
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
An exploring study of defecography, digital rectal examination, and balloon expulsion test for screening and predicting of symptoms with defecation disorders
Xiaotong Tian1; Qi Ge2; Chunli Liang1; Ruifang Li1; Shurui Bu1*
1 Department of Gastroenterology, Jinshan Hospital Affiliated to Fudan University, Shanghai 201508, China.
2 Department of Medical Statistics, School of Public Health, Sun Yat-sen University,Guangdong 510080, China.
*Corresponding Author: Shurui Bu
Department of Gastroenterology and Hepatology,
Jinshan Hospital Affiliated to Fudan University, No.
1508 Longhang Road, Shanghai 201508, China.
Email: bushurui@fudan.edu.cn
Received : Sep 11, 2021
Accepted : Oct 22, 2021
Published : Oct 29, 2021
Archived : www.jcimcr.org
Copyright : © Bu S (2021).
Abstract
Background: Defecation disorder is widely common in constipa� tion, which diagnosed by Defecography (DF), Digital Rectal Examina� tion (DRE), Balloon Expulsion Test (BET), and others. It remains not clear that which one would be more accessible and effective due to no comparison of defecation disorders among diagnosis, classification and treatments, based on symptoms. The aim of this study is to evalu� ate which method should be used more easy operational and accu� rately in clinics with prediction based on symptoms.
Methods: Consecutive patients with chronic constipation (Rome III criteria, n=141) underwent DF, DRE, and BET between 2014 and 2018. Those examination findings and symptoms with constipation were re� corded and analyzed.
Results: Of the 141 patients included in our study, 67 (47.5%) had a sensation of incomplete defecation, 66 (46.8%) of these were identi� fied to have clinical symptoms with obstruction. The sensitivity and specificity of DF for identifying patients with obstruction were 42.4% and 78.7%, respectively; the positive predictive value was 63.6%, with [AUC: 0.62 (95% CI: 0.54-0.71)]. The sensitivity and specificity of DRE for identifying patients with a sensation of incomplete defecation were 76.1% and 44.6%, respectively; the positive predictive value was 55.4%, with [AUC: 0.60 (95% CI: 0.53-0.68)]. It is only useful dignosis for abdominal distention used BET. The sensitivity and specificity of BET for identifying patients with abdominal distention were 75.0% and 43.6%, respectively, with [AUC: 0.59 (95% CI: 0.51-0.68)]. The positive correlation between sacrum-rectal separate and obstruction was ob� served in the study, the similar correlation was observed in between Pelvic floor hernia and abdominal distention.
Conclusions: It is a valuable tool for diagnosis and further treat� ment of these six symptoms used an index combining DF and DRE. In addition, DF and DRE would be a more accessible and effective clini� cal tool for screening and diagnosis of patients with obstruction and a sensation of incomplete defecation, respectively. However, it would be only valuable tool for abdominal distention used BET. Both methods could facilitate the selection of appropriate patients for further exami� nations and tailored therapy accordingly
Keywords: defecation disorder; defecography; DRE; BET; screening; predicting
Abbreviations: DF: Defecography; DRE: Digital Rectal Examination; BET: Balloon Expulsion Test; DD: Defeca� tion Disorder; ARA: Anorectal Angle; RC: Rectocele; PD: Perineum Descending; SPFS: Spastic Pelvic Floor Syndrome; S-RS: Sacrum-Rectal Separate; SP: Splanch� noptosis; PFH: Pelvic Floor Hernia; AMP: Anterior Mu� cosal Prolapse; PMH: Puborectalis Muscle Hypertro� phy; IRI: Internal Rectal Intussusception; ERP: External Rectal Prolapse.
Citation: Tian X, Ge Q, Liang C, Li R, Bu S. An exploring study of defecography, digital rectal examination, and balloon expul� sion test for screening and predicting of symptoms with defecation disorders. J Clin Images Med Case Rep. 2021; 2(5): 1389.
Introduction
Constipation is a common gastrointestinal symptoms through out the world in primary care, which affects the quality of life and increases medical costs related to diagnosis and treat� ment, especially the elderly. The previous study showed that its prevalence has been steadily increasing from 11% to 18% in communities [1]. Based on the literature [2], the occurrence of constipation has also been shown to vary according to race and the regions that sufferers live in. Although the symptoms of constipation are generally harmless, they are sometimes warn� ing signs of more serious conditions including colorectal cancer, cardiocerebrovascular and kidney disease [3-5]. Patients with chronic constipation often have mental and psychological disor� ders such as anxiety and depression [6,7], which seriously affect the physical and mental health of the patients and significantly reduces their quality of life.
The constipation is classified into two types, namely func� tional and organic. Nevertheless, functional constipation sub� types are considered to include functional defecation disorders, slow transit constipation, and a combination of the former two. Due to literatures [8,9], the functional defecation disorders di� agnosed in 12%-24% of patients’ complaints with a sensation of incomplete defecation and obstruction.
The defecation disorders could be accurately diagnosed by some examinations in clinics, including DF, DRE, and BET [10]. DF is a traditional barium enema technique for dynamic and static observation of the structure and function of the anorec� tal and pelvic floor using X-rays during defecation[11]. Although the function of the anal sphincter function, presence of dyssyn� ergia, and fecal impaction can be fully shown by DRE, the def� ecation disorder should be diagnosed with DF and (or) BET, not solely [12]. It is unclear for patients with defecation disorders how to select these three methods in clinics. Hence, our aim is to how to fastly, accurately and conveniently select one meth� od, which would be more suitable for first screening in primary care, based on symptoms.
Materials and methods
Characteristics of enrolled patients
A total of 141 patients aged from 18 to 80 were enrolled with clinical symptoms of constipation and received examination in our hospital between 2014 and 2018, including DF, DRE, and BET. The clinical diagnosis of constipation is mainly based on the Rome III diagnostic criteria and patient complaints [9,13,14], including a history of the foregoing symptoms for at least 6 months and having at least 2 of the following complaints for at least 3 months: difficulty in passing stools, dry balls or hard feces, anorectal obstruction that needs manual assistance, and a frequency of bowel movement <3 times a week. All patients were asked to complete a questionnaire including their names, gender, constipation symptoms including frequency of bowel movements, hard stools, difficulty in passing stools, a sensation of incomplete defecation, obstruction, abdominal distention, presence of anorectal organic diseases such as tumor, surgical history etc � � son’s, hypothyroidism and so on) after patients were excluded. The study protocol was approved by the Research Ethics Com� mittee of our Hospital and written informed consent was obtained from all participants.
Defecography examination
Usually, defecography can be performed without any prepa� ration. At most, a 60-120 mL glycerin enema has to be � istered.
