
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Superior mesenteric artery syndrome causing gastric outlet obstruction: A myth in acute abdomen
Norfaidhi Akram MN1; S Husni2; Sarmukh S2*; Azmi H2
1 International Islamic University Malaysia, Malaysia.
2 Hospital Sultan Haji Ahmad Shah, Temerloh, Malaysia.
*Corresponding Author: Sarmukh Singh
Hospital Sultan Haji Ahmad Shah, Temerloh, Malaysia.
Email: sarmukh_rao@yahoo.com
Received : Sep 14, 2021
Accepted : Oct 19, 2021
Published : Oct 26, 2021
Archived : www.jcimcr.org
Copyright : © Sarmukh S (2021).
Abstract
Objective: We aim to report a case of gastric outlet obstruction in adolescence that was diagnosed as a superior mesenteric artery syndrome and treated successfully by gastrojejunostomy.
Case report: A 17-year-old female presented to emergency department with acute abdomen. She was also complaint of significant weight loss past 2 months. On clinical examination she was underweight with fullness of upper abdomen down to umbilicus. Oesophagogastroduodenoscopy (OGDS) was performed showed grossly dilated stomach with unable to go beyond D3 region. Contrast Enhanced Computed Tomography (CECT) abdomen suggestive of Superior Mesentery Artery (SMA) syndrome. She was subjected to gastrojejunostomy and recovered well postoperatively.
Conclusion: An acute onset of gastric outlet obstruction in adolescence can be a diagnostic and treatment challenging. Our case patient was diagnosed as a SMA syndrome based on the history taking and CT findings. We would like to advocate a high index of suspicious SMA syndrome should be included in an acute abdomen in adolescence besides volvulus and malrotation. The treatment options should be individualized. In this case we opted for a gastrojejunostomy compared to duodenojejunostomy. The decision was made based on the patient nutritional status as patient was low Body Mass Index (BMI) was 16 kg/m2 which carries a high risk of anastomotic leak.
Keywords: superior mesenteric artery syndrome; cast syndrome; wilkie’s syndrome; arteriomesenteric duodenal compression; duodenal vascular compression.
Citation: Akram MN, S Husni, Sarmukh S, Azmi H. Superior mesenteric artery syndrome causing gastric outlet obstruction: A myth in acute abdomen. J Clin Images Med Case Rep. 2021; 2(5): 1383.
Introduction
Superior mesenteric artery syndrome is a rare entity of chronic duodenal obstruction, caused by compression of the third part of the duodenum between the superior mesenteric artery and the aorta with the prevalence less than 0.3% [1]. High index suspicious of the disease must be made due to difficulty in diagnosis clinically. We describe the rare case of superior mesentery artery syndrome managed in district hospital in Malaysia.
Case report
A 17-year-old lady presented to emergency department with acute onset colicky generalized abdominal pain for 2 days. She had vomited more than 5 times for 2 days prior to presentation on which was fluid content. She had an episode of loose stool after taking outside food last 2 days. Further questioning she informed that the weight reducing past 2 months was 5 kg (49 kg to 44 kg). Otherwise, able to take orally well, no early satiety, no altered bowel habit, no prolonged cough episodes. Her father diagnosed to has lung cancer at the age of 40 years old. Other than that, no past medical, psychiatric nor surgical history.
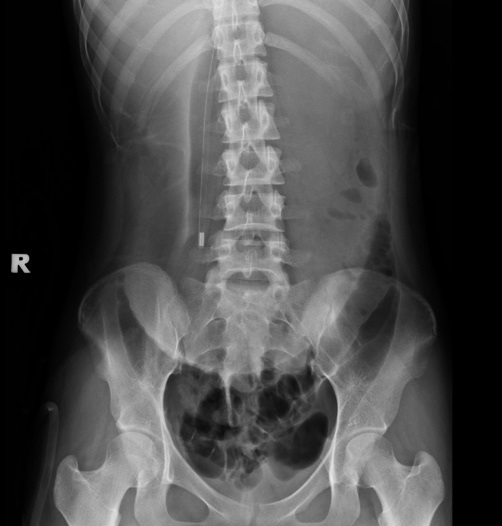
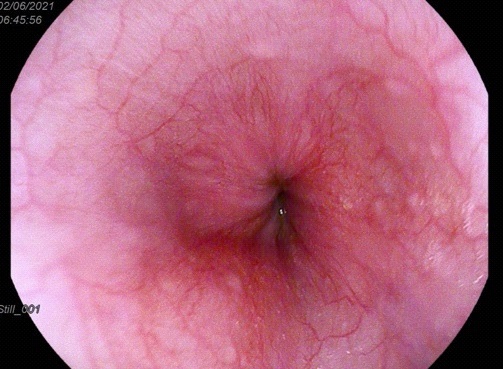
General examination showed patient was cachexic (BMI was 16 kg/m2 ) and dehydrated. On abdominal examination there was fullness from upper abdomen down to umbilicus region, but no tenderness elicited. Succussion splash was positive. Systemic reviews were unremarkable. Laboratory investigation showed leukocytosis. Other blood parameter and electrolytes were within normal range. Abdominal x-ray showed large gastric pushing the transverse colon to the pelvis region (Figure 1). We resuscitated the patient with crystalloids and a Ryle’s tube was inserted showed about 3 liters of gastric contain. Our provisional diagnosis was gastric volvulus and malrotation. An Oesophagogastroduodenoscopy (OGDS) was performed showed grossly dilated stomach with normal mucosa lining. Unable to go beyond D3 region (Figure 2). We proceeded with CECT abdomen showed a narrow aortomesenteric angle concerning for superior mesenteric artery syndrome with reduced aortomesenteric distance and aortomesenteric angle measuring 4.4mm and 15 degree respectively (Figure 3 & 4). A diagnosis of superior mesenteric artery syndrome was made. Patient was started on parenteral nutritional support with total calorie requirement of 12 kcal/kg/day. However, after 7 days patient abdomen was distended, and the abdomen pain was persisted. We proceeded with exploratory laparotomy and retro-colic gastrojejunostomy. Post operatively patient had speedy recovered and was discharged home.


