
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Case report of three distinctive pulmonary toxicities related to durvalumab (PD-L1 inhibitor) consolidation therapy in locally advanced non-small cell lung cancer
Andrew Gross1#; Asrar Alahmadi2,3#; Nikhil Ramaiya4; Afshin Dowlati2; Tithi Biswas1*
1 Department of Radiation Oncology, University Hospitals Cleveland Medical Center, Cleveland, Ohio, USA.
2 Division of Hematology and Oncology, University Hospitals Cleveland Medical Center, Cleveland, Ohio, USA.
3 Division of Medical Oncology, Ohio State University Comprehensive Cancer Center, Columbus, Ohio, USA.
4 Department of Diagnostic Radiology, University Hospitals Cleveland Medical Center, Cleveland, Ohio, USA.
*Corresponding Author: Tithi Biswas
University Hospitals Cleveland Medical Center, Cleveland, Ohio, Department of Radiation Oncology, 11100
Euclid Avenue, Cleveland Ohio, 44106, USA.
Email: tithi.biswas@uhhospitals.org
Received : Sep 14, 2021
Accepted : Oct 22, 2021
Published : Oct 29, 2021
Archived : www.jcimcr.org
Copyright : © Biswas T (2021).
Abstract
Immunotherapy has become part of the standard of care in the treatment of locally advanced non-small cell lung cancer. However, immunotherapy is associated with immune-related pneumonitis and radiation-related adverse effects. Pulmonary-related toxicity after definitive chemoradiotherapy can be challenging to distinguish from disease progression, especially in the setting of additional immunotherapy after radiation.
Our patient is a 61-year-old male that was diagnosed with stage IIIA lung adenocarcinoma of the right upper lobe that underwent treatment with concurrent chemoradiation and adjuvant durvalumab. He was found to have fevers, shortness of breath, generalized body aches and dry cough. His influenza test was positive for Influenza A. On imaging, there was significant hypermetabolic enlargement of multiple lymph node stations underwent bronchoscopy with biopsies of the right upper lobe, station 4R and 7 lymph node. Pathology of the right upper lobe biopsy showed fragments of bronchial epithelium with rare atypical cells present. Pathology of the station 7 lymph node showed small non-necrotizing granulomas, and station 4R showed rare atypical cells, consistent with squamous metaplasia. The patient was started on high dose prednisone for treatment of immune related pneumonitis and continue follow up in clinic. His symptoms continued to improve continued interval improvement seen on serial imaging in the right upper lobe soft tissue changes within the field of prior radiation in addition to improvement in the mediastinal and hilar lymphadenopathy, consistent with immunotherapy related Sarcoidlike granulomatous reactions.
Patients treated with chemoradiation and adjuvant immunotherapy for NSCLC have unique presentations of symptoms which can be mistaken for disease progression. The interpretation of imaging of the thorax such as CT or PET/CT from these symptoms can be complicated in patients treated with immune checkpoint inhibitors therapy after radiation with acute viral infectious respiratory diseases such as influenza. The noted appearance of new lung abnormalities in patients treated with chemo-radiotherapy and immunotherapy raises the concern of disease progression or pulmonary toxicity from treatment. Clinicians should be aware of these potential pulmonary immune-related adverse events or pseudoprogression, and a multidisciplinary team must be utilized to ensure appropriate treatment and evaluation of these complex patients.
Keywords: Non-small cell lung cancer; Immunotherapy; Pulmonary immune related adverse events; Radiation therapy.
Abbreviations: AKI: Acute kidney injury; CBC: Complete blood count; cGy: Centigrey; GGOs: Ground-glass opacities; ICI: Immune checkpoint inhibitor; irAE: Immune-related adverse events; NSCLC: Non-small cell lung cancer; PCR: Polymerase chain reaction; PDL-1: Programmed death-ligand 1; PET-CT: Positron Emission Tomography–Computed Tomography; RRP: Radiation recall pneumonitis; WBC: White blood cell.
Citation: Gross A, Alahmadi A, Ramaiya N, Dowlati A, Biswas T. Case report of three distinctive pulmonary toxicities related to durvalumab (PD-L1 inhibitor) consolidation therapy in locally advanced non-small cell lung cancer. J Clin Images Med Case Rep. 2021; 2(5): 1390.