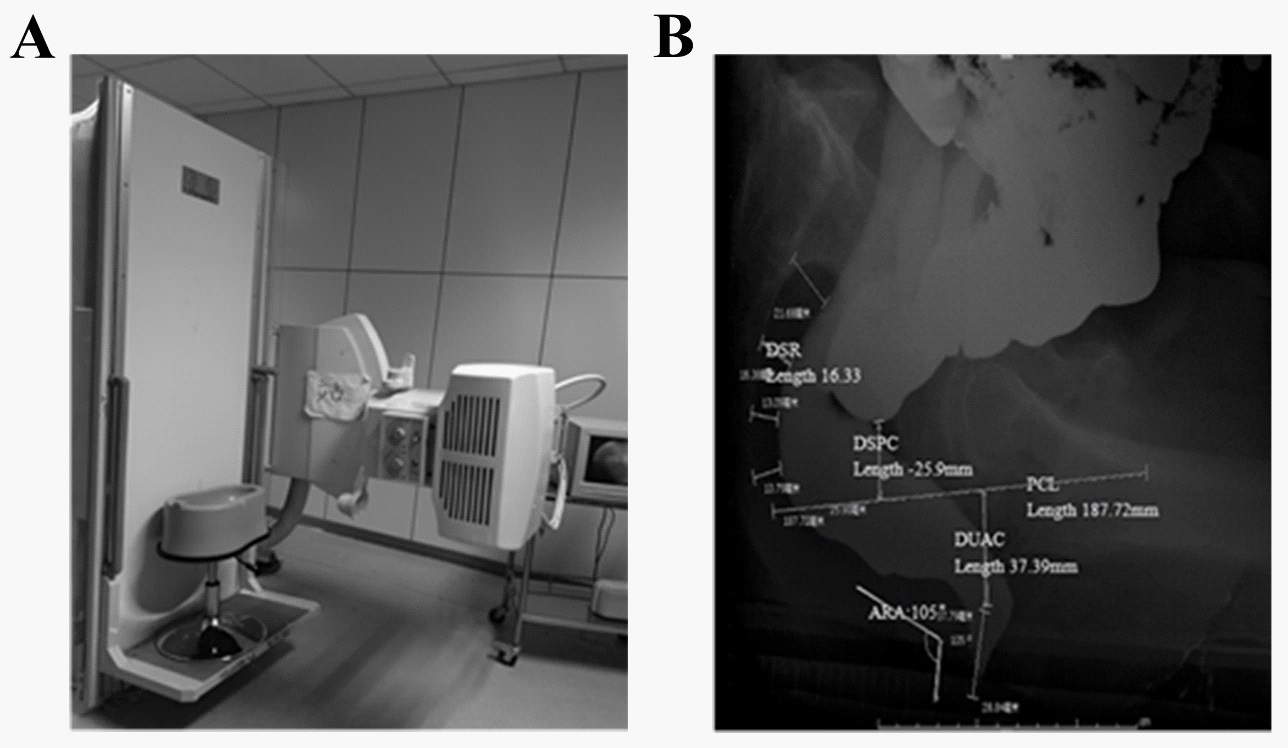
A multi-functional digital perspective photography system and a DS-1 seater were used in the present study. First, each patient was asked to cooperate actively with the radiologists. Second, each patient adopted a lateral (distal) supine position and was injected with barium through the anus. � tient was permitted to sit sideways on a self-made pervious and rotator X-ray barrel for the convenience of dynamic observation of the rectal and anal canal morphology and the mucosa during rest, lift, contraction and defecation. The X-ray barrel is shown in Figure 1A.
Digital rectal examination
DRE is not only important but also the most revealing part of a clinical evaluation [15]. This manoeuvre consisted of 2 steps. With the patient in the left lateral position, and hips flexed to 90°. Firstly, the anus and surrounding tissue were exposed to good light to check for skin of the anus. Next, digital palpation was performed by slowly advancing a lubricated and gloved in� dex finger into the rectum. Not only the resting and squeeze sphincter tone of the anal sphincter, but also puborectalis mus� cle could be assessed by asking the subject to squeeze for as long as possible. Simultaneously, the examiner should perceive relaxation of the external anal sphincter and (or) the puborec� talis muscle, together with perineal descent. Next, the patient then was asked to push and bear down as if to defecate when the examiner placed the left hand on the abdomen to assess the pushing effort [12]. Any absence of these findings should suggest the suspicion for dyssynergic defecation.To ensure the veracity of the responses, each step should be repeated once or twice [15,16]. The presence of any 2 of the following find� ings was used to clinically diagnose dyssynergia: the inability to contract the abdominal muscles, inability to relax the anal sphincter, a paradoxic contraction of the anal sphincter, or the absence of perineal descent.
Balloon expulsion test
The balloon expulsion test [17] is a simple, clinical examina� tion to judge whether the function of rectum and pelvic floor muscles is abnormal. In this test, A 4-cm long balloon tipped catheter is inserted in to the ampulla rectal and inflated with warm water at 37o C or air to 50 mL. The subject is asked to take the habitual defecation posture to expel the balloon while timed.
Major measurements and observations
DF: According to the modified diagnostic criteria for X-ray defecography reported in a previous study [18], the measure� ments and observation made in the present study mainly in� cluded: 1) The Anorectal Angle (ARA), which was defined as the angle of the longitudinal axis of the anal canal and the posterior rectal line, mainly reflected the activity of the puborectalis. The value at rest was between 92 and 114 degrees; during muscle contraction the ARA becomes more acute, while during the relaxing phase it became obtuse. In spastic pelvic floor syndrome, the ARA was unchanged during defecation compared to the angle at rest. 2) The distance between the anorectal junction and the pubococcygeal line (DUAC) is the vertical distance from the upper midpoint of the anal canal to the pubococcygeal line (the joint of the lower margin of the pubic symphysis to the tip of the coccyx). The value of perineum descending was > 30 mm. 3) The distance between the sigmoid colon and the pubococ� cygeal line (DSPC); the vertical distance from the lowest point of the sigmoid colon or the small intestine to the pubococcy� geal line should be a negative value except for the condition of splanchnoptosis. 4) The distance between the sacrum and the rectum (DSR); the distance between the anterior wall of the third sacrum and the posterior wall of the rectum. The value of the Sacrum-Rectal Separaton (S-RS) should be > 20 mm; the above measurements are shown in Figure 1B.
DRE: The presence of any stricture, spasm, tenderness, mass, blood or stool were noted. It assess the strength of anal resting sphincter and rectal squeeze tone. The normal should be considered to be relaxed for former and increased for later. In addition to assess the anal sphincter tone with defecation whether relaxed or not, the change of ARA should be observed. If normal, the former should be relaxed, the ARA would be in� creased, compared with the resting.
BET: The normal result of this test is considered within one to two minutes, whereas, dyssynergia is suspected if the patient is unable to expel the balloon in under two minutes.
Statistical analysis
SPSS Statistics for Windows software (ver. 22.0, SPSS Inc., US) and R 3.6.1 software were used for all statistical analyses. Mea� surements of normally distributed data are presented as the mean ± standard deviation (χ ± SD). Enumeration data are de� scribed as constituent ratios. A chi-squared test was performed to compare the rates between two groups. Logistic regression was used to fit model to detect the constipation symptoms and ROC curves were used to evaluate classification effect of the predictors. A value of P < 0.05 was considered to be of statistical significance.
