
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A review on covid-19 and acute ischemic stroke, malignant cerebral edema & decompressive hemicraniectomy: A perfect storm; tackling this crisis by understanding it
Ardavan Ahmadvand1; Hamidreza Seifmanesh1; Maryam Ghandali1; Ali Afrasiabi2; Vida Tajiknia3*; Mahtab Amoujani4
1 Department of Internal Medicine, Iran University of Medical Sciences, Tehran, Iran.
2 Department of Internal Medicine, Rasoul Akram Hospital, Iran University of Medical Sciences (IUMS), Tehran, Iran.
3 Rasoul Akram Hospital, Iran University of Medical Sciences (IUMS), Tehran, Iran.
4 Department of Endocrinology, Tehran University of Medical sciences, Tehran, Iran.
*Corresponding Author: Vida Tajiknia1 & Mahtab Amoujani2
1 Rasoul Akram Hospital, Iran University of Medical
Sciences (IUMS), Tehran, Iran; 2 Department of Endocrinology, Tehran University
of Medical sciences, Tehran, Iran.
Email: tajiknia@gmail.com
Received : Sep 14, 2021
Accepted : Oct 22, 2021
Published : Oct 29, 2021
Archived : www.jcimcr.org
Copyright : © Tajiknia V (2021).
Abstract
Since the world was hit by novel coronavirus pandemic, so many challenges for all healthcare providers have been arisen. It is safe to say that no specialty was singled out in the matter of different complication from this viscous covid-19 situation and neurologists and neurosurgeon were no different. There are some studied reporting neurological complication associated with coronavirus infections but when it comes to life threatening and acute neurological complications such as strokes and malignant cerebral edema the data is scant. Here we are going to review the possible pathophysiology of this phenomenon, the relationship between covid-19 and acute ischemic stroke and malignant cerebral edema by taking a closer look at current data regarding this matter.
Keywords: covid-19; acute ischemic stroke; malignant cerebral edema; covid-19 associated neurological complications.
Abbreviations: DHC: Decompressive Hemicraniectomy; ELVO: Emergent Large Vessel Occlusion; MCE: Malignant Cerebral Edema.
Citation: Ahmadvand A, Seifmanesh H, Ghandali M, Afrasiabi A, Tajiknia V. A review on covid-19 and acute ischemic stroke, malignant cerebral edema & decompressive hemicraniectomy: A perfect storm; tackling this crisis by understanding it. J Clin Images Med Case Rep. 2021; 2(5): 1388.
Introduction
In December 2019 the world was hit by new coronavirus pandemic with variety of symptoms. Neurologic manifestations have been reported as part of the different clinical presentation of the disease [1]. First reports came from China indicating a higher incidence of cerebrovascular complication associated with covid-19 [2]. With this published data Concerns about potential neurological complications of COVID-19 have been alarmingly increasing and obligated all researchers and clinicians to investigate this matter in a more serious fashion. Higher rates of strokes among patients with covid-19 has been discussed, but data regarding the outcomes of COVID-19 patients developing acute ischemic stroke due to large vessel occlusion (LVO) are limited [3].
Acute Ischemic Stroke (AIS) is a life-threatening complication of coronavirus disease 2019 infection. New reports suggest an association between COVID-19 and AIS, although the underlying mechanism remains uncertain [4].
Cryptogenic stroke has been reported in 53 to 67% of AIS in COVID-19 patients [5,6].
Malignant edema is a well-described consequence of acute ischemic stroke and can be worsened by the presence of hypercarbia induced by respiratory failure. Considering the higher incidence of cerebrovascular complications in patients with COVID-19, it is crucial for clinicians to be aware of the risk of rapidly progressive cerebral edema in the setting of respiratory failure of covid-19 infection and ischemic stroke [7].
Here we are going to review the reports about covid-19 associated acute ischemic stroke and malignant cerebral edema by describing the pathophysiological mechanisms and detailed reported cases.
Pathophysiology
The main possible pathophysiological mechanisms contributed to cerebrovascular events are illustrated in this diagram.
As it is demonstrated above vasculopathy related to covid-19 infection and its cytokine causing endothilitis out of CNS vascular structures is one of the main mechanism [8,9].
Another mechanism attributed to this phenomenon is coagulopathy along with sepsis in critically ill patients with higher level of D-dimer [10-13].
