
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
5-methyltetrahydrofolate: A mandatory support for T677T MTHFR SNP women suffering from premature ovarian insufficiency, endometriosis and/or multiple ART failures
Kristy L Martin1,2; Edouard J Servy2; Yves JR Menezo3*
1 MS4, University of Medicine and Health Sciences, New York, NY, USA
2 Servy institute of Reproductive endocrinology, Augusta, GA, USA.
3 Laboratoire CLEMENT, Paris, France
*Corresponding Author: Yves JR Menezo
Laboratoire CLEMENT, Paris, France.
Email: Yves.menezo@gmail.com
Received : Sep 16, 2021
Accepted : Oct 21, 2021
Published : Oct 28, 2021
Archived : www.jcimcr.org
Copyright : © Menezo YJR (2021).
Abstract
A patients, age 39 in 2019, suffering hypermenorrhea, secondary dysmenorrhea and endometriosis with pelvic adhesions, Normal physical examination with an AMH value of 0.877 ng/L . At this time the couple had been trying to conceive for over 2 years while taking nature made prenatal vitamins and the wife was given 9 rounds of clomid treatments (6–50 mg, 3- 100 mg). She was advised to take DHEA and then started IUI and IVF with no success. On August, 2020, it was elected to check the couple for MTHFR mutation. The woman was found to be homozygous for T677T MTHFR mutation and her spouse homozygous for the C1298C MTHFR mutation but with a subnormal sperm.
The patient and her spouse were both advised to discontinue any vitamins containing folic acid and start vitamins with a daily dose of 1,000 mcg of 5-MTHF (folate) with chelated zinc and a vitamin B complex. On December, 2020 spontaneous conception occurred. On July 27, 2021, a healthy 48.26 cm (19 inches), 3 kg (6 pounds 9 ounces) girl was delivered by c-section.
Keywords: MTHFR 677TT SNP; endometriosis; ART failures; premature ovarian insufficiency; 5MTHF.
Citation: Martin KL, Servy EJ, Menezo YJR. 5-methyltetrahydrofolate: A mandatory support for T677T MTHFR SNP women suffering from premature ovarian insufficiency, endometriosis and/or multiple ART failures. J Clin Images Med Case Rep. 2021; 2(5): 1386.
Introduction
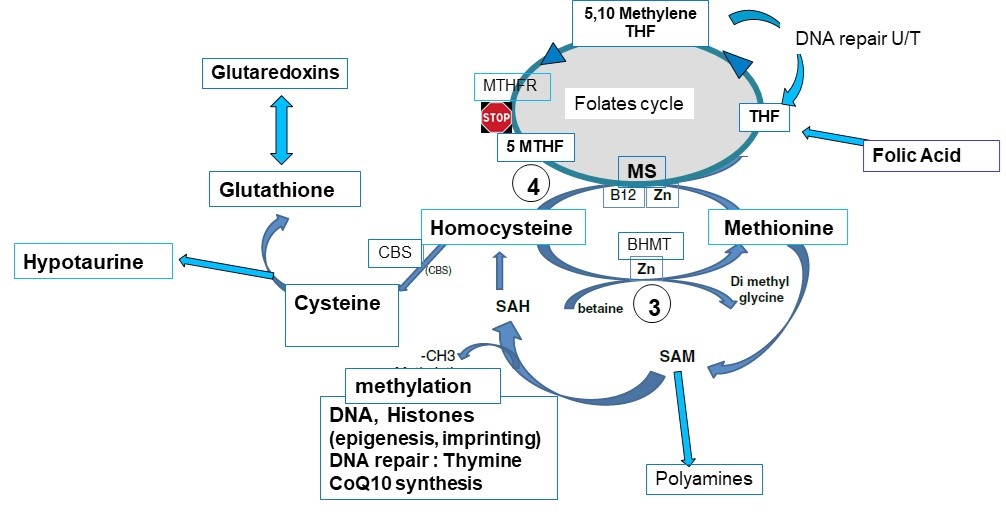
MTHFR is an enzyme involved in the folic acid cycle connected to the 1-carbon cycle (1-CC). MTHFR, located on the short arm of chromosome 1, catalyses the reduction of 5,10 methylenetetrahydrofolate to 5-methytetrahydrofolate, and is used for cellular methylation processes including epigenetic and imprinting regulation via DNA and histones methyl tagging. These two cycles play a major role in DNA repair, but also in gametogenesis, early embryo development, embryo implantation, and pregnancy support [1]. Two common MTHFR polymorphisms are C677T and A1298C, cause reduced MTHFR activity [2,3]. In severe cases can cause hyperhomocysteinemia, homocystinuria, and hypomethioninemia which has been associated with impaired reproductive function including cell division, oocyte development, implantation, follicular atresia [10]. Also, it can be associated with first trimester miscarriages, Assisted Reproduction (ART) failure, endometriosis, and premature ovarian insufficiency [5-8,11]. High doses of folic acid are not a solution for the aforementioned problems, as synthetic folic acid has a poor capacity to enter the folate cycle to form Tetrahydrofolate (THF) and then 5-MTHF. It may cause an increase in serum homocysteine [9]. This can lead to Unmetabolized Folic Acid Syndrome (UFAS). This report reviews the case of a female patient who had a history of stage II endometriosis with premature ovarian insufficiency, one biochemical pregnancy, failed ART attempts - Intrauterine Insemination (IUI) and in-vitro-fertilization (IVF). After discovering the homozygous mutation for MTHFR C677T SNP, the patient was successfully treated with 5-MTHF.