Discussion
Superior Mesentery Artery (SMA) syndrome is a rare benign causes of small bowel obstruction. In this syndrome, the third part of the duodenum will be compressed between the superior mesenteric artery from which it is originated and the abdominal aorta. The reduction in angulation results in partial or complete obstruction. Normal aorta-superior mesenteric artery angle ranges from 38 to 65 degree and aortomesenteric distance 10 to 28 mm. In SMA syndrome, both the angle and distance between two structures reduced [1-4].
Etiologies of the SMA syndrome can be congenital or acquired anatomical abnormalities [5]. Congenital etiologies include abnormal insertion of SMA or high insertion of the angle to Treitz dislocating the duodenum to cranial position. Acquired anatomic abnormalities can occur following corrective spinal surgery, and after abdominal surgery. Severe wight loss leading the depletion of the fatty cushion around the SMA in a major cause of SMA syndrome. Catabolic states like burns, eating disorders, or wasting conditions such as neoplastic diseases and malabsorption are most reported reasons of drastic weight loss.
Patient with SMA syndrome may present with acute or chronic symptoms. Acute presentation usually characterized by signs and symptoms of duodenal obstruction. Chronic cases may present with long standing vague abdominal symptoms or recurrent episodes of abdominal pain with vomiting. But in our patient, she presented with acute gastroenteritis like symptoms in which incidental finding of the SMA syndrome.
The diagnosis of SMA syndrome is challenging and often delayed due to its insidious presentation. High clinical suspicion is warranted, and diagnosis is based on clinical evidence supported by radiological findings. Barium follow-though study demonstrates dilatation of the first and second part of duodenum with or without gastric dilatation, anti-paristaltic flow of barium proximal to the obstruction and delay of 4-6 hours in gastroduodenojejunal transit time, with the relief of obstruction when the patient is placed on prone, knee-chest or left lateral position. Contrast enhanced CT or magnetic resonance imaging enable visualized the vascular compression of the duodenum and precise measurement of the aortomesenteric angle and distance [6]. Endoscopic examination may visualize pulsatile extrinsic compression.
Treatment for SMA syndrome can be divided into conservative medical treatment and surgical intervention. Conservative measure such as gastric decompression, parenteral nutrition post pyloric feeding. In some patient, posturing maneuvers during meal and motility agents may be helpful. High success rate up to 90% in surgical intervention of duodenojejunostomy. Strong’s procedure involves dissection of ligament of Treitz with mobilization caudally of the duodenum [5]. However, the success rate of the procedure as low as 75% [6]. Gastrojejunostomy is another method to relieve the obstruction but with increase of postoperative complications [6].
Conclusion
An acute onset of gastric outlet obstruction in adolescence can be a diagnostic and treatment challenging. Our case patient was diagnosed as a SMA syndrome based on the history taking and CT findings. We would like to advocate a high index of suspicious SMA syndrome should be included in an acute abdomen in adolescence besides volvulus and malrotation. The treatment options should be individualized. In this case we opted for a gastrojejunostomy compared to duodenojejunostomy. The decision was made based on the patient nutritional status as patient was low BMI was 16 kg/m2 which carries a high risk of anastomotic leak.
References
- Mathenge N. et al. Superior mesenteric artery syndrome and its associated gastrointestinal implications. Clin. Anat. 2014; 27: 1244–1252.
- Welsch T, Büchler MW, Kienle P. Recalling superior mesenteric artery syndrome. Dig. Surg. 2007; 24: 149–156.
- Merrett ND, Wilson RB, Cosman P, Biankin AV. Superior mesenteric artery syndrome: Diagnosis and treatment strategies. J. Gastrointest. Surg. 2009; 13: 287–292.
- Mandarry MT, Zhao L, Zhang C, Wei ZQ. A comprehensive review of superior mesenteric artery syndrome. Eur. Surg. Acta Chir. Austriaca. 2010; 42: 229–236.
- Ganss A, Rampado S, Savarino E, Bardini R. Superior Mesenteric Artery Syndrome: a Prospective Study in a Single Institution. J. Gastrointest. Surg. 2019; 23: 997–1005.
- Lee TH et al. Superior Mesenteric Artery Syndrome: Where Do We Stand Today? J. Gastrointest. Surg. 2012; 16: 2203–2211.