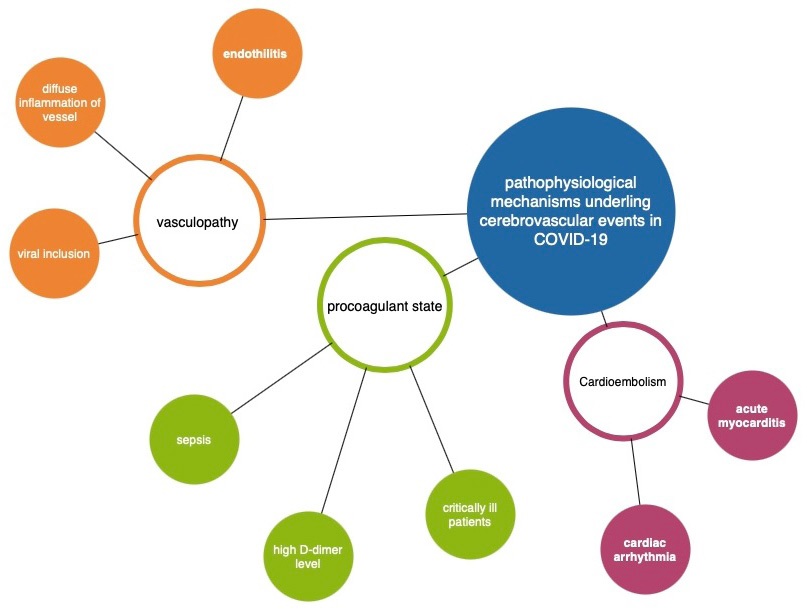
A third possible mechanism is cardio-embolic stroke, as cardiac arrythmia and acute myocarditis which are complication of cardiovascular system in covid-19 patients [14]. Cardioembolism was considered as the cause of AIS in respectively 15% and 24% of COVID-19 patients in two studies[5,6]. Finally, other rare causes of AIS have been reported in COVID-19 patients, including five cases of cervical artery dissections [1,6,15] and one case of focal cerebral arteriopathy in a 12-year-old boy [16].
Acute ischemic stroke (AIS) and Covid-19
Acute Ischemic Stroke prevalence has been reported about 1.3 to 4.7% of COVID-19 patients [17].
There have been some studies about ischemic stroke in covid-19 patients [18]. In a study in new York clinical presentation between two group of patients were assessed one with covid-19 and ischemic stroke the other without covid-19 and only ischemic stroke the results were informative and surprising, COVID-19 patients were younger, had higher admission National Institutes of Health Stroke Scale Score (NIHSS), higher peak D-dimer level, were more likely to have cryptogenic stroke subtype and a proximal large vessel occlusion, were more likely to be treated with anticoagulation, and had a higher inpatient mortality. The global COVID-19 Stroke registry including 174 patients from 16 countries confirmed that AIS patients with COVID-19 had a higher risk for severe disability and death [19].
In a surveillance study in UK on Neurological and neuropsychiatric complications of COVID-19 in 153 patients, 57 cases with acute ischemic stroke reported all with diagnosis of severe covid-19 and mostly the pattern of stroke was involvement of large vessels [5]. Because of the nature of this study it is important to pay close attention as many clinicians who is on the first line of admitting covid-19 patients considering the possible acute cerebrovascular events.
Table 1: Acute ischemic stroke (AIS) & Covid-19.