Results
Basic demographic characteristics of the enrolled cohort
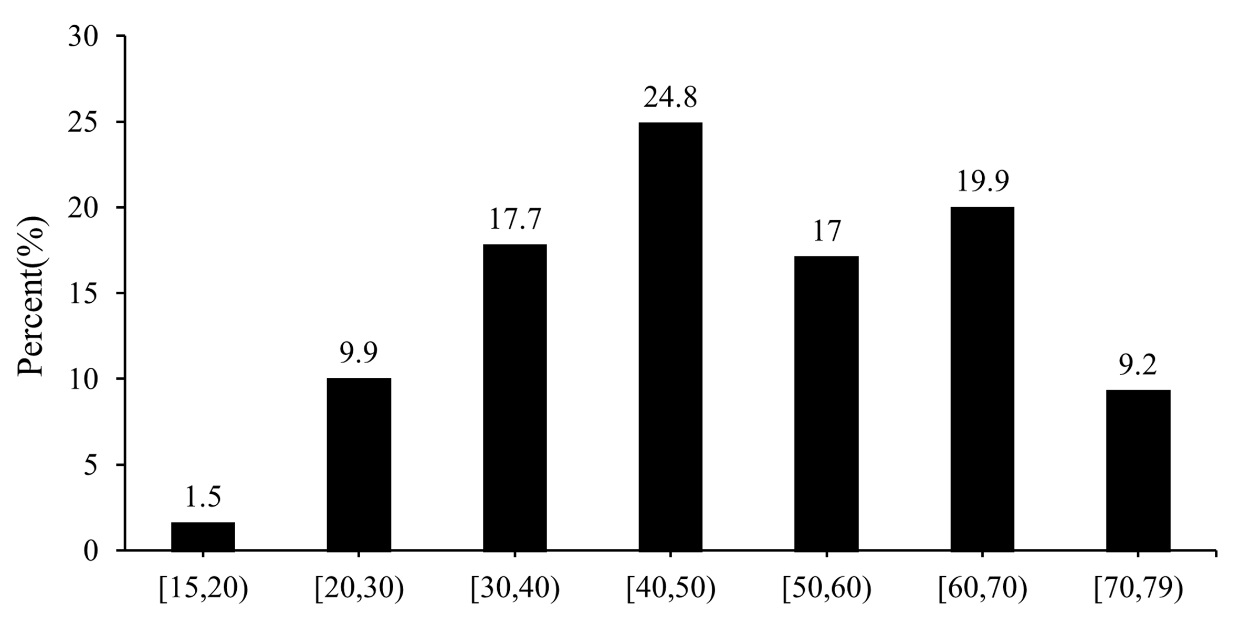
In the present study, 141 patients (34 male and 107 female, with a M/F ratio of 1:3.2) with clinical symptoms of constipa� tion who received examinations in our hospital between 2014 and 2018. The main clinical symptoms were a low frequency of bowel movements, hard stools, difficulty in passing stools and a sensation of incomplete defecation, as well as a feeling of ob� struction and abdominal distension, which accounted for 28.4- 58.2% of patients (Table 1). In different age ranges, it was found that constipation was more common in the middle and older age groups (30-69 years), the incidence being 17.7% at 30-39 years, 24.8% at 40-49 years, 17.0% at 50-59 years and 19.9% at 60-69 years old, respectively. A significant difference in the def� ecation disorder distribution between patients < 30 years old and patients > 70 years old was revealed (Figure 2).
Table 1: Basic demographic characteristics of patients.
Variables |
N |
% |
Age (years) < 50 |
76 |
53.9 |
Gender (Male) |
34 |
24.1 |
Clinical symptoms |
|
|
Low frequency of bowel movements |
66 |
46.8 |
Hard stools |
82 |
58.2 |
Difficulty in passing stools |
43 |
30.5 |
A sensation of incomplete defecation |
67 |
47.5 |
Obstruction |
66 |
46.8 |
Abdominal distention |
40 |
28.4 |
Defecography |
|
|
Rectocele (RA) |
111 |
78.7 |
Perineum descending (PD) |
92 |
65.3 |
Spastic pelvic floor syndrome (SPSF) |
40 |
28.4 |
Sacrum-rectal separate (S-RS) |
20 |
14.2 |
Splanchnoptosis (SP) |
22 |
15.6 |
Pelvic floor hernia (PFH) |
33 |
23.4 |
External rectal prolapse (ERP) |
1 |
0.7 |
Puborectalis muscle hypertrophy (PMH) |
5 |
3.6 |
Internal rectal intussusception (IRI) |
3 |
2.1 |
Anterior mucosal prolapse (AMP) |
5 |
3.6 |
Regular defecography |
1 |
0.7 |
RC: Rectocele; PD: Perineum Descending; SPSF: Spastic Pelvic Floor Syndrome; S-RS: Sacrum-Rectal Separate; SP: Splanchnoptosis; PFH: Pelvic Floor Hernia ERP: External Rectal Prolapse; PMH: Puborectalis Muscle Hypertrophy; IRI: Internal Rectal Intussusceptions; AMP: Anterior Mucosal Prolapse.
Next, we evaluated the DF findings and classified constipa� tion patients in the 141 patients. Rectocele (RC) and perineum descending (PD) are the two main pathogens found in defecation disorders with DF, accounting for 78.7% and 65.3% in the 141 patients, respectively. We further attempted to analyze whether an index combining DF and others would be useful for the screening and diagnosis of symptoms with defecation dis� orders.
Correlation analysis of constipation symptoms and defeco� graphic findings
In our present study, we found that the clinical symptoms of a lower frequency of bowel movements, hard stools, difficult defecation, and a sensation of incomplete evacuation, were dif� ficult to associate with any defecography indicators (Table 2), while obstruction as a clinical symptom was related to sacrumrectal separate (S-RS) defecography (χ2 = 5.034, P=0.025). In ad� dition, abdominal distension was not only related to PD but also with Pelvic Floor Hernia (PFH) (P=0.031, P=0.001). These find� ings indicated that it could be diagnosed and confirmed with DF of the S-RS with obstruction, which once had abdominal disten� tion, and could be further confirmed to be a defecation disorder with PD or PFH.
