normal limits. On examination of the abdomen, mild tenderness was noted over the epigastric and right hypochondrium. The blood investigations were reported to be normal without any indication of a bowel infection. A routine radiograph of the abdomen revealed, 11 radio opaque spherical bodies (neodymium magnets) arranged in a linear fashion with dilated small bowel loops, with no signs of free air in the abdomen (Figure 1a). On retrospective interrogation the parents revealed the history of consumption of small magnets by the infant, which was used for playing by the elder sibling.
The infant was prepared for an exploratory laparotomy in view of features suggestive of an intestinal obstruction, after obtaining consent from the parents. Intraoperatively, the proximal small bowel (jejunum and proximal ileum) appeared to be dilated, with 8 magnets (4 in each loop) adherent to adjacent bowel loops causing congestion secondary to a volvulus, due to entrapment of the bowel by the magnets (Figure 1b). The magnets appeared to be strongly adherent to each other, after the bowel involved was separated from each other two perforations were noted, i.e., 7 cm and 30 cm proximal to the ileo cecal junction (Figure 1c). Only 8 magnets were extracted out, when an on-table fluoroscopy was performed the remaining 3 magnets were found in the 1st part of duodenum which were carefully milked out through the first perforation in the small bowel. The proximal perforation in the ileum was large, with extensive serosal tear which warranted resection and anastomosis, while the distal perforation was converted into a loop ileostomy due to its proximity to the ileocecal junction. A repeat fluoroscopy was performed on table to check for any residual magnets. All the 11 magnets were extracted out (Figure 1d).
The post-operative period was uneventful, oral feeds were started on post-operative day 3 which was progressed to full feeds by day 6. The infant was discharged from the hospital on post-operative day 7. The stoma reversal was performed 3 weeks later, which was also uneventful. The child at follow up has grown well with no residual abdominal complaints.
Discussion
Foreign body ingestion is a common paediatric problem; with majority been reported in those who are younger than 3 years of age [3]. Most foreign bodies ingested, pass out without any complications, however a history of possible magnet ingestion should be treated with more caution, especially amongst children. Traditional ferrite magnets are large and magnetically weak, and the earliest case report of bowel perforation following the ingestion of these ferrite magnet was from Japan in 1995 [4]. However, the new neodymium iron boron magnets have become smaller, stronger, more prevalent, causing severe damage to the gastrointestinal tract. Neodymium iron boron magnets are 10-20 times stronger than traditional ferrite magnets. Neodymium magnets were invented by General Motors and Sumitomo Special Metals in 1982, and are used in many toys and modern household products [2]. In 2002 , McCormick et al reported 24 cases of neodymium magnets ingestion causing gastro intestinal complications [5]. Complications tend to occur when these magnets after ingestion attract different bowel loops, trapping them causing ischemia secondary to pressure necrosis leading to bowel necrosis, volvulus, perforation and sepsis [6,7]. This could have serious lifelong consequences, including bowel resections and thereby increasing the morbidity especially amongst children [8]. In 2006, the US Consumer Product Safety Commission raised the recommended age for magnetic children’s toys from 3 years to 6 years due to increased incidence of ingestion of these magnets and to ensure children’s safety [9,10]. In a 2012 survey, members of the North American Society for Paediatric Gastroenterology, Hepatology and Nutrition reported 480 cases of high-powered magnet ingestions in the previous 10 years, 204 of which were in the previous 12 months [11]. We at our institute have observed a similar trend of increase in the prevalence of such cases amongst children, and we feel that a ban on the sale of such type of toys may help in preventing future incidence of such cases.