Country |
Study |
Sample size |
Onset of stroke during covid |
Treatment |
Stroke mechansim |
Outcome |
Covid respiratory symptoms |
UK |
Survilance |
153 |
Not mentioned |
Not mentioned |
Large artery |
Not mentioned |
All with severe covid syndrome |
UAE, |
Case series |
22 |
18 cases stroke was presenting symptoms |
acute recanalization treatment in 2
|
predominantly large artery. |
Six died, three from complications related to stroke and three from other COVID-19 complications. |
12 had lung involvement and respiratory problems |
Spain |
Cohort |
841 |
In 4 cases was presenting symtopma |
therapeutic anticoagulation |
The posterior arterial territory in 4 cases
|
Not mentioned |
11 had respirator involvement |
China |
Cohort |
6 of 78 patients |
2 presented with stroke |
Not mentioned |
Not mentioned |
Not mentioned |
5 of these patients had been categorized as severe COVID-19 and 1 had been categorized as non-severe |
NYU Langone Health |
retrospective case review |
4 of 17 patients |
All in first week of admission with no initial symptoms of stroke |
therapeutic anticoagulation |
large vessel ischemic stroke |
Not mentioned |
suspicious lung findings with multifocal, peripheral, ground-glass opacities in both lungs |
Mount Sinai Health System, New York |
Case series |
5 |
From 2 hours to 28 hours after having covid-19 symptoms |
therapeutic anticoagulation in all |
large-vessel stroke |
Discharged to rehabilitation facility 2 cases |
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection was diagnosed in all five patients. |
In a study in dubai 22 covid-19 patient with acute ischemic stroke were reported in 81.8% unfortunately stroke was the first symptom, with the use of surgical and medical treatment the mortality was significant (6 of 22). The pattern of stroke in this report was large territory infarctions. All patients were young adults [21]. This data shows the severity of covid-19 role ischemic stroke.
In a systematic review of 841 covid-19 patients with neurological manifestations, 11 cases were reported with ischemic stroke in 4 cases it was the first presenting sign. What is really interesting in this study is the fact that Unlike ICH, ischemic stroke occurred independently of COVID-19 severity, even in the absence of systemic manifestations. In fact, 4 patients had this serious complication in the recovery phase of the disease [1] which can be translated to the immense need of follow up of these patients also an emphasize on future guidelines in this particular matter.
In a large cohort study in Wuhan, China on neurological manifestation of covid it was reported 6 ischemic stroke cases which 5 of them were categorized as sever covid cases. Like other studies 30% of cases presenting symptoms were ischemic stroke, there were no other data regarding the outcome of these cases [2].
Another surprising report is from a study in NYU Langone Health 17 covid-19 patients were under neuro imaging for completely unrelated reason to covid-19 but amazing findings were 4 of them showed symptoms of ischemic stroke. This particular report is alarmingly concerning because it expresses that sever respiratory symptoms of covid-19 is not necessarily an indicator or even a requirement for development of cerebral ischemic stroke [22]. This data is concerning and highlight the need of even more detailed and careful evaluation of patients
In another report from New York of 5 patients all diagnosed with severe covid-19 syndrome ischemic stroke with large vessel involvement was reported. The novelty of this report was the fact that all patients were younger than 50. And their mean NIHSS score (score used to determine severity of stroke) was 17, consistent with severe large-vessel stroke [23]. This is also an interesting topic for future studies to investigate the relationship between covid-19 and large vessel stroke in young population.
Malignant cerebral edema (MCE) and covid-19
The scarcity of available reports of covid-19 patients with acute ischemic stroke and malignant cerebral edema makes this issue formidable to discuss although because of the importance of this subject we have decided to review all possible data.
In a study from a single center in New York all covid-19 patients with emergent large vessel occlusions with risk of developing MCE (risk was defined >50% of middle cerebral artery involvement on CT imaging) were reported. The risk assessment of 2 patient for MCE was not significant and they received medical treatment. 3 cases developed MCE and underwent DHC. The outcome of this group of 3 patients were good and only one mortality was reported due to the concurrent ST-segment–elevation myocardial infarction [24].
This report is showing promising results; COVID-19 patients with large territorial ischemic stroke can actually benefit from DHC and have a good outcome.
Table 2: Malignant cerebral edema (MCE) & Covid-19.
Country |
Study |
Sample size |
Stroke pattern |
Treatment |
outcome |
New York, US |
retrospective single-center |
7 |
ELVO in the internal carotid artery or middle cerebral artery |
4 patients underwent decompressive hemicraniectomy (DHC) |
4 of 7 died |
Westchester Medical Center/New York Medical College |
Case report |
1 |
posterior division right MCA/parietal stroke |
Due to patient thrombocytopenia no anticoagulant therapy was administrated |
malignant cerebral edema/hemorrhagic transformation of the infarct in day 4 |
Philippine General Hospital |
Case report |
1 |
acute left internal carotid artery (ICA) infarct |
emergent left DH |
Deceased due to respiratory failure |
Italy |
Case report – child |
1 |
large right middle cerebral artery (RMCA) ischemia |
bridging systemic thrombolysis followed by endovascular thrombectomy |
good functional recovery, residual hemiplegia.. |
In a case report from New York one covid-19 patient with ischemic stroke surprisingly no large vessel involvement was reported after 4 days patient developed MCE and was deceased [7]. The key point of this report was the pathophysiological aspect of Hypercarbic respiratory failure associated with the development of fulminant cerebral edema [25]. Acute respiratory distress syndrome (ARDS) is a known complication of COVID-19 and can result in a severe and rapid respiratory failure leading to hypercarbia.