Introduction
Immunotherapy has become part of the standard of care in the treatment of metastatic and locally advanced non-small cell lung cancer (NSCLC). The PACIFIC trial established durvalumab, an Immune Checkpoint Inhibitor (ICI), after chemoradiotherapy as the preferred agent in advanced-stage non-metastatic NSCLC, showing superior survival in the treatment group and a higher reported incidence of pneumonitis related to immunotherapy and radiation in both the control and treatment groups over previously reported studies [1-3]. Pulmonary-related toxicity after definitive chemoradiotherapy can be difficult to distinguish from disease progression, especially in the setting of additional immunotherapy after radiation. Though several reports have described a sarcoidlike granulomatous reaction in response to ICI therapy, there are currently few reports describing multiple pulmonary immune-related adverse events (irAE) within a single individual. We report a unique case of NSCLC with three distinctive pulmonary toxicities that mimic disease progression, highlighting the diagnostic challenges of pulmonary toxicities in stage III NSCLC.
Case presentation
A 61-year-old male was diagnosed with stage IIIA (cT4pN2cM0) lung adenocarcinoma of the right upper lobe in January 2019 by positive biopsy of a station 4R lymph node on endoscopic bronchial ultrasound, and underwent concurrent chemoradiation which he completed without significant toxicity or course complication. His most recent staging CT chest scan showed disease in remission while on consolidative durvalumab (Figure 1A). He was undergoing consolidative durvalumab immunotherapy (in his sixth month of a one year planned treatment) when he presented with a 2–3-day history of fever, shortness of breath, generalized body aches, and dry cough. In the emergency department, the patient showed no distress with vitals of normal oxygen saturation of 95% on room air, heart rate of 109, respiratory rate of 18, temperature of 36.7 Celsius (98.0 Fahrenheit), and blood pressure of 134/84. A physical examination showed wheezing throughout all lung fields, most prominently in the upper right. The rest of the physical examination was normal. Chest x-ray showed a suprahilar mass in the right upper lobe with patchy opacification. CT chest with angiography and pulmonary embolism protocol showed a significant enlargement of the lymph nodes of the bilateral axillae, the