Table 2: The relationship between clinical symptoms and DF indicators.
|
N (%) |
Low frequency of bowel movements |
Hard stools |
Difficulty in passing stools |
A sensation of incomplete defecation |
Obstruction |
Abdominal Distention |
RC |
|
|
|
|
|
|
|
Yes |
111 (78.8) |
50 (45.0) |
63 (56.8) |
33 (29.7) |
52 (46.8) |
51 (45.9) |
32 (28.8) |
No |
30 (21.2) |
16 (53.3) |
19 (63.3) |
10 (33.3) |
15 (50) |
15 (50) |
8 (26.7) |
PD |
|
|
|
|
|
|
|
Yes |
92 (34.7) |
44 (47.8) |
50 (54.3) |
26 (28.2) |
43 (46.7) |
44 (47.8) |
31(33.7)* |
No |
49 (65.3) |
22 (44.9) |
32 (65.3) |
17 (34.7) |
24 (49.0) |
22 (44.9) |
9 (18.4) |
SPSF |
|
|
|
|
|
|
|
Yes |
40 (28.4) |
20 (50.0) |
28 (70.0) |
13 (32.5) |
15 (37.5) |
18 (45.0) |
9 (22.5) |
No |
101 (71.6) |
46 (45.5) |
54 (53.5) |
30 (29.7) |
52 (51.5) |
48 (47.5) |
31 (30.7) |
S-RS |
|
|
|
|
|
|
|
Yes |
20 (14.2) |
8 (40) |
8 (40.0) |
7 (35.0) |
10 (50.0) |
14 (70.0)* |
4 (20.0) |
No |
121 (85.8) |
58 (47.9) |
74 (61.2) |
36 (29.8) |
57 (47.1) |
52 (43.0) |
36 (29.8) |
SP |
|
|
|
|
|
|
|
Yes |
22 (15.6) |
12 (54.5) |
13 (59.1) |
6 (27.3) |
11 (50.0) |
8 (36.4) |
6 (27.3) |
No |
119 (84.4) |
54 (45.4) |
69 (58.0) |
37 (31.1) |
56 (47.1) |
58 (48.7) |
34 (28.6) |
PFH |
|
|
|
|
|
|
|
Yes |
33 (23.4) |
11 (33.3) |
18 (54.5) |
8 (24.2) |
17 (51.5) |
19 (57.6) |
17 (51.5)* |
No |
108 (76.6) |
55 (50.9) |
64 (59.3) |
35 (32.4) |
50 (46.3) |
47 (43.5) |
23 (21.3) |
ERP |
|
|
|
|
|
|
|
Yes |
1(7.1) |
1 (100) |
1 (100.0) |
0 (0) |
1 (100.0) |
0 (0) |
1 (100.0) |
No |
140 (92.9) |
65(46.4) |
81 (57.9) |
43 (30.7) |
66 (47.1) |
66 (47.1) |
39 (27.9) |
PMH |
|
|
|
|
|
|
|
Yes |
5 (3.5) |
3 (60.0) |
4 (80.0) |
2 (40.0) |
3 (60.0) |
3 (60.0) |
2 (40.0) |
No |
136 (96.5) |
63(46.3) |
78 (57.4) |
41 (30.1) |
64 (47.1) |
63 (46.3) |
38 (27.9) |
IRI |
|
|
|
|
|
|
|
Yes |
3 (2.1) |
1(33.3) |
1 (33.3) |
1 (33.3) |
1 (33.3) |
2 (66.7) |
1 (33.3) |
No |
138 (97.9) |
65(47.1) |
81 (58.7) |
42 (30.4) |
66 (47.8) |
64 (46.4) |
39 (28.3) |
AMP |
|
|
|
|
|
|
|
Yes |
5 (3.5) |
1(20.0) |
2 (40.0) |
3 (60.0) |
3 (60.0) |
3 (60.0) |
1 (20.0) |
No |
136 (96.5) |
65(47.8) |
80 (58.8) |
40 (29.4) |
64 (47.1) |
63 (46.3) |
39 (28.7) |
RD |
|
|
|
|
|
|
|
Yes |
1 (7.1) |
1(100.0) |
0 (0) |
0 (0) |
1 (100.0) |
0 (0) |
0 (0) |
No |
140 (92.9) |
65(46.4) |
82 (58.6) |
43 (30.7) |
66 (47.1) |
66 (47.1) |
40 (28.6) |
* representing that the P value of the significant test of chi-squared is smaller than 0.05; RC: Rectocele; PD: Perineum Descending; SPSF: Spastic Pelvic Floor Syndrome; S-RS: Sacrum-Rectal Separate; SP: Splanchnoptosis; PFH: Pelvic Floor Hernia ERP: External Rectal Prolapse; PMH: Puborectalis Muscle Hypertrophy; IRI: Internal Rectal Intussusceptions; AMP: Anterior Mucosal Prolapse; RD: Regular Defecography.
Based on patients with obstruction, the positive correla� tion between S-RS and a feeling of obstruction was found by multi-factor logistic regression (OR=3.1, P=0.03). The sensitivity and specificity of DF for identifying patients with this symptom were 42.4% and 78.7%, respectively. In addition, the positive predictive value was 63.6%, with the AUC of 0.62 and 95% confi� dence interval of 0.54-0.71 (Table 3). Based on patients with ab� dominal distention, the positive correlation between PFH and abdominal distention was found by multi-factor logistic regres� sion (OR=0.43, P=0.003). The sensitivity and specificity of DF for identifying patients with this symptom were 42.5% and 87.1%, respectively, with AUC of 0.67 and 95% confidence interval of 0.57-0.77.
Table 3: Performance Characteristics of DF in the Diagnosis of Obstruction
|
|
95% CI |
|
|
Estimated value |
Lower limit |
Upper limit |
Sensitivity |
0.424 |
0.306 |
0.552 |
Specificity |
0.787 |
0.673 |
0.869 |
For any particular positive test result, the probability that it is: |
|
|
|
True positive |
0.636 |
0.477 |
0.772 |
False positive |
0.364 |
0.228 |
0.523 |
Correlation analysis of constipation symptoms and DRE findings
The change of ARA, when push efforts, is normal in a total of 92 patients (65.2%), and 49 patients (34.8%) is unchanged or less than 90 degree, compared with the resting (Table 4). There was a negative correlation between the change of ARA and a sensation of incomplete defecation detected by multifactor logistic regression (OR=0.39, P=0.011). The sensitivity and specificity of DRE for identifying patients with a sensation of incomplete defecation were 76.1% and 44.6%, respectively; the positive predictive value was 55.4%, with AUC of 0.60 and 95% confidence interval of 0.53-0.68. It was not valuable diag� nosis for a sensation of incomplete defecation used DF, with the AUC of 0.56 and 95% confidence interval of 0.48-0.63 (Table 5). There is no significant difference between other symptoms and DRE findings detected by detected by multi-factor logistic re� gression.