In another case report from Italy a 11 year old boy with serological evidence of covid-19 infection presented with acute ischemic stroke firstly managed medically but after 12 hours patient developed MCE and underwent emergency DHC which was successful [26].
The importance of this case report lies in the fact that pediatric patients are also in danger of developing the worst scenario caused by covid-19 crisis.
In one case report from Philippine, a 36 year old female during home quarantine was presented with acute ischemic stroke and underwent emergency DH but due to respiratory failure patient was deceased [27].
Discussion
A meta-analysis showed that the incidence of acute ischemic stroke in COVID-19 patients ranges from 0.9 to 2.7% [4]. Acute ischemic stroke has been in some cases the presenting symptom of disease and it was not always with a linear pattern in association with covid-19 severity [20].
Because of the pattern of AIS associated with covid-19 is mostly large vessel [5]. Special attention is needed to be paid. Malignant cerebral edema is the most feared complication of acute ischemic stroke in the setting of covid-19 and in some reports DHE was shown to be life -saving but the mortality is still high [7,11,26,28].
Conclusion
In conclusion, our review reported that acute ischemic stroke is a serious complication in covid-19 cases and it can rapidly cause patient’s deterioration by developing malignant cerebral edema. Data about outcome of these patients specially the one who underwent DHS is limited and further studies are needed. Also all clinicians must be familiar with the risk of AIS and its presentation to improve quality of care.
References
- Romero-Sánchez CM, Díaz-Maroto I, Fernández-Díaz E, SánchezLarsen Á, Layos-Romero A, et al. Neurologic manifestations in hospitalized patients with COVID-19: The ALBACOVID registry Neurology. 2020; 95: e1060–70.
- Mao L, Jin H, Wang M, Hu Y, Chen S, et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurology. 2020; 77: 683–90.
- Escalard S, Maïer B, Redjem H, Delvoye F, Hébert S, et al. Treatment of Acute Ischemic Stroke due to Large Vessel Occlusion With COVID-19: Experience From Paris. Stroke 2020; 51: 2540– 3.
- Tan Y-K, Goh C, Leow AST, Tambyah PA, Ang A, et al. COVID-19 and ischemic stroke: a systematic review and meta-summary of the literature. Journal of Thrombosis and Thrombolysis 2020; 50: 587–95.
- Meppiel E, Peiffer-Smadja N, Maury A, Bekri I, Delorme C, et al. Neurologic manifestations associated with COVID-19: A multicentre registry. Clinical Microbiology and Infection : The Official Publication of the European Society of Clinical Microbiology and Infectious Diseases. 2021; 27: 458–66.
- Hernández-Fernández F, Sandoval Valencia H, Barbella-Aponte RA, Collado-Jiménez R, Ayo-Martín Ó, et al. Cerebrovascular disease in patients with COVID-19: neuroimaging, histological and clinical description. Brain : A Journal of Neurology 2020; 143: 3089–103.
- Dakay K, Kaur G, Mayer SA, Santarelli J, Gandhi C. Cerebral Herniation Secondary to Stroke-Associated Hemorrhagic Transformation, Fulminant Cerebral Edema in Setting of COVID-19 Associated ARDS and Active Malignancy. Journal of Stroke and Cerebrovascular Diseases: The Official Journal of National Stroke Association. 2020; 29: 105397.
- Varga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet (London, England). 2020; 395: 1417–8.
- Zhang Y, Xiao M, Zhang S, Xia P, Cao W, et al. Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19. The New England Journal of Medicine. 2020; 382: e38.
- Giannis D, Ziogas IA, Gianni P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. Journal of Clinical Virology : The Official Publication of the Pan American Society for Clinical Virology. 2020; 127: 104362.