mediastinum, and the left hilum. Additionally it showed a new large mass-like opacity in the partially collapsed right upper lobe, extensive consolidation throughout the peripheral right lung, tree-in-bud opacity throughout the right middle and right lower lobes, and evidence of radiation recall pneumonitis in the right upper lobe. These findings were concerning for active progressive malignancy and post obstructive pneumonia (Figure 1B). Complete blood count (CBC) with differential showed a white blood cell (WBC) count of 4.4 x 109 cells/L, Hemoglobin 12.3 g/dL (L), and Platelet 336 X 109 cells/L. Complete metabolic profile showed an Acute Kidney Injury (AKI), Creatinine 1.37 mg/dL (H), compared to his baseline 1.01 mg/dL. Due to patient complaints of myalgia, fever, and shortness of breath, he was evaluated for influenza A/B with PCR.
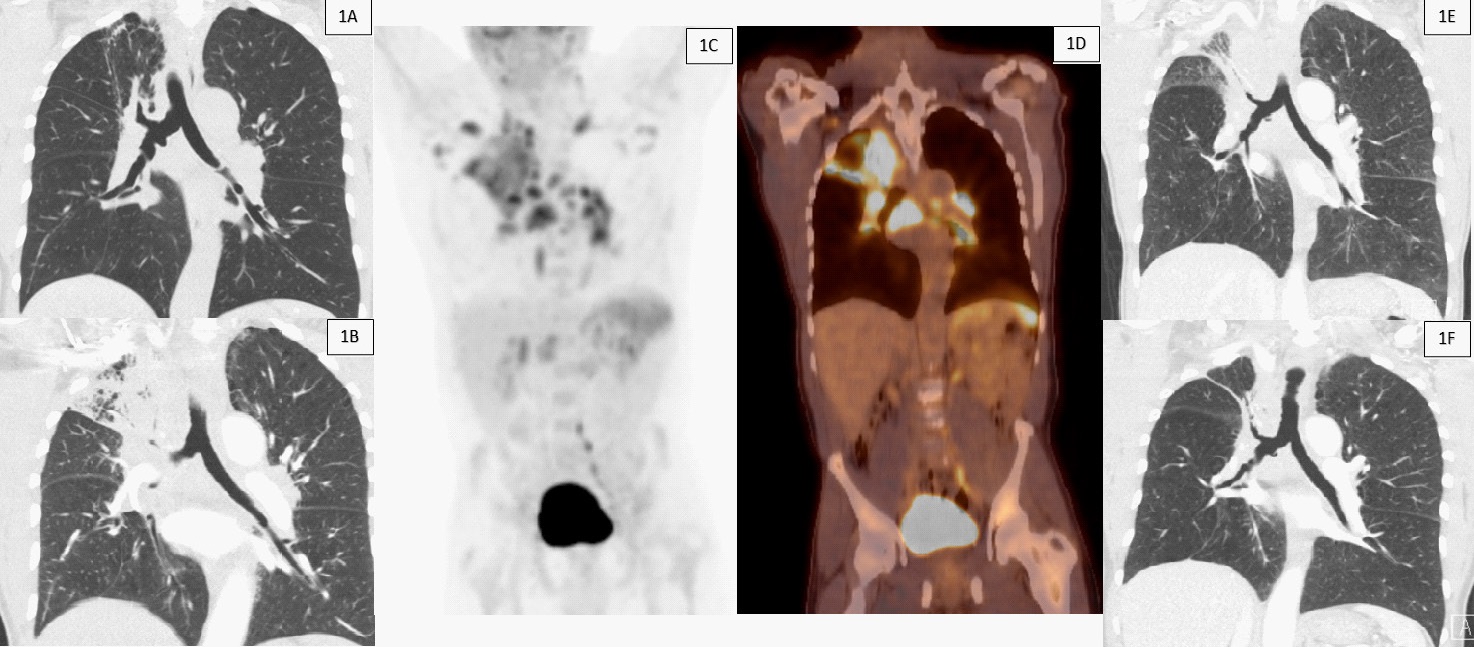
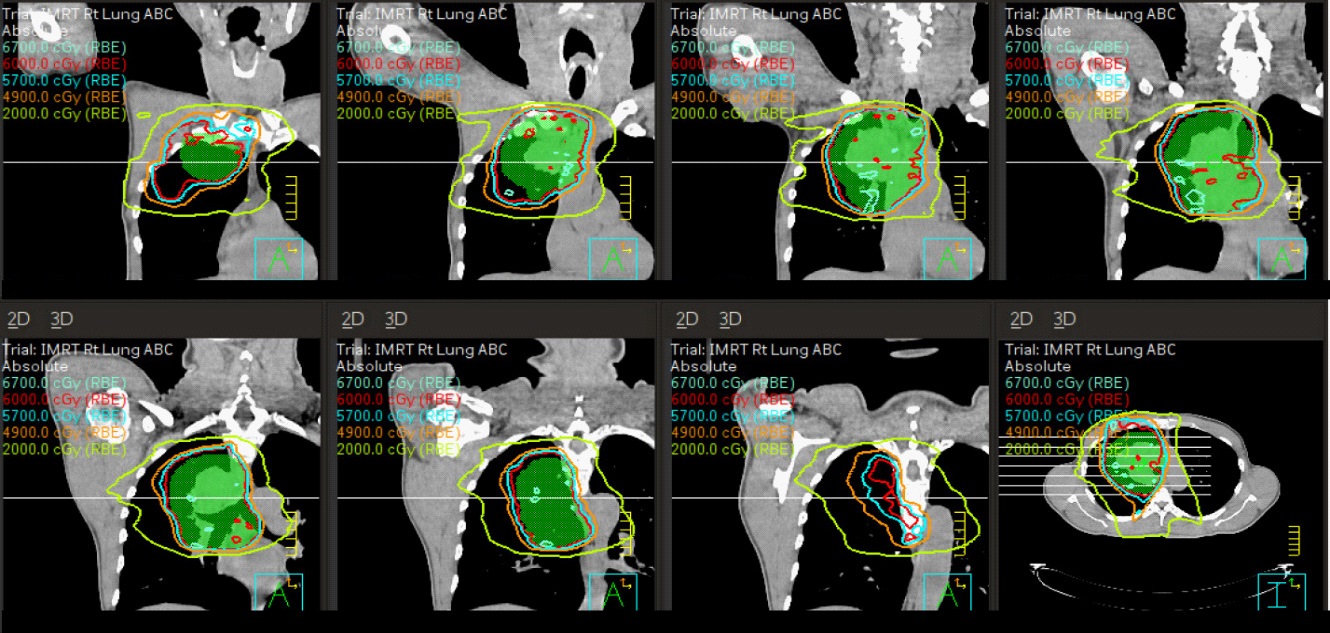
The patient completed concurrent chemotherapy with cisplatin and pemetrexed and radiation of 6000 cGy in 30 fractions to the right upper lobe, mediastinum and right paratracheal lymph node chain approximately nine months prior to presentation (Figure 2). In contrast to the favorable response seen on his last CT chest imaging one month prior to presentation, current imaging showed significant interval enlargement of multiple lymph nodes treated in the radiation field and new enlarging lymph nodes outside the radiation field in the axilla (Figure 1B). The results of the patient’s influenza PCR returned positive for Influenza A and negative for Influenza B. While admitted to the hospital, he was started on oseltamivir, nasal cannula oxygen, intravenous fluids, and levofloxacin for potential bacterial superimposed infection of the right middle and lower lobes. PET-CT showed new, diffusely increased, intense hypermetabolic activity throughout the right upper lobe, mediastinum, neck, axilla, abdomen, pelvis, spleen, and bone marrow with the concern of cancer progression (Figures 1C and 1D). The patient underwent bronchoscopy where biopsies and aspiration of the right upper lobe, station 4R and 7 lymph nodes were done. Pathology of the right upper lobe biopsy showed fragments of bronchial epithelium with rare atypical cells present. Pathology of the station 7 lymph node showed small nonnecrotizing granulomas, and station 4R showed rare atypical cells, consistent with squamous metaplasia.