Table 4: Detection Rate of DRE in 141 Patients With Symptoms.
|
N(%) |
Low frequency of bowel movements |
Hard stools |
Difficulty in passing stools |
A sensation of incomplete defecation |
Obstruction |
Abdominal distention |
ARA |
|
|
|
|
|
|
|
Increased |
92 (65.2) |
40 (60.6) |
49 (59.8) |
25 (58.1) |
51 (76.1)* |
41 (62.1) |
28 (70) |
Less than 90° or unchanged |
49 (34.8) |
26 (39.4) |
33 (40.2) |
18 (42.9) |
16 (23.9) |
25 (37.9) |
12 (30) |
Anal resting tone |
|
|
|
|
|
|
|
Normal |
27 (19.1) |
16 (24.2) |
16 (19.5) |
5 (11.6) |
13 (19.4) |
12 (18.2) |
10 (25) |
Increased |
107 (75.9) |
46 (69.7) |
62 (75.6) |
36 (83.7) |
50 (74.6) |
49 (74.2) |
27 (67.5) |
Decreased |
7 (5.0) |
4 (6.1) |
4 (4.9) |
2 (4.7) |
4 (6.0) |
5 (7.6) |
3 (7.5) |
Anal squeeze pressure |
|
|
|
|
|
|
|
Normal |
107 (75.9) |
48 (72.7) |
60 (73.2) |
35 (81.4) |
51 (76.1) |
52 (78.8) |
30 (75) |
Decreased |
34 (24.1) |
18 (27.3) |
22 (26.8) |
8 (18.6) |
16 (33.9) |
14 (21.2) |
10 (25) |
Anal sphincter relaxation |
|
|
|
|
|
|
|
Normal |
57 (40.4) |
25 (37.9) |
32 (39.0) |
18 (41.9) |
25 (37.3) |
27 (40.9) |
16 (40) |
Impaired |
65 (46.1) |
30 (45.5) |
39 (47.6) |
20 (46.5) |
33 (49.3) |
31 (47.0) |
20 (50) |
Paradoxic contraction |
19 (13.5) |
11 (16.7) |
11 (13.4) |
5 (11.6) |
9 (13.4) |
8 (12.1) |
4 (10) |
* representing that the P value of the significant test of chi-squared is smaller than 0.05; ARA: Anorectal Angle.
Table 5: Performance Characteristics of DRE in the Diagnosis of a sensation of incomplete defecation
|
|
95% CI |
|
|
Estimated value |
Lower limit |
Upper limit |
Sensitivity |
0.761 |
0.639 |
0.85 |
Specificity |
0.446 |
0.332 |
0.57 |
For any particular positive test result, the probability that it is: |
|
|
|
True positive |
0.554 |
0.447 |
0.657 |
False positive |
0.446 |
0.343 |
0.553 |
Correlation analysis of constipation symptoms and BET findings
A total of 141 patients (38.3%) had normal balloon expul� sion time, 87 patients (61.7%) could not expel the balloon or prolonged balloon expulsion time. It has an valuable dignosis of abdominal distention used BET. The sensitivity and speciicity of BET for identifying patients with abdominal distention were 75.0% and 43.6%, respectively, with AUC of 0.59 and 95% con� fidence interval of 0.51-0.68. However, there was no significant difference in patients with abdominal distention between DF and BET (Delong test: P=0.24).
Correlation analysis of constipation symptoms and the combined index findings
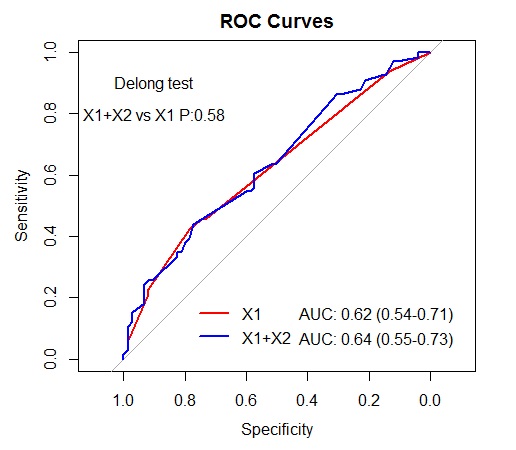
We further attempted to analyze whether an index combin� ing DF and DRE would be useful for the detection and diagno� sis of defecation disorders. The sensitivity and specificity of the combined index for identifying patients with obstruction were 43.9% and 77.3%, respectively. In addition, the positive predic� tive value was 63.0%, with the AUC of 0.64 and 95% confidence interval of 0.55-0.73 (Figure 3). And there is no difference in the classification effect between DF index and the combined index by comparing the areas under the ROC curves (AUC) (Delong test, P=0.64).
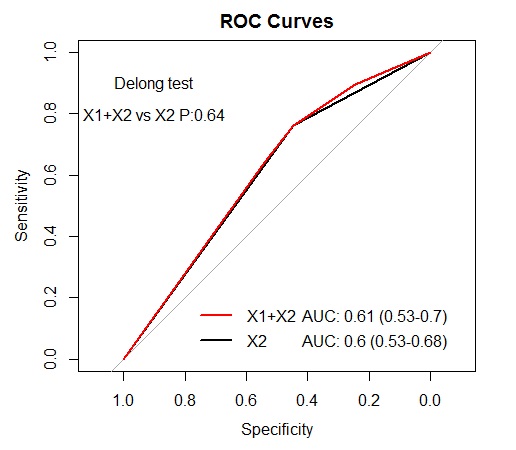
The sensitivity and specificity of an index combining DF and DRE for identifying patients with a sensation of incomplete def� ecation were 44.6% and 76.1%, respectively. In addition, the positive predictive value was 63.0%, with the AUC of 0.61 and 95% confidence interval of 0.53-0.70 (Figure 4). And there is no significant difference in a sensation of incomplete defecation between DRE and combined examination (Delong test, P=0.64).
The sensitivity and specificity of an index combining DF and DRE for identifying patients with abdominal distention were 42.5% and 87.1%, respectively, with AUC of 0.68 and 95% con� fidence interval of 0.59-0.79. And there is no significant differ� ence in abdominal distention between BET and combined ex� amination (Delong test, P=0.64).
Predictive logistic model for symptoms with examination
According to ROC curves, the comparison between DF, DRE, and BET, based on symptoms, were in Table 6. It was valuable diagnosis for these six symptoms used an index combining DF and DRE. BET was a useful tool for one symptom. Based on these results, the logistic model containing an index combining DF and DRE findings and six symptoms were as follows:
Table 6: Classification Effect of Predictors for six Outcomes (AUC(95%CI)).
|
X1(DF) |
X2(DRE) |
X3(BET) |
X2+X3 |
X1+X2 |
Y1(Low frequency of bowel movements) |
0.63(0.54-0.71)* |
0.58(0.48-0.67) |
0.57(0.49-0.65) |
0.61(0.52-0.70)* |
0.64(0.55-0.74)* |
Y2(Hard stools) |
0.63(0.54-0.72)* |
0.58(0.50-0.67)* |
0.51(0.43-0.59) |
0.58(0.50-0.67)* |
0.64(0.55-0.73)* |
Y3(Difficulty in passing stools) |
0.57(0.48-0.67) |
0.61(0.52-0.71)* |
0.52(0.44-0.61) |
0.61(0.52-0.71)* |
0.63(0.52-0.73)* |
Y4(A sensation of incomplete defecation) |
0.56(0.48-0.63) |
0.60(0.53-0.68)* |
0.52(0.44-0.60) |
0.60(0.53-0.68)* |
0.61(0.53-0.70)* |
Y5(Obstruction) |
0.62(0.54-0.71)* |
0.57(0.48-0.66) |
0.53(0.45-0.61) |
0.56(0.46-0.65) |
0.64(0.55-0.73)* |
Y6(Abdominal distention) |
0.67(0.57-0.77)* |
0.53(0.45-0.62) |
0.59(0.51-0.68)* |
0.61(0.52-0.71)* |
0.68(0.58-0.78)* |
* represents that the P value of the significant test of AUC is smaller than 0.05
* based on Y2, Y3, andY4,it would be considered as the same model between X2 and an index combining X2 and X3, due to X3 excluded with P > 0.5.
