
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Rhodococcus in foal, from diagnosis to treatment: Case report
Suellen Cristina Guedes da Luz1*; Márcio Augusto Ferreira1; Juliana Weckx Peña Muñoz4; André Rinaldi Fukushima2,3,4
1 São Judas Tadeu University (USJT), Mooca, SP Brazil.
2 Departamento de Patologia, Faculdade de Medicina Veterinária e Zootecnia, Universidade de São Paulo, São Paulo/SP,Brasil
3 School of Health Sciences IGESP, Rua da Consolação, 1025, 01301-000, São Paulo, Brazil.
4 Centro Universitário das Américas FAM - São Paulo, Brazil.
*Corresponding Author: Suellen Cristina
Guedes da Luz
São Judas Tadeu University (USJT). Mooca, SP
Brazil.
Email: su-guedes@uol.com.br
Received : Sep 13, 2021
Accepted : Oct 19, 2021
Published : Oct 26, 2021
Archived : www.jcimcr.org
Copyright : © Guedes SC (2021).
Abstract
The present work reports a case of a foal affected by Rhodococcus equi, an optional intracellular gram-positive pleomorphic cocobacillus, which, when eliminated with the feces of infected animals, in the soil becomes a potential pathogen, capable of causing mainly piogranulomatous bronchopneumonia. The animal, a 23-day-old Brazilian equestrian foal, was sent to the veterinary hospital with hyperthermia, increased heart and respiratory rates, crackle in tracheal auscultation, loss of appetite and prostration. After hematological, ultrasound, radiographic examinations, and collection of tracheal lavages for culture and PCR, the definitive diagnosis of rhodococcosis was obtained, which is a bacterial disease that mainly affects foals, has a worldwide distribution and has a great economic impact on equine culture. Based on the results, treatment with azithromycin, rifampin, flunixin meglumine, sucralfate, ranitidine hydrochloride and amoxicillin with clavulanate was instituted, associated with nebulization with acetylcysteine diluted to 0.9% sodium hydrochloride solution. After a few weeks, there was no evolution in the results of the ultrasound and radiographic exams, however the hematological exams were within the reference levels, there was a significant clinical improvement, and the animal was discharged. It is noteworthy that early diagnosis was essential for the effectiveness of treatment and remission of clinical signs.
Keywords: rhodococcosis; foals; rhodococcus equi.
Citation: Guedes SC, Ferreira MA, Muñoz JWP, Fukushima AR. Rhodococcus in foal, from diagnosis to treatment: Case report. J Clin Images Med Case Rep. 2021; 2(5): 1384.
Introduction
Caused by the bacterium Rhodococcus equi, rhodococcosis is considered a zoonosis and its main manifestation is pyogranulomatous pneumonia, which is difficult to treat and results in high mortality rates in foals. This agent is an opportunistic and facultative intracellular microorganism, it multiplies in the soil, mainly in large farms of production animals [9,15].
It is a disease that mainly affects horses and, in addition to pulmonary infections, less frequently enteric and joint manifestations occur. In foals, morbidity is variable, reaching 30% or more of the animals, since its mortality is high, with 50% or more of the animals infected, especially in cases where the diagnosis is late or when the therapy is inadequate. With worldwide distribution, R. equi is considered the infectious agent that causes the greatest damage in the rearing of foals, as it mainly affects animals between two weeks and six months of age, a period in which there is a decline in passive immunity acquired through colostrum associated with the immaturity of the animal’s immune system at the cellular response level. It is a rare disease in adult horses, which when affected manifest mainly respiratory and enteric affections in them, rhodococcosis is associated with immunosuppressive diseases, such as equine herpesvirus, being secondary to them [20,4,12,5,15,21].
Sick animals and reservoirs are a source of infection, as they eliminate the agent with feces, but foals are considered the main disseminators and responsible for maintaining the bacteria in the properties, eliminating virulent strains that are associated with the type of protein that the plasmid produces, the that makes the microorganism virulent or not. In addition to feces, the agent can be eliminated by respiratory secretions of other herbivores and omnivores and can remain viable in the facilities, in the soil for up to twelve months, as it is a very resistant agent to adverse environmental conditions, excess organic matter and dry climate environments favor the formation of contaminated aerosols. The agent can be transmitted through the respiratory route, orally, contaminating water and food, and because of the habit of coprophagy that foals may have, ingesting contaminated feces [20,4,1,21].