MTHFR SNPs may decrease severely (up to 75%) the formation of 5MTHF, necessary for Homocysteine recycling. It impairs the methylation capacity (especially DNA). The blockade may lead to accumulation of unmetabolized folic acid, and to an increase of circulating Homocyteine.
Case description
SA Gravida 0, Para 0, Abortus 0, presented at 39 years of age in October 2019 with a past medical history of hypermenorrhea, secondary dysmenorrhea and pelvic adhesive disease with stage II endometriosis discovered at the time of a laparoscopy performed in October 2018. Her menarche occurred at the age of 13. She had regular 28–30-day cycles with heavy periods lasting 5 to 7 days. At this time the couple had been trying to conceive for over 2 years while taking nature made prenatal vitamins and the wife was given 9 rounds of clomid treatments (6 – 50 mg, 3- 100 mg).
Normal physical examination with an AMH value of 0.877 ng/mL was noted. Patient was asked to return in November 2019 for an ultrasound. Pelvic ultrasound revealed normal size uterus with bilateral hypo-trophic ovaries. Right ovary with a volume of 1.71 mL, with 1 or 2 antral follicles. Left ovary with a volume of 1.83 mL, with 2 antral follicles noted. At this time the patient was diagnosed with premature ovarian insufficiency. Patient was advised to take DHEA 25 mg 3 times per day. The male factor was considered as sub-normal with a concentration of 20 million sperm cells per ml, a 10% progressive motility and a 4% normal morphology (Kruger criteria). The couple was counselled on intrauterine insemination (IUI), in-vitro-fertilization (IVF) and continuation of commercial routine prenatal vitamins. Patient was then started on an IUI cycle with stimulation using 50 mg of clomid on cycle days (CD) 3-7 and 100 IU of rFSH CD 6-10. Patient returned on November 20,2019, CD 10, where a follicle measuring 20 mm was noted on the left ovary and endometrium 8 mm with a triple layer, estradiol level of 519 pg/ mL and LH level of 5.2 mIU/mL. Following an injection of 10,000 units hCG on Nov 20, IUI was completed on November 22, when ovulation was noted. No conception was noted on December 9, 2019.
Patient returned, January 3, 2020, for a saline infusion sonohysterogram (SIS). Normal uterine size endometrial cavity, no defect and a good expansion were noted. Right ovary had a volume of 10 mL, with a 30 mm functional ovarian cyst noted. Left ovary had a volume of 1.51 mL and 2 antral follicles. Patient had a biochemical pregnancy on July 6, 2020 following a spontaneous conception.
On July 31,2020, the patient returned for IVF. Her ovaries were stimulated with 9 days of 200 IU of rFSH with 150 IU of FSH/LH, and 4 days of .25mg GnRH antagonist on cycle days 7 through 10. Ten oocytes were retrieved. Seven fertilized after intracytoplasmic sperm injection (ICSI). Day 3, four embryos were noted to be 7-8 cells and three 4-6 cells. Further development growth arrested day 3 and there was no embryo transfer.
The patient and her spouse were both advised to discontinue any vitamins containing folic acid and start vitamins with a daily dose of 1,000 mcg of 5-MTHF (folate) with chelated zinc and a vitamin B complex. On December 3, 2020 spontaneous conception occurred and the patient was followed through the first trimester of gestation, then transferred for obstetrical care. On July 27, 2021, a healthy 48.26 cm (19 inches), 3 kg (6 pounds 9 ounces) girl was delivered by c-section.