The logistic model containing an index combining DF and DRE findings and obstruction was as follows: logit(π)= - 0.58 + 1.09 X104 – 0.51 X105 + 0.66 X106 + 0.58 X109 + 0.31 X201 + 0.18 X202 – 0.22 X203: [X104: S-RS: [(+): 1, (-): 0], X105: SP: [(+): 1, (-): 0], X106: PFH: [(+): 1, (-): 0], X109: IRI: [(+): 1, (-): 0], X201: ARA: [Unchanged or less than 90°): 1, (Increased): 0], X202: Anal testing tone: [(Normal): 0, (Increased): 1, (Decreased): 2], X203: Anal squeeze pressure: [(inadequate contraction): 1, (Normal): 0], and cut-off value was 0.495.
The logistic model containing an index combining DF and DRE findings and a sensation of incomplete defecation was as follows: logit(π)=0.26 – 0.25 X103 – 0.86 X201: [X103: SPFS: [(+): 1, (-): 0], X201: ARA: [(Unchanged or less than 90°): 1, (In� creased): 0], and cut-off value was 0.428.
The logistic model containing an index combining DF and DRE findings and low frequency of bowel movements was as fol� lows: logit(π)= 0.28 – 0.27 X101 + 0.66 X105 - 0.74 X106 – 1.61 X110+ 0.17 X201 - 0.32 X202 + 0.24 X203 + 0.09 X204:[X101: RC: [(+): 1, (-): 0], X105: SP: [(+): 1, (-): 0], X106: PFH: [(+): 1, (-): 0], X110: AMP: [(+): 1, (-): 0], X201: ARA: [Unchanged or less than 90°): 1, (Increased): 0], X202: Anal testing tone: [(Normal): 0, (Increased): 1, (Decreased): 2], X203: Anal squeeze pressure: [(inadequate contraction): 1, (Normal): 0], X204: Anal sphincter relaxation: [(Impaired): 1, (Paradoxic contraction): 2, (Normal): 0], and cut-off value was 0.426.
The logistic model containing an index combining DF and DRE findings and hard stools was as follows: logit(π)= 0.30 – 0.28 X102 + 0.56 X103 - 0.83 X104 + 0.82 X108 - 0.80 X109 - 0.48 X110 + 0.34 X201 + 0.34 X203: [X102: PD: [(+): 1, (-): 0], X103: SPSF: [(+): 1, (-): 0], X104: S-RS: [(+): 1, (-): 0], X108: PMH: [(+): 1, (-): 0], X109: IRI: [(+): 1, (-): 0], X110: AMP: [(+): 1, (-): 0], X201: ARA: [Unchanged or less than 90°): 1, (Increased): 0], X203: Anal squeeze pressure: [(inadequate contraction): 1, (Normal): 0]], and cut-off value was 0.662.
The logistic model containing an index combining DF and DRE findings and difficulty in passing stools was as follows: logit(π)= - 1.19 - 0.19 X102 – 0.27 X106 + 1.26 X110 + 0.42 X201 + 0.47 X202 - 0.37 X203:[X102: PD: [(+): 1, (-): 0], X106: PFH: [(+): 1, (-): 0], X110: AMP: [(+): 1, (-): 0], X201: ARA: [Unchanged or less than 90°): 1, (Increased): 0], X202: Anal testing tone: [(Normal): 0, (Increased): 1, (Decreased): 2], X203: Anal squeeze pressure: [(inadequate contraction): 1, (Normal): 0]], and cut-off value was 0.254.
The logistic model containing an index combining DF and DRE findings and abdominal distention was as follows: logit(π)= - 1.62 + 0.65 X102 – 0.39 X103 - 0.53 X104 + 1.29 X106 + 0.16 X201:[X102: PD: [(+): 1, (-): 0], X103: SPSF: [(+): 1, (-): 0], X104: S-RS: [(+): 1, (-): 0], X106: PFH: [(+): 1, (-): 0], X201: ARA: [Un� changed or less than 90°): 1, (Increased): 0]], and cut-off value was 0.405.
Discussion
Constipation is a very common disorder worldwide, with the variable symptoms of this gastrointestinal tract occurring most frequently in children, women and the elderly. The examination of the causes and treatment of constipation has recently be� come a very significant field of research [19]. As is shown that in previous study [20], detailed clinical examination, and in par� ticular a DRE, DF, and (or) BET is indispensable in the evaluation of a patient with defecation disorder constipation. It can fully evaluate whether a patient has acute or chronic constipation, and whether the condition is primary or secondary. In our pres� ent study, it is a useful tool for patients with adominal disten� tion used BET, and it is valuable dignosis for patients with these six symptoms used an index combining DF and DRE. However, DF [21] is currently considered as the primary method for the detection of obstructed defecation, as it produces more accurate results than a barium enema and colonoscopy. At present, the DF used in clinics is limited, due to its radiation exposure, poor tolerance, lack of trained physician, embarrassment, and performed with MR defecography [22]. However, Foti et al. [23- 25] pointed out that MR defecography was less sensitive than Xray defecography for the diagnosis of enterocele, rectocele and rectal prolapse (56%, 38% and 85%, respectively) [26]. Patients with DRE, considered as physical testing, could be selected for further appropriate physiologic testing and treatment. It would be limited in clinics due to trainees lack of adequate skills, priva� cy and the poor consent. Hence, based on patients with symp� toms, it is important for clinicians to select the most examina� tions, and further to guide treatment.
We found that the etiology of constipation had a tendency to be diversified. Unlike reported in previous investigations [27], RC was detected in 20 (40%) vs 111 (78.7%). No abnormalities were observed in RC in 30 cases that had previously undergone colonoscopy. And a previous study [28] reported that detec� tion rates of Internal rectal intussusception (IRI) and Anterior Mucosal Prolapse (AMP) were 37.5% and 15%, respectively. In contrast, unlike in our study, it was 2.1% and 5.5%, respectively. These different results might be associated with the patient’s position, requirement for radiologists, and the types and traits of enemas employed.
Ramage et al. [29] concluded that the results of defecog� raphy were poorly correlated with the severity of ‘patient re� ported’ symptoms. Unlike the previous study, there was a substantial concordance in our study, not only with significant differences between obstruction and S-RS, but also between abdominal distention and PFH observed. It further shows that it is not obviously diagnosed by the DRE in patients with obstruc� tion and abdominal distention in our present study. However, the S-RS can diagnose the 63.6% of obstruction in DF, and the 63.0% of it in an index combining DF and DRE, which suggests that patients with this symptom may be related to abnormal anatomy of defecation-related condition. It is found that DF could be used as a much more accessible diagnostic method for patients with obstruction and an index combining DF and DRE can further assess for the screening and diagnosis of the cause(s) of their symptoms, to guide treatment in clinics [30]. The treatment of constipation includes drug therapy, anorectal myectomy, biofeedback or surgery, but in general these treat� ments have poor efficacy due to various etiology [31,32]. Thus treatment decisions should not depend solely on this type of feedback.