The disease has a silent onset, with incubation for several weeks, where the first signs to manifest are hyporexia, hyperthermia (41°C), lethargy and reduced feedings. The progression of the case can lead to weight loss and coughing (productive or not), as nasal secretions are not common, but when they occur, they present a purulent aspect. The most evident clinical manifestation of the disease is pneumonia and with the development of the disease, the animals start to present anorexia, recumbency, exercise intolerance, abdominal breathing, tachycardia, and cyanosis. Among the enteric signs are diarrhea, dehydration, weight loss, and growth retardation caused by ulcerative colitis and mesenteric lymphadenitis. Arthritis and synovitis can often occur due to deposition of immune complexes, especially in the tibiotarsal joints, but their signs are not clinically significant. In 10% of severely affected foals, immune-mediated uveitis may occur [14,4,16].
The early diagnosis of rhodococcosis is difficult due to its silent behavior associated with the capacity of foals to discreetly compensate for the progressive loss of respiratory function, and must be based on clinical and epidemiological findings, together with laboratory tests. Foals with rhodococcosis usually present leukocytosis by neutrophilia and increased levels of fibrinogen in the hematological analysis, but in some animals the changes are subtle, requiring the use of other diagnostic techniques such as ultrasonography and chest radiography, which reveal abnormalities in the lung parenchyma, among them, images that suggest abscesses. Another method to be used is the microbiological examination, which can be done from material obtained from tracheobronchial lavage, synovial fluid, blood and affected organs collected during necropsy. However, with greater specificity and sensitivity, we can use the PCR assay as a diagnostic tool, which identifies the DNA of the bacteria, the material for analysis is obtained from tracheal lavage, capable of identifying strains of R. equi. [14,15,21,18,8, 10,13,17,6].
After obtaining the definitive diagnosis, treatment should be instituted immediately due to the rapid progression of the disease, knowing that, in the 1980s there was a drastic reduction in mortality in foals due to the use of erythromycin associated with rifampicin, both of which are bacteriostatic that have synergy. Over the years, variable absorption of erythromycin when administered orally to foals and the appearance of side effects, including diarrhea and hyperthermia, have been observed. In view of this fact, azithromycin or clarithromycin is used as an alternative to it, which are more stable drugs, with greater bioavailability when administered orally, which allows reaching higher concentrations in cells and tissues. In foals with hyperthermia, lethargy and anorexia, therapy with non-steroidal antiinflammatory drugs should be performed. On the other hand, nebulization must be performed with care, as it can stress the animal and not have the desired effect, but oxygen therapy is indicated in animals with respiratory distress [7,5,19,11,2].
Therapy should be continued until complete remission of clinical signs and when its physical, radiological and laboratory parameters are within reference values. Decreased plasma fibrinogen levels, positive clinical response, and improvement in pulmonary conditions within seven days suggest a favorable prognosis. The growth of resistant strains, development of resistance during treatment, discontinuation of therapy and the difficulty that some antimicrobials must penetrate intracellularly or into the pyogranulomatous focus are facts that limit the treatment of rhodococcosis [14,15,7,5,1].
The control and prophylaxis of the disease are essential due to the difficulty in diagnosing and treating the disease. For this, some measures are needed, such as stimulating colostrum ingestion in the first hours of life of the foals, separating the animals into categories, adjusting the animal density in the same location and avoid accumulation of feces in pens and paddocks, as well as early identification of infected foals to start their treatment, thus preventing the spread of virulent strains [1].
This paper aims to report the occurrence of a case of rhodococcosis in a 23-day-old foal, treated at the Veterinary Hospital of the University of São Paulo, where he received clinical treatment indicated for the disease.