The patient clinically improved after discharge and the decision was made to hold durvalumab therapy. He continued to be on observation, and a repeat imaging showed a reduction in the size of mediastinal lymphadenopathy. However, the patient was found to have interval development of ground-glass opacities (GGOs) in the bibasilar aspect of the lungs on this follow-up CT imaging of chest, representing pneumonitis. The patient was initiated on high-dose prednisone for treatment of immune-related pneumonitis and continued to follow up in clinic. His symptoms continued to improve with interval improvement seen on serial imaging in the right upper lobe soft tissue changes within the field of prior radiation, in addition to improvement in the mediastinal and hilar lymphadenopathy (Figure 1E). This was evaluated further with more improvement in his symptoms and the findings on his most recent CT chest imaging (Figure 1F).
Discussion
The noted appearance of new lung abnormalities in patients treated with chemoradiotherapy and immunotherapy raises the concern of disease progression, pulmonary irAE, radiation recall, or infection. Pulmonary irAE are common, occurring in 3-5% of patients based on large meta-analysis of randomized trials and retrospective studies, and have a variety of clinical presentations [3]. Real-world data show a higher incidence of immune-related pulmonary toxicity of 19% in some series, which can be in line with the increased use of immunotherapy to treat NSCLC in different stages and better understand of the clinical and radiographic characteristics [4,5]. Pneumonitis can range from subclinical to severe and life-threatening. Therefore, clinical suspicion, early detection, and prompt treatment are of vital importance. However, imaging findings can be misleading and easily often confused with pseudo-progression.
Our case shows that with the use of immunotherapies, the ability to characterize irAE by imaging alone is difficult due to imaging differential including other causes such as infections, inflammation or disease progression. Our patient developed multiple pulmonary irAE. Despite having normal CT scans a month before presentation, his scans showed interval enlargement of the main tumor site, enlarging mediastinal and hilar lymphadenopathy, and evidence of radiation recall pneumonitis. Biopsy for evaluation of new lesions developing on immunotherapy helped guide the diagnosis of sarcoidosis as an irAE. His biopsy showed non-necrotizing granulomas in the subcarinal lymph node on his most recent bronchoscopy. Sarcoidlike granulomatous reactions have been reported in melanoma and NSCLC patients undergoing immunotherapy with both PDL-1 and CTLA-4 inhibitor [5-7]. Asymptomatic in most cases, it can be mistaken for disease recurrence or progression that can affect patient management. Functional imaging like PET-CT scan has a limited role in solving this dilemma, with limitations in distinguishing sarcoidosis from pseudo-progression or disease recurrence. To guide the decision making, a biopsy of new lesions developing on immunotherapy should be considered [8].
Another finding in our patient scans is immunotherapyrelated radiation recall. Radiation recall pneumonitis (RRP) is a known but poorly understood phenomenon involving prior radiated tissues responding with inflammation 6-9 months post radiation within the radiation field when exposed to a systemic pharmacological agent. One hypothesis is that anti-tumor agents trigger a remembered response in surviving cells that had undergone prior radiation [9]. This phenomenon has been reported in studies involving post-radiation chemotherapy or targeted molecular agents [10,11]. However, radiation recall has rarely been reported in the immunotherapy setting [12]. RRP has a common feature among patients where confluent ground-glass opacities are located in relation to prior radiation fields. CT chest imaging on admission to the hospital showed right upper lobe mass-like consolidation corresponding to the PET avid regions seen in the location of the prior right upper lobe malignancy, consistent with RRP.
Lastly, our patient developed a classical grade 2, asymptomatic, immune-related pneumonitis with ground-glass appearance in a subsequent scan outside of radiation field, along with improvement in his mediastinal and hilar lymphadenopathy after holding the treatment for one month. He responded to high-dose steroids in addition to holding his immunotherapy. On the subsequent scan, his pneumonitis also improved. Unlike other types of irAE that show favorable association with disease response, pneumonitis correlates with poor prognosis, emphasizing the importance of appropriate and timely diagnosis and treatment [4,13].