Based on patients with a sensation of incomplete defeca� tion, in our study, the ARA in pushing efforts is unchanged or the change is not more than 90 degree, compared with the rest� ing. It seems that the sensitivity and specificity of DRE for iden� tifying patients with a feeling of incomplete defecation were 76.1% and 44.6%, respectively. At the same time, there are the 55.4% of patients with a feeling of incomplete defecation who could be diagnosed by DRE. An index combining DF and DRE is no better than DRE alone, and we conclude that DRE would be first line screening for a sensation of incomplete defecation. Like to previous study [16], which showed that the symptoms of incomplete evacuation was independent predictors of func� tional defecation disorder on multivariate analysis. However, the previous study [33] showed that defecation disorders could be detected by DRE with a sensitivity of 75% and a specificity of 87%. This different result may be explained by the fact that it is associated with most physicians and trainees who has inad� equate skills. Hence, we infer that this symptom could associate with pelvic floor spasm, and the pathogenesis may be related to functional defecation disorders. Those patients need to be further accurately diagnosed by the Anorectal Manometry [34], who may have a certain benefit from biofeedback therapy.
Due to literature [35,36], BET is a useful screening test for identifying patients with defecation disorder, and the previous study showed that the specificity of it is high (80-90%), although the sensitivity is low (50%). However, based on previous study [37], one study showed that the prevalence of a positive test in favor of dyssynergia varies between 23% and 67%. Another study suggested a specificity of 89%, and a sensitivity of 88%. In addition, Grossi et al. [38] pointed that the BET has an 80%-90% specificity and sensitivity ranges from 33% to 94% for dyssyner� gia as defined by anorectal manometry (which itself remains a controversial diagnostic tool given its possible high false positive rate [39]). Unlike the previous study, there is significant dif� ference between abdominal distention and BET in our present study, with the sensitivity of 75.0% and specificity of 43.6%. We consider that this different result may be related to testing tech� niques, body positions and types of balloons. However, an index combining DF and DRE is no better than BET and DF alone, and we conclude that BET or DF would be first line screening for abdominal distention.
In additon, based on ROC curves, an index combining DF and DRE could be as valuable diagnosis of these six symptoms. At the same time, low frequency of bowel movements, and hard stools could be detected by DF with a sensitivity of 36.4% and a specificity of 81.3%, and a sensitivity of 91.5% and a specific� ity of 25.4%, respectively. Difficulty in passing stools, and hard stools could be detected by DRE with a sensitivity of 79.1% and a specificity of 37.8%, and a sensitivity of 57.3% and a specificity of 55.9%, respectively. In addition, an index combining DF and DRE is no better than one used solely. However, there is no sig� nificant difference between above examinations and symptoms detected by multi-factors logistic regression. This phenomenon could be associated with our samples. Hence, it needs further explore these results in the future.
Some phenomena in our research data are worth noting. First, consistent with previous studies, the prevalence of consti� pation in females was higher than in males, a finding that may be explained by the characteristic female physiological form, such as a history of birth and degeneration of the pelvic floor muscles. Second, the prevalence of constipation was greater in the elderly, probably due to reduced intestinal movement be� cause of a more sedentary life style and eating less of a diet? Thus, the suggestion is put forward that patients should do more exercise and increase their intake of water and dietary fiber.
The present study has a number of limitations. First, is the lack of a control group of ‘healthy volunteers’. All patients in the study had been referred due to the presence of constipation symptoms, although these may not fully explain both the high prevalence of symptoms and the DF, DRE, and BET findings. Sec� ond, multiple factors may affect the occurrence of constipation, including age, sex, eating habits and the education level of pa� tients. In addition, our study did not analyze the impact of these factors on bowel movements, which may cause sample bias. Fi� nally, the sample size was relatively small. Therefore, a larger cohort of patients will be required in future studies to refine the distribution of constipation types for these symptoms so as to provide a more accurate decision making basis in the clinic.
Our study suggests that symptoms together with DRE or DF can be a useful tool for detecting and recognizing of a defecation disorder not only may facilitate an accurate diagnosis , tailored treatment but also lead to an improved clinical outcome, which can be widely applied in clinics and primary center. However, it is much more accessible and effective for such symptoms used one method solely.
Conclusions
In conclusion, it is necessary as well as primary for patients with obstruction to perform the DF examination. And DRE can be used for early identifying and predicting those who present� ing symptoms of a sensation of incomplete defecation, which could be benefit from selecting tailored management. Suspi� cion of dyssynergic defecation on a proper DRE should be confirmed with anorectal manometry and/or DF, which associate with spastic pelvic floor muscle. Hence, it needs further refine� ment to develop more accurate and sensitive diagnostic indica� tors to simplify our understanding of defecation disorders. The logistic model containing an index combining DF and DRE find� ings, based on symptoms, would be valuable for clinicians to diagnosis and guide treatment in the future.
Declarations
Ethics approval and consent to participate: The Research Ethics Committee of Jinshan Hospital Affiliated to Fudan Univer� sity provided ethical approval. Written informed consent was obtained from all participants
Consent for publication: Not applicable.
Availability of data and material: The datasets used and/or analyzed during the current study are available from the cor� responding author on reasonable request.
Competing interests: The authors declare that they have no conflict of interest.
Funding: This research was supported by the Science and Technology Commission of Shanghai Municipality (Grant No. 16411972100). The funder had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript of the manuscript.
Authors' contributions: SB was responsible for the conception and design of the study as well as the acquisition and analy sis of data. SB revised and commented the draft. XT drafted the manuscript, and XT was responsible for acquisition and analysis of data as well as statistical analysis. QG was in charge of arrangement of large data, statistical analysis, and prediction of models. CL was responsible for acquisition and analysis of data. RL was in charge of acquisition, analysis of data and searching latest literatures. All authors read and approved the final manuscript.
Acknowledgements: The authors sincerely acknowledge the excellent statistical advice and help from Prof. Jinxin Zhang, PhD.
References
- Goyal O, Bansal M, Sood A. Clinical and anorectal manometry profile of patients with functional constipation and constipation-predominant irritable bowel syndromeJ. Indian J Gastroenterol. 2019; 38: 211-219.
- Singh P, Surana R, Soni S, et al. Cross cultural comparison of constipation profiles at tertiary care centers between India and USAJ. Neurogastroenterol Motil. 2018.
- Black CJ, Ford AC. Chronic idiopathic constipation in adults: epidemiology, pathophysiology, diagnosis and clinical managementJ. Med J Aust. 2018; 209: 86-91.
- Knudsen K, Krogh K, Ostergaard K, et al. Constipation in parkin� son’s disease: Subjective symptoms, objective markers, and new perspectives J. Mov Disord. 2017; 32: 94-105.
- Prichard D O, Bharucha A E. Recent advances in understanding and managing chronic constipationJ. F1000Res. 2018; 7.