Case report
At the Veterinary Hospital of the Faculty of Veterinary Medicine and Animal Science of the University of São Paulo, in March 2020, a brown foal of the Brazilian Equestrian breed, with an estimated weight of 60 kg and 23 days of age, was treated. The main complaint was hyperthermia (42°C). During the anamnesis with the responsible veterinarian, he reported that on 02/03/2020 the animal was born without any changes, suckled colostrum, removed the meconium normally and the umbilicus was bandaged with 10% iodine, with no problems for your healing. The animal started to be more apathetic as of 02/22/20, reducing the frequency of feedings and tenesmus. On 02/26/20, when re-evaluating the foal, the veterinarian reported that the temperature had increased, reaching 42°C, the mucous membranes were congested, he had tenesmus and there was the presence of dry feces with blood in the rectal ampoule. It was then decided to institute treatment with fluid therapy with 7 liters of ringer with lactate, flunixin meglumine and dipyrone, soon after the animal was sent to the veterinary hospital. On physical examination, there was an increase in heart rate with 148 bpm, an increase in respiratory rate with 68rpm, temperature was 38.5°C and tracheal auscultation with crackle. The resident and the professor responsible for the case determined as a presumptive diagnosis an infection by Rhodococcus equi, responsible for causing rhodococcosis, then opted for hematological tests such as complete blood count, fibrinogen dosage, biochemistry, ultrasound and chest radiography and tracheal lavage for culture and PCR.
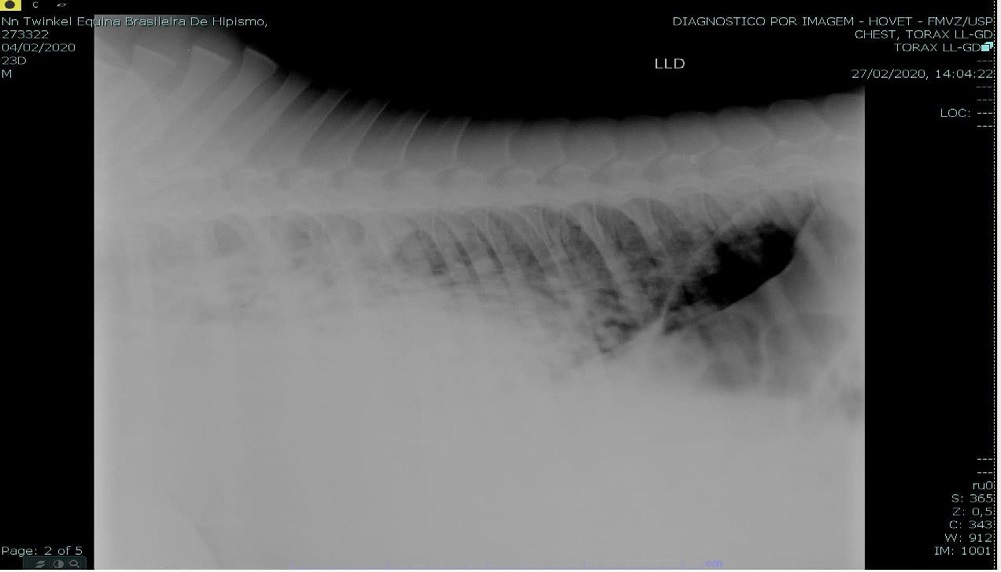
On chest ultrasound images, many anechogenic areas were observed in both hemithoraces, suggesting the presence of abscesses (cavitation areas). In the chest X-ray images performed on 02/27/2020, it was possible to observe lung fields with radiopaque images in the cranioventral region in greater quantity. Image suggestive of abscesses as shown in Figure 1.
The hematological tests were performed at small intervals for greater control, as the animal was not clinically stable, in graph 1 we can see the results of the animal’s erythrograms, with the reference values of each analysis being, red blood cells between 6.0 and 10.4 X 106 /uL, hemoglobin between 10.1 and 16.1 g/dL and hematocrit between 27 and 44%.
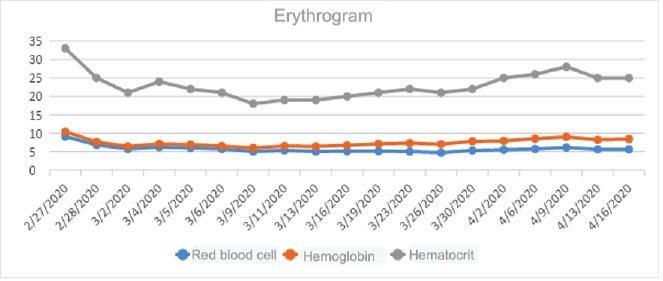
In the graph 1, we can see how the levels of red blood cell, hemoglobin and hematocrit were presented during the period of hospitalization of the animal, and the hemoglobin values were below the reference value throughout the period, the levels of red blood also remained below the reference values, however, close to it. When it comes to the hematocrit, it is possible to notice that, as well as the other erythrogram analyses, they were also below the reference levels, but its lowest value was on 03/09/2020, reaching 18%, at this time it was treatment with hyperimmune plasma bag was instituted, to stimulate the body to produce red cells and, from the results, it was possible to see that it had the desired effect, since the erythrogram levels were higher in the following days, even not reaching the value of reference at the time of the animal’s discharge.