Discussion and conclusion
This case report is in line with the association between long lasting infertility miscarriages, failed ART attempts and MTHFR Single Nucleotide Polymorphism (SNP). Moderate endometriosis surgically treated, recurrent failed clomid stimulations, failed IUI, biochemical pregnancy and failed ART could not be overcome before treatment with 5-MTHF, the compound located downstream the MTHFR blockade. MTHFR SNP may lead, sooner or later to embryo developmental arrests [1,4,8,14]. This means that patients with endometriosis [11,12], a history of recurrent pregnancy losses, multiple failed IUIs or failed ART should be tested for MTHFR mutations. Homocysteine levels were not obtained in this patient, although it is a weaker marker especially in women, more protected than the men against an increase in homocysteine.
Treatment with exogenous 5-MTHF vs synthetic folic acid, allows the mutated MTHFR SNP problems to be bypassed. It avoids uncertainties due to treatments with high doses of synthetic folic acid, such as Unmetabolized Folic Acid (UMFA) and pseudo-MTHFR syndrome, while possibly improving ovarian quality, and pregnancy outcome [3]. High doses of folic acid can also increase homocysteine via a pseudo MTHFR effect [13] and lead to an adverse competition between natural folate (5- MTHF) and unmetabolized folic acid, for cellular transport and metabolism. Testing patients for an MTHFR mutation prior to IUIs, expensive ART procedure, or pre-implantation genetic screening could possibly help avoid unexplained lack of implantation or recurrent pregnancy losses.
References
- Menezo Y, Clement P, Clement A and Elder K. Methylation: An Ineluctable Biochemical and Physiological Process Essential to the Transmission of Life. Int J Mol Sci. 2020; 21: 9311.
- Frost P, Bloom H., Milos R, et al. A candidate genetic risk factor for vascular disease: A common mutation in methylenetetrahydrofolate reductase. Nature genetics. 1995; 10: 111-113.
- Weisberg I, Tran P, Christensen B, Sibani S, Rozen R. A Second Genetic Polymorphism in Methylenetetrahydrofolate Reductase (MTHFR) Associated with Decreased Enzyme Activity. Molecular genetics and metabolism. 1998; 64: 169-172.
- Silvestris E, Cohen M, Cornet D, et al. Supporting the One-Carbon Cycle Restores Ovarian Reserve in Subfertile Women: Absence of Correlation with Urinary Bisphenol A Concentration. BioResearch open access. 2017; 6: 14-109.
- Servy EJ, Jacquesson-Fournols L, Cohen M, Menezo YJR. MTHFR isoform carriers. 5-MTHF (5-methyl tetrahydrofolate) vs folic acid: A key to pregnancy outcome: a case series. Journal of assisted reproduction and genetics. 2018; 35: 1431-1435.
- Hague WM. Homocysteine and pregnancy. Best practice & research Clinical obstetrics & gynaecology. 2003; 17: 459-469.
- A.B.C. Coumans, P.C. Huijgens, C. Jakobs, R. Schats, J.I.P. de Vries, M.G. van Pampus, G.A. Dekker, Haemostatic and metabolic abnormalities in women with unexplained recurrent abortion, Human Reprod., 2019; 14: 211–214.
- D’Uva M, Di Micco P, Strina I, et al. Hyperhomocysteinemia in women with unexplained sterility or recurrent early pregnancy loss from Southern Italy: A preliminary report. Thrombosis journal. 2007; 5: 10-10.
- Steven W Bailey, June E Ayling. The extremely slow and variable activity of dihydrofolate reductase in human liver and its implications for high folic acid intake. PNAS. 2009; 106: 15424-15429.
- D’Elia P, dos Santos A, Bianco B, Barbosa C, Christofolini D, Aoki T. MTHFR polymorphisms C677T and A1298C and associations with IVF outcomes in Brazilian women. Reproductive biomedicine online. 2014; 28: 733-738.
- Clement A, Cornet N, Alvarez, Brami C, Clement P and Menezo Y, Endometriosis pathogenesis: role played by the oxidative stress due to MTHFR mutations. Fertility and Sterility. 2018; 110: E394- E395.
- Koukoura O, Sifakis S, Spandidos D. DNA methylation in endometriosis (Review) DNA methylation in endometriosis, Molecular Medicine Reports. 2016; 13: 2939-2948.
- Cornet D, Clement A, Clement P, Menezo Y. High doses of folic acid induce a pseudo-methylenetetrahydrofolate syndrome SAGE Open Med Case Reports. 2019; 7: 2050313X19850435.
- Enciso M, Sarasa J, Xanthopoulou L, Bristow S, Bowles, et al. Polymorphisms in the MTHFR gene influence embryo viability and the incidence of aneuploidy. Hum. Genet. May. 2016; 135: 555-568.