- Huang L, Zhu Q, Qu X, et al. Microbial treatment in chronic con� stipationJ. Sci China Life Sci. 2018.
- Escalante J, McQuade RM, Stojanovska V, et al. Impact of che� motherapy on gastrointestinal functions and the enteric ner� vous systemJ. Maturitas. 2017; 105: 23-29.
- Skardoon GR, Khera AJ, Emmanuel AV, et al. Review article: Dys� synergic defaecation and biofeedback therapy in the pathophys� iology and management of functional constipationJ.. Aliment Pharmacol Ther. 2017; 46: 410-423.
- Lacy BE, Mearin F, Chang L, et al. Bowel Disorders J. Gastroenter� ology. 2016; 150: 1393-1407.
- Ghoshal UC. Chronic constipation in Rome IV era: The Indian perspectiveJ.. Indian J Gastroenterol. 2017; 36: 163-173.
- Lalwani N, El SR, Kamath A, et al. Imaging and clinical assess� ment of functional defecatory disorders with emphasis on defe� cographyJ. Abdom Radiol (NY). 2019.
- Tantiphlachiva K, Rao P, Attaluri A, et al. Digital rectal examina� tion is a useful tool for identifying patients with dyssynergia J. Clin Gastroenterol Hepatol, 2010; 8: 955-960.
- Yiannakou Y, Piessevaux H, Bouchoucha M, et al. A randomized, double-blind, placebo-controlled, phase 3 trial to evaluate the efficacy, safety, and tolerability of prucalopride in men with chronic constipation J. Am J Gastroenterol. 2015; 110: 741-748.
- Emmanuel A, Cools M, Vandeplassche L, et al. Prucalopride im� proves bowel function and colonic transit time in patients with chronic constipation: an integrated analysisJ.. Am J Gastroen� terol. 2014; 109: 887-894.
- Rao SS, Patcharatrakul T. Diagnosis and Treatment of Dyssyner� gic DefecationJ.. J Neurogastroenterol Motil. 2016; 22: 423-435.
- Goyal O, Bansal M, Sood A. Clinical and anorectal manometry profile of patients with functional constipation and constipa� tion-predominant irritable bowel syndromeJ.. Indian J Gastro� enterol. 2019; 38: 211-219.
- Skardoon GR, Khera AJ, Emmanuel AV, et al. Review article: Dys� synergic defaecation and biofeedback therapy in the pathophys� iology and management of functional constipationJ. Aliment Pharmacol Ther. 2017; 46: 410-423.
- Andrade L C, Correia H, Semedo L C, et al. Conventional video� defecography: Pathologic findings according to gender and age J. Eur J Radiol Open. 2014; 1: 1-5.
- Bellini M, Usai-Satta P, Bove A, et al. Chronic constipation diag� nosis and treatment evaluation: the “CHRO.CO.DI.T.E.” study J. BMC Gastroenterol. 2017; 17: 11.
- Videlock EJ, Lembo A, Cremonini F. Diagnostic testing for dyssyn� ergic defecation in chronic constipation: meta-analysisJ.. Neuro� gastroenterol Motil. 2013; 25: 509-520.
- Wald A, Bharucha AE, Cosman BC, et al. ACG clinical guideline: management of benign anorectal disorders J. Am J Gastroen� terol. 2014; 109: 1141-1157.
- Lalwani N, Moshiri M, Lee J H, et al. Magnetic resonance imag� ing of pelvic floor dysfunctionJ. Radiol Clin North Am. 2013; 51: 1127-1139.
- Vanbeckevoort D, Van Hoe L, Oyen R, et al. Pelvic floor descent in females: comparative study of colpocystodefecography and dynamic fast MR imaging J. J Magn Reson Imaging. 1999; 9: 373- 377.
- Farah H, Laurent N, Phalippou J, et al. Postoperative pelvic pain: An imaging approachJ.. Diagn Interv Imaging. 2015; 96: 1065- 1075.
- Poncelet E, Rock A, Quinton J F, et al. Dynamic MR defecography of the posterior compartment: Comparison with conventional X-ray defecography J. Diagn Interv Imaging, 2017; 98: 327-332.
- Ratuapli SK, Bharucha AE, Noelting J, et al. Phenotypic identification and classification of functional defecatory disorders us� ing high-resolution anorectal manometryJ.. Gastroenterology. 2013; 144: 314-322.
- Poncelet E, Rock A, Quinton J F, et al. Dynamic MR defecography of the posterior compartment: Comparison with conventional X-ray defecography J. Diagn Interv Imaging, 2017; 98: 327-332.
- Martin-Martin G P, Garcia-Armengol J, Roig-Vila J V, et al. Mag� netic resonance defecography versus videodefecography in the study of obstructed defecation syndrome: Is videodefecography still the test of choice after 50 years? J. Tech Coloproctol, 2017; 21: 795-802.
- Ramage L, Georgiou P, Qiu S, et al. Can we correlate pelvic floor dysfunction severity on MR defecography with patient-reported symptom severity? J. Updates Surg. 2018; 70: 467-476.
- Kim N Y, Kim D H, Pickhardt P J, et al. Defecography: An Overview of Technique, Interpretation, and Impact on Patient Care J. Gas� troenterol Clin North Am, 2018; 47: 553-568.
- Sharma A, Rao S. Constipation: Pathophysiology and Current Therapeutic Approaches J. Handb Exp Pharmacol. 2017; 239: 59-74.
- Liu W C, Wan S L, Yaseen S M, et al. Transanal surgery for ob� structed defecation syndrome: Literature review and a singlecenter experience J. World J Gastroenterol. 2016; 22: 7983- 7998.
- Tantiphlachiva K, Rao P, Attaluri A, et al. Digital rectal examina� tion is a useful tool for identifying patients with dyssynergia J. Clin Gastroenterol Hepatol. 2010; 8: 955-960.
- Carrington EV, Heinrich H, Knowles CH, et al. Methods of ano� rectal manometry vary widely in clinical practice: Results from an international surveyJ.. Neurogastroenterol Motil. 2017; 29: e13016.
- Chiarioni G, Kim SM, Vantini I, et al. Validation of the balloon evacuation test: Reproducibility and agreement with findings from anorectal manometry and electromyography J. Clin Gas� troenterol Hepatol. 2014; 12: 2049-2054.
- Patcharatrakul T, Rao S. Update on the Pathophysiology and Management of Anorectal Disorders J. Gut Liver. 2018; 12: 375- 384.
- Rao SS. Advances in diagnostic assessment of fecal incontinence and dyssynergic defecation J. Clin Gastroenterol Hepatol. 2010; 8: 910-919.
- Wald A, Bharucha A E, Cosman B C, et al. ACG clinical guideline: management of benign anorectal disorders J. Am J Gastroen� terol. 2014; 109: 1141-1157, 1058.
- Grossi U, Carrington E V, Bharucha A E, et al. Diagnostic accuracy study of anorectal manometry for diagnosis of dyssynergic def� ecation J. Gut. 2016; 65: 447-455.