Conclusion
As ICI became the standard of care for patients undergoing concurrent chemoradiotherapy for non-metastatic advanced NSCLC, clinicians should be aware of these potential pulmonary irAEs or pseudo-progression. The differential for these findings is wide and not always well understood or reported. Our patient developed the classical picture of sarcoid-like granulomatous reaction, immune-related pneumonitis, and RRP related to immunotherapy. In the case of new lung lesions and findings suggestive of disease progression, a multidisciplinary team and additional workup, including bronchoscopy and biopsy, should be utilized.
Declarations
Ethics statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013). We were unable to obtain written informed consent from the patient, as such, we removed all patient-specific identifiable information and images from the manuscript to protect the patient’s identity.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Disclaimers: The authors have no disclaimers in regard to the manuscript publication.
Authors' contributions: All authors aided in writing and approving the final manuscript.
Conflicts of interest: All authors have completed the ICMJE uniform disclosure form. The authors have no conflicts of interest to declare for the manuscript publication.
Acknowledgements: We would like to acknowledge all the great providers at University Hospitals Cleveland Medical Center and the quality patient-driven care they provide.
References
- Antonia SJ, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N Engl J Med. 2018; 379: 2342-50.
- Khunger M, Jain P, Rakshit S, Pasupuleti V, Hernandez AV, Stevenson J, et al. Safety and Efficacy of PD-1/PD-L1 Inhibitors in Treatment-Naive and Chemotherapy-Refractory Patients With Non-Small-Cell Lung Cancer: A Systematic Review and MetaAnalysis. Clin Lung Cancer. 2018; 19: e335-e48.
- Khunger M, Rakshit S, Pasupuleti V, Hernandez AV, Mazzone P, et al. Incidence of Pneumonitis With Use of Programmed Death 1 and Programmed Death-Ligand 1 Inhibitors in Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Trials. Chest. 2017; 152: 271-81.
- Suresh K, Voong KR, Shankar B, Forde PM, Ettinger DS, et al. Pneumonitis in Non-Small Cell Lung Cancer Patients Receiving Immune Checkpoint Immunotherapy: Incidence and Risk Factors. J Thorac Oncol. 2018; 13: 1930-9.
- Nishino M, Ramaiya NH, Awad MM, Sholl LM, Maattala JA, et al. PD-1 Inhibitor-Related Pneumonitis in Advanced Cancer Patients: Radiographic Patterns and Clinical Course. Clin Cancer Res. 2016; 22: 6051-60.
- Berthod G, Lazor R, Letovanec I, Romano E, Noirez L, Mazza Stalder J, et al. Pulmonary sarcoid-like granulomatosis induced by ipilimumab. J Clin Oncol. 2012; 30: e156-9.
- Nishino M, Sholl LM, Awad MM, Hatabu H, Armand P, et al. Sarcoid-Like Granulomatosis of the Lung Related to ImmuneCheckpoint Inhibitors: Distinct Clinical and Imaging Features of a Unique Immune-Related Adverse Event. Cancer Immunol Res. 2018; 6: 630-5.
- Lainez S, Tissot C, Cottier M, Vergnon JM. EBUS-TBNA Can Distinguish Sarcoid-Like Side Effect of Nivolumab Treatment from Tumor Progression in Non-Small Cell Lung Cancer. Respiration. 2017; 94: 518-21.
- Azria D, Magne N, Zouhair A, Castadot P, Culine S, Ychou M, et al. Radiation recall: a well recognized but neglected phenomenon. Cancer Treat Rev. 2005; 31: 555-70.
- Ding X, Ji W, Li J, Zhang X, Wang L. Radiation recall pneumonitis induced by chemotherapy after thoracic radiotherapy for lung cancer. Radiat Oncol. 2011; 6: 24.
- Togashi Y, Masago K, Mishima M, Fukudo M, Inui K. A case of radiation recall pneumonitis induced by erlotinib, which can be related to high plasma concentration. J Thorac Oncol. 2010; 5: 924-5.
- Chen Y, Huang Z, Xing L, Meng X, Yu J. Radiation Recall Pneumonitis Induced by Anti-PD-1 Blockade: A Case Report and Review of the Literature. Front Oncol. 2020; 10: 561.
- Fukihara J, Sakamoto K, Koyama J, Ito T, Iwano S, et al. Prognostic Impact and Risk Factors of Immune-Related Pneumonitis in Patients With Non-Small-Cell Lung Cancer Who Received Programmed Death 1 Inhibitors. Clin Lung Cancer. 2019; 20: 442-50 e4.