In graph 2, it is possible to carry out the analysis of the animal’s white blood cell count throughout the period it was hospitalized, and its reference values are total leukocytes between 5600 and 12,100/uL, segmented neutrophils between 2900 and 8,500/uL, lymphocytes between 1,160 and 5,100/uL and monocytes between 0 and 700/uL.
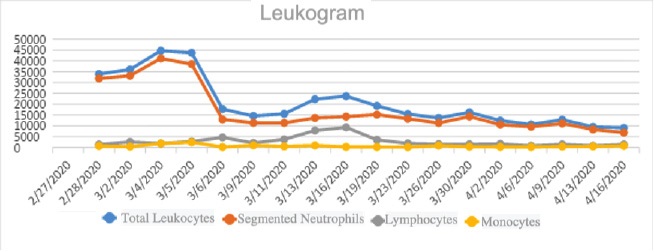
On the white blood cell count, we can see that the total leukocytes were much higher than the reference values until 04/02/2020 and, close to the animal’s discharge date, on 04/06/2020, the values stabilized within the reference. As for segmented neutrophils, they only entered the reference values on 04/13/2020, and it was maintained in the last exam, on 04/16/2020, the day the animal was discharged, before that, the values were always above the reference. Lymphocytes were as expected, and monocytes were reactive, and were sometimes identified as toxic monocytes, common in pneumonia. These results are consistent with the picture presented by the patient.
Graph 3 shows the serum biochemistry values. The reference values of each analysis are, albumin between 2.5 to 3.5 g/dL, AST 120 U/L, GGT between 4 and 44 U/L, total bilirubin between 0.9 and 2.9 mg/dL and direct bilirubin between 0.2 and 0.7 mg/dL, for the analysis of the renal profile, urea, which has a reference value between 30 and 40 mg/dL, and creatine, with values between 1.0 and 2.0 mg/dL, were evaluated. The results can be seen below.
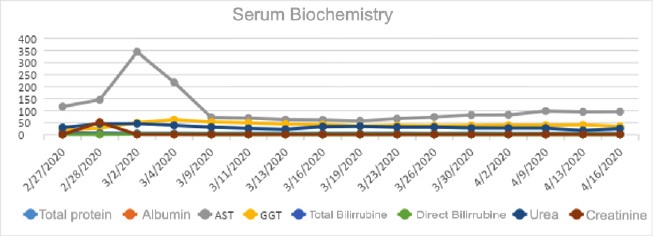
In the results of serum biochemistry, we can see that AST had a significant increase on 03/02/2020, as well as the levels of GGT and direct bilirubin were above the reference value, being normalized from 03/09/2020. Creatine and urea did not show important changes.
After performing the transtracheal wash and sending the collected material for the above-mentioned analyses, the result obtained from the PCR assay was positive for Rhodococcus equi and in the microbiological culture colonies of Escherichia coli, Escherichia fergusonii and Staphylococcus sciuri, which are gram bacteria, were isolated. negative and probably secondary to rhodococcosis.
Based on the results obtained in the exams performed, it was possible to reach a definitive diagnosis for rhodococcosis and immediately institute the treatment, which can be seen in table 1.
Table 1: Drugs used at the beginning of treatment.