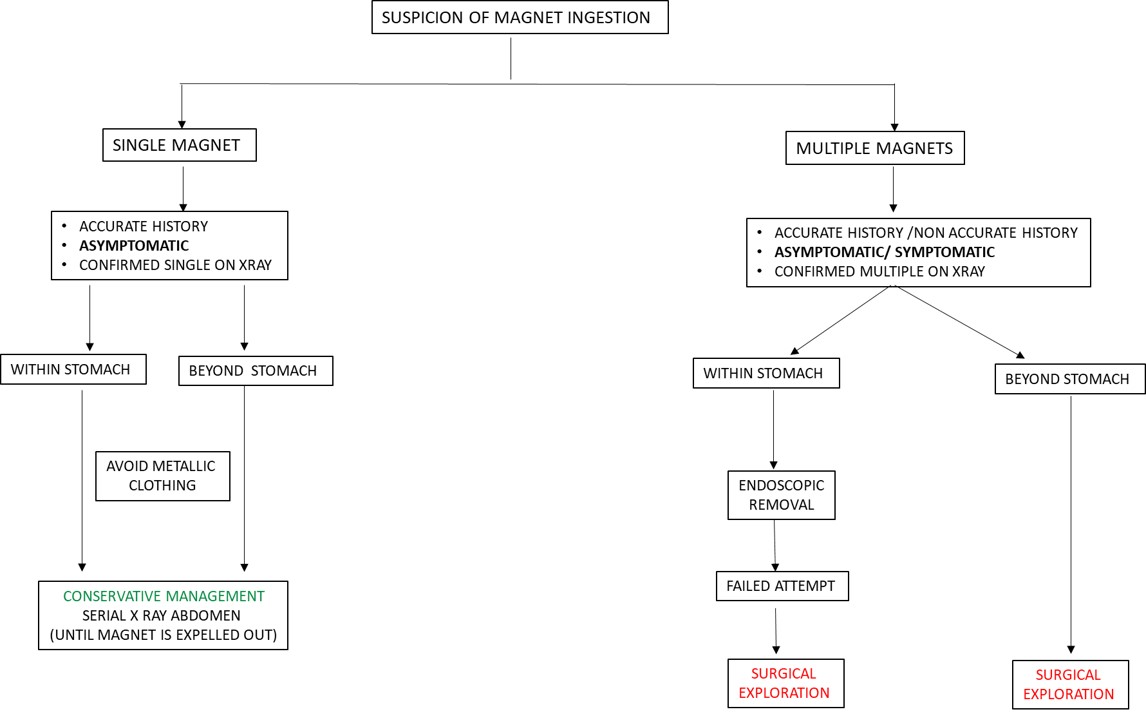
Children usually present with symptoms such as vomiting, abdominal pain, and fever following ingestion of a foreign body [12]. The difficulty to obtain a precise history of magnet ingestion, which is common amongst the paediatric population, can lead to substantial delays in diagnosis and management. In our case the parents did not reveal any history of magnet ingestion initially, only on detecting a foreign body on imaging, the parents retrospectively revealed a history of multiple magnet ingestion. There are many guidelines and algorithms proposed in literature for the management of children with magnet ingestions, to avoid delay in their diagnosis and management especially by primary health care individuals [1,2,13]. We too have formulated an algorithm for the management of such cases of magnet ingestion which is simple, detailed, and self-explanatory (Figure 2). An accurate history, clinical features and an appropriate imaging are the most important, in the management of such children who have ingested magnets, be it single or multiple. If ingestion of a single magnet is suspected (either in stomach or beyond the stomach), then the child may be followed by serial imaging until the magnet is expelled out. Hypothetically, a single magnet especially the neodymium magnets may be attracted to other metallic objects which are either swallowed or in contact with the anterior abdominal wall. Thus, the parents are counselled to avoid clothing with metallic buttons or buckles for the children. If ingestion of multiple magnets is suspected (either in the stomach or beyond the stomach), then the management is more complicated. If the child is symptomatic or asymptomatic and on serial imaging the magnets appear to be bound together, it can be inferred that they are anchoring to each other through the bowel wall, and a perforation is likely to occur. If in the stomach, a trial with endoscopy or a catheter with magnetic tip for retrieving the magnet can be attempted, but if failed the child would require surgical intervention [14,15]. If passed distal to pylorus, prompt surgical intervention is required before a complication develops. In our case as the infant was symptomatic with abdominal pain and vomiting with the magnets been multiple, we considered surgical exploration to avoid further complications. If early intervention is considered extensive bowel resections due to bowel necrosis and dangers of sepsis can be avoided.