- González-Pinto T, Luna-Rodríguez A, Moreno-Estébanez A, Agirre-Beitia G, Rodríguez-Antigüedad A, et al. Emergency room neurology in times of COVID-19: Malignant ischaemic stroke and SARS-CoV-2 infection. European Journal of Neurology. 2020; 27: e35–6.
- Boehme AK, Ranawat P, Luna J, Kamel H, Elkind MS v. Risk of Acute Stroke After Hospitalization for Sepsis: A Case-Crossover Study. Stroke. 2017; 48: 574–80.
- Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. Journal of Thrombosis and Haemostasis : JTH. 2020; 18: 844–7.
- Zheng Y-Y, Ma Y-T, Zhang J-Y, Xie X. COVID-19 and the cardiovascular system. Nature Reviews Cardiology. 2020; 17: 259–60.
- Morassi M, Bigni B, Cobelli M, Giudice L, Bnà C. Bilateral carotid artery dissection in a SARS-CoV-2 infected patient: causality or coincidence? Journal of Neurology. 2020; 267: 2812–4.
- Mirzaee SMM, Gonçalves FG, Mohammadifard M, Tavakoli SM, Vossough A. Focal Cerebral Arteriopathy in a Pediatric Patient with COVID-19. Radiology. 2020; 297: E274–5.
- Mahammedi A, Saba L, Vagal A, Leali M, Rossi A, et al. Imaging of Neurologic Disease in Hospitalized Patients with COVID-19: An Italian Multicenter Retrospective Observational Study. Radiology. 2020; 297: E270–3.
- Guilmot A, Maldonado Slootjes S, Sellimi A, Bronchain M, Hanseeuw B, et al. Immune-mediated neurological syndromes in SARS-CoV-2-infected patients. Journal of Neurology 2021; 268: 751–7.
- Yaghi S, Ishida K, Torres J, mac Grory B, Raz E, et al. SARS-CoV-2 and Stroke in a New York Healthcare System. Stroke. 2020; 51: 2002–11.
- Varatharaj A, Thomas N, Ellul MA, Davies NWS, Pollak TA, et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: a UK-wide surveillance study. The Lancet Psychiatry. 2020; 7: 875–82.
- Khan M, Ibrahim RH, Siddiqi SA, Kerolos Y, Al-Kaylani MM, et al. COVID-19 and acute ischemic stroke - A case series from Dubai, UAE. International Journal of Stroke: Official Journal of the International Stroke Society. 2020; 15: 699–700.
- Jain R, Young M, Dogra S, Kennedy H, Nguyen V, Raz E. Surprise Diagnosis of COVID-19 following Neuroimaging Evaluation for Unrelated Reasons during the Pandemic in Hot Spots. AJNR American Journal of Neuroradiology. 2020; 41: 1177–8.
- Oxley TJ, Mocco J, Majidi S, Kellner CP, Shoirah H, et al. LargeVessel Stroke as a Presenting Feature of Covid-19 in the Young. The New England Journal of Medicine. 2020; 382: e60.
- Liang JW, Reynolds AS, Reilly K, Lay C, Kellner CP, et al. COVID-19 and Decompressive Hemicraniectomy for Acute Ischemic Stroke. Stroke. 2020; 51: e215–8.
- Roh D, Merkler AE, Al-Mufti F, Morris N, Agarwal S, et al. Global cerebral edema from hypercapnic respiratory acidosis and response to hyperosmolar therapy. Neurology 2016; 86: 1556–8.
- Scala MR, Spennato P, Cicala D, Piccolo V, Varone A, et al. Malignant cerebral infarction associated with COVID-19 in a child. Child’s Nervous System: ChNS: Official Journal of the International Society for Pediatric Neurosurgery. 2021: 1–5.
- Chan KIP, Salonga AEM, Khu KJO. Decompressive hemicraniectomy for acute ischemic stroke associated with coronavirus disease 2019 infection: Case report and systematic review. Surgical Neurology International. 2021; 12: 116.
- Patel SD, Kollar R, Troy P, Song X, Khaled M, et al. Malignant Cerebral Ischemia in A COVID-19 Infected Patient: Case Review and Histopathological Findings. Journal of Stroke and Cerebrovascular Diseases: The Official Journal of National Stroke Association. 2020; 29: 105231.