Drug |
|
Dose (mg/kg) |
Volume |
Route of administration |
Frequency |
Azithromycin |
|
10 |
1 tube |
orally |
1 once a day |
Rifampicin |
|
10 |
1 tube |
orally |
2 times a day |
Flunixin meglumine |
|
1,1 |
1,3 ml |
intravenously |
1 once a day |
ranitidine hydrochloride |
|
2 |
2,5 ampoules |
intravenously |
3 times a day |
Metronidazole |
|
15 |
200 ml |
intravenously |
3 times a day |
sucralfate |
|
2000 |
1 ampoules |
orally |
4 times a day |
Amoxicillin with clavulanate |
|
15 |
2 pills |
orally |
2 times a day |
Source: author
In addition to the drugs used above, supplementation with a vitamin complex was performed and it was decided to perform nebulization with 3 ml of acetylcysteine diluted in 20 ml of 0.9% sodium chloride solution three times a day, as shown in figure 2, and soon after, respiratory physiotherapy was performed. During the procedure, the animal was not stressed to the point of hindering or preventing the treatment with nebulization, as well as physiotherapy, but had some episodes of bruxism, dry cough and little or no nasal secretion. During the days of hospitalization, the animal began to present respiratory rales, mainly in the cranial ventral region of the lungs, as well as difficulty breathing and wheezing. The animal also had episodes of diarrhea for three days, with fluctuations in its behavior, and in some moments, it behaved in an active way, standing up alone and looking for its mother to suckle, and in others it was apathetic and lying down for a long time.
With the progression of the treatment, the animal started to show clinical improvement, the respiratory changes stopped after approximately two weeks, it got up with the help of residents and trainees every two hours, but it had appetite and suckled in greater amounts compared to the beginning of your treatment. A few days later, the foal started to get up on its own, and went out twice a day to walk with its mother.
The treatment had the expected effect and even with a poor prognosis, the animal recovered clinically and was discharged on 04/16/2020, but the radiographic and ultrasound images of its lungs remained similar to the images at the time of diagnosis, the which was already expected by hospital professionals, since these signs take longer to show improvement, and in some cases, sequelae can be observed until the animal’s adult life.
For home treatment, rifampicin, azithromycin, and omeprazole were prescribed for 5 days. Probiotic in a single dose on 04/21/2020 and Pulmo-plus indefinitely. It was recommended to perform a complete blood count and fibrinogen on April 23, 2020, maintain oral supplementation according to the manufacturer’s recommendations and observe the frequency of feedings. Due to the administration of azithromycin, the animal could not be kept in the sun.
On 23/04/2020 the veterinarian responsible for the animal contacted the veterinary hospital to inform that the animal was clinically stable, and the results of the tests were within the expected levels.

Discussion
R. equi is considered an opportunistic microorganism, facultative intracellular, multiplying in the soil, mainly in rural environments with the creation of production animals. Horses are the main species affected and, in farms, the disease is endemic, where predisposing conditions for infection are observed, such as inadequate colostrum intake by foals, lack of hygiene and environmental health, excessive dust, proximity of facilities between different categories and age groups of animals, paddocks with high density of animals, dirty pastures, dry climate and high temperatures. The animal in question was with its mother in a stud farm, where the disease was not considered endemic, having as its main cause its age, its immune status, and the location of the property, which is in the state of São Paulo, as the occurrence of rhodococcosis is more frequent in southern and southeastern Brazil [8,3,4].
With the progression of the disease, the animal presented clinical signs already described by Radostits et al, (2007) [14], which highlights pneumonia as the main one, representing 60% or more of the cases, as well as anorexia, inappetence, exercise intolerance, abdominal breathing, tachycardia, corroborating the signs that the foal presented. Death occurs in 50% or more of cases diagnosed late, which did not occur with the animal in question, precisely because it instituted treatment and early diagnosis. The association of clinical and epidemiological findings, together with hematological, imaging and PCR tests are the basis for a definitive diagnosis, tools used by professionals at the veterinary hospital where he was hospitalized [14].
Bertone [4]. (2000) recommends for the treatment of rhodococcosis, the use of lipophilic antimicrobials, which have high intracellular concentrations, which corroborates the treatment established in this report, based on rifampcin and azithromycin, however, has the presence of purulent material as a limiting factor for the therapeutic action. in injuries caused by the disease [5].
Conclusion
Rhodococcosis is a disease with worldwide distribution, has a severe progression and a high mortality rate among foals. In this report, it was observed that early diagnosis and the institution of adequate treatment as described in the literature were essential factors for the remission of clinical signs, thus preventing the animal's death. As it affects mainly foals in their first weeks of life, it is the cause of great economic impact in equine culture.
References
- Barton MD, Hughes KL. Corynebacterium equi: A review. Veterinary Bullettin. 1980; 50: 65-80.