Conclusion
Primary prevention is the best way to avoid morbidity associated with multiple magnet ingestion in children, and warning labels on magnet-based products have been insufficient in avoiding such cases scenarios. This case illustrates the dangers of multiple neodymium magnet ingestion, and the need for an early surgical intervention based on a simple management algorithm to prevent morbidity.
Declarations
Ethics approval and consent to participate: Since the patient concerned is a child, written informed consent was obtained from the parent.
Consent for publication: Written informed consent was obtained from the parent for publication of this case report and accompanying images.
Availability of data and material: Available on request.
Competing interests: The authors declare that they have no competing interests.
Authors’ contributions: Concepts: NP, AC. Design: NP. Definition of intellectual content: NP, MS. Literature search: PSK, JS. Data acquisition: NP, AC: Manuscript preparation: NP, AC and MS. Manuscript editing: MS. Manuscript review: NP, PSK and MS. Guarantor: MS. It is also declared that all authors have read and approved the manuscript.
References
- Butterworth J, Feltis B. Toy magnet ingestion in children: revising the algorithm. J Pediatr Surg. 2007; 42: e3–e5.
- Hussain SZ, Bousvaros A, Gilger M, Mamula P, Gupta S, Kramer R, et al. Management of ingested magnets in children. J Pediatr Gastroenterol Nutr. 2012; 55: 239–242.
- Kay M, Wyllie R. Pediatric foreign bodies and their management. Curr Gastroenterol Rep. 2005; 7: 212–218.
- Honzumi M, Shigemori C, Ito H, Mohri Y, Urata H, Yamamoto T. An intestinal fistula in a 3-year-old child caused by the ingestion of magnets: Report of a case. Surg Today. 1995; 25: 552–553.
- McCormick S, Brennan P, Yassa J, Shawis R. Children and minimagnets: an almost fatal attraction. Emerg Med J. 2002; 19: 71–73.
- Dutta S, Barzin A. Multiple magnet ingestion as a source of severe gastrointestinal complications requiring surgical intervention. Arch Pediatr Adolesc Med. 2008; 162: 123–125.
- Haraguchi M, Matsuo S, Tokail H, Azuma T, Yamaguchi S, Dateki S, et al. Surgical intervention for the ingestion of multiple magnets by children. J Clin Gastroenterol. 2004; 38: 915–916.
- Oestreich AE. Danger of multiple magnets beyond the stomach in children. J Natl Med Assoc. 2006; 98: 277.
- Commission UCPS. Serious injuries prompt recall of Mattel’s Polly Pocket magnetic play sets. Release. 2012.
- İlçe Z, Samsum H, Mammadov E, Celayir S. Intestinal volvulus and perforation caused by multiple magnet ingestion: report of a case. Surg Today. 2007; 37: 50–52.
- Li BU, Lefevre F, Chelimsky GG, Boles RG, Nelson SP, Lewis DW, et al. North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition consensus statement on the diagnosis and management of cyclic vomiting syndrome. J Pediatr Gastroenterol Nutr. 2008; 47: 379–393.
- Miller RS, Willging JP, Rutter MJ, Rookkapan K. Chronic esophageal foreign bodies in pediatric patients: A retrospective review. Int J Pediatr Otorhinolaryngol. 2004; 68: 265–272.
- Vijaysadan V, Perez M, Kuo D. Revisiting swallowed troubles: Intestinal complications caused by two magnets - A case report, review and proposed revision to the algorithm for the management of foreign body ingestion. J Am Board Fam Med. 2006; 19: 511–516.
- Hachimi-Idrissi S, Corne L, Vandenplas Y. Management of ingested foreign bodies in childhood: our experience and review of the literature. Eur J Emerg Med Off J Eur Soc Emerg Med. 1998; 5: 319–323.
- Suita S, Ohgami H, Yakabe S, Nagasaki A. The fate of swallowed button batteries in children. Z Für Kinderchir. 1990; 45: 212–214.