- Beech J, Sweeney CR. Infections caused by bacteria, mycoplasma, parasites and fungi. In: BEECH, J. Equine respiratory disorders. Philadelphia: Lea and Febiger. 1991; 181-207.
- Belotta AF. et al. Pneumonia por Rhodococcus equi em potra quarto de milha: diagnóstico radiográfico e ultrassonográfico. Veterinária e Zootecnia. 2015; 22 p.209-214, jun. 2015.
- Bertone JJ. Pneumonia e outros distúrbios associados ao Rhodococcus equi. In: REED, S.M.; BAYLY, W.M. Medicina Interna Eqüina. Rio de Janeiro: Guanabara Koogan. 2000; 830–839
- Giguère S, Prescott JF. Clinical manifestations, diagnosis, treatment, and prevention of Rhodococcus equi infections in foals. Veterinary Microbiology. 1997; 56: 313–334.
- Halbert ND. et al. Evaluation of a multiplex polymerase chain reaction assay for simultaneous detection of Rhodococcus equi and the vapA gene. American Journal of Veterinary Research. 2005; 66: 1380-1385.
- Hillidge CJ. Use of erythromycin-rifampin combination in treatment of Rhodococcus equi pneumonia. Veterinary Microbiology. 1987; 14: 337-342, 1987
- Leclere, M. et al. Comparison of the clinical, microbiological, radiological and haematological features of foals with pneumonia caused by Rhodococcus equi and other bacteria. Veterinary Journal. 2009; 187: 109-112, 2009.
- Linder R. Rhodococcus equi and Corynebacterium haemolyticum: two “Coryneform” bacteria increasingly recognized as agents of human infection. Emerging Infectious Diseases. 1997; 3: 1-10.
- Muscatello G. et al. Rhodococcus equi infection in foals: the science of ‘rattles’. Equine Veterinary Journal. 2007; 39: 470-478.
- Peiró JR. et al. Pneumonia em potros causada pelo Rhodococcus equi. Revista de Educação Continuada. 2002; 5: 73-86.
- Pronost S. et al. Rhodococcus équine: nouvelles approches et bilan de trois années d’études au laboratoire. Prat. Vét. Equine. 1998; 30: 57–65, 1998.
- Quinn PJ, Markey B, Carter ME, Donnelly WJ, Leonard FC. Microbiologia veterinária e doenças infecciosas. Artmed: Porto Alegre. 2005; 512.
- Radostits OM, Gay ME, Hinchcliff KW, Constable PD. Rhodococcus equi pneumonia in foals. In: radostits OM, GAY ME, Hinchcliff KW, Constable PD. Veterinary Medicine. A textbook of the disease of cattle, horses, sheep, pigs, goats and horses. WB Saunders, London. 2007; 800- 805.
- Ribeiro Mg.; Salerno, T.; Lara, G.H.B.; Siqueira, A.K.; Fernandes, M.C. Fatores de virulência de Rhodococcus equi. Implicações na epidemiologia e controle da rodococose nos animais e no homem. Veterinária e Zootecnia, v.14, n.2, p.147–163, 2007.
- Ribeiro MG, Nardi Júnior G, Dias Júnior JG, Paes AC, Megid J, et al. Polissinovite auto-imune por Rhodococcus equi em potro, secundária à enterocolite. Revista de Educação Continuada do CRMVSP. 2002; 5: 206–214.
- Sellon DC. et al. Comparasion of nucleic acid amplification serology and amplification serology and microbial culture for diagnosis of Rhodococcus equi pneumonia in foals. Journal of Clinical Microbiology. 2001; 39: 1289-1293.
- Slovis NM. What’s news. Journal of Equine Veterinary Science. 2004; 24: 369-370.
- Stratton-phelps M. et al. Risk of adverse effects in pneumonic foals treated with erythromycin versus other antibiotics: 143 cases (1986-1996). Journal of American Veterinary Medical Association. 2000; 217: 68-73.
- Takai S. Epidemiology of Rhodococcus equi infections: A review. Veterinary Microbiology. 1997; 56: 167– 176.
- Vargas AC. Infecções por Rhodococcus equi. In: Riet–Correa F, Schild AL, Mendez AMC, Lemos RAA. Doenças de Ruminantes e Eqüinos. 2.ed. São Paulo: Varela. 2001.