
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
The effect of tranexamic acid on blood loss in non-urgent trauma patients undergoing major orthopaedic surgery: A retrospective cohort study
Vasileia Nyktari1*; Helen Diamantaki2; Georgios Stefanakis2; Emmanouela Koutoulaki2; Periklis Vasilos2; Athanasios Alegakis1; Ioannis Sperelakis3; Alexandra Papaioannou1
1 Faculty of Medicine, University of Crete, Heraklion, Crete, Greece.
2 Department of Anaesthesiology, University Hospital of Heraklion, Crete, Greece.
3 Department of Trauma and Orthopedic Surgery, University Hospital of Heraklion, Crete, Greece.
*Corresponding Author: Vasileia Nyktari
University of Crete School of Sciences, Faculty of
Medicine, 71003, 17 Lyktou Street, 71307, Heraklion,
Crete, Greece.
Email: vnyktari@gmail.com
Received : Sep 23, 2021
Accepted : Oct 26, 2021
Published : Nov 02, 2021
Archived : www.jcimcr.org
Copyright : © Nyktari V (2021).
Abstract
Objectives: This study aims to clarify the role of prophylactic TXA on blood loss and transfusion requirements in a subgroup of trauma patients undergoing major orthopaedic surgery on a non-urgent basis.
Study design: This is a retrospective cohort study
Setting: Tertiary University Hospital of Crete (2017-2018)
Patients/participants: Polytrauma patients who underwent delayed major orthopaedic surgery
Main outcome measurement: Significant haemorrhage occurrence in relation to TXA administration. In a subgroup of patients Rotational Thromboelastometry (ROTEM) was used to reveal their haemostatic profile prior to TXA administration.
Methods: Data from anaesthetic and ICU records were analyzed regarding age, sex, body mass index, ASA physical status, Injury Severity Score, Caprini Score, intraoperative blood loss, number of packed red blood cells units transfused, volume of crystalloids administered, operation duration, preoperative and postoperative haemoglobin values, and days from hospital admission to surgery. ROTEM analysis in a subgroup of patients revealed their haemostatic profile prior to TXA administration.
Results: Twenty five out of 46 patients received prophylactic TXA treatment. After adjustment for confounding factors, the odds ratio for the composite endpoint for prophylactic TXA (n=25) vs no TXA (n=21) was 1.27 (95% confidence interval, CI 0.39-4.16). Propensity matched analysis confirmed the absence of a difference between patients with and without TXA. In all patients analyzed with ROTEM normal or hypercoagulable status was revealed.
Conclusions: In trauma patients undergoing major orthopaedic surgery more than 12 hours after the initial injury, TXA has no effect on blood loss and transfusion requirements.
Keywords: tranexamic acid; blood loss; transfusion; orthopaedic trauma surgery; spine surgery; pelvis surgery; significant bleeding in orthopaedic surgery
Citation: Nyktari V, Diamantaki H, Stefanakis G, Koutoulaki E, Vasilos P, et al. The effect of tranexamic acid on blood loss in non-urgent trauma patients undergoing major orthopaedic surgery: A retrospective cohort study. J Clin Images Med Case Rep. 2021; 2(6): 1394.
Introduction
Major haemorrhage during orthopaedic surgery is a cause of perioperative morbidity and mortality [1]. Tranexamic Acid (TXA), a lysine derivative, exerts its action by competitively occupying the lysine binding site of plasminogen, thereby blocking interaction with fibrin and subsequent clot breakdown [2]. TXA reduces perioperative blood transfusion in elective and emergency surgery [3,4], including elective orthopaedic procedures [5,6].
When considering administering TXA the main questions to be answered are which patients will benefit, when is the best time and whether blind or goal-directed administration should be preferred.
Even though CRASH-2 trial showed a survival benefit after traumatic haemorrhage, TXA’s efficacy in trauma was challenged by thereafter studies and Cole et al suggested TXA only in severely injured, shocked trauma patients [7-9].
Trauma patients are prone to thrombotic events, with DVT rates approaching 60%, supporting the reluctance to use TXA in orthopaedic trauma patients [10]. However, it has been shown that orthopaedic trauma patients have a 0.4%–7.5% increased risk of fatal pulmonary embolism compared to patients undergoing arthroplasty [11]. Furthermore, Cole et al found that Venous Thromboembolism (VTE) was more common in more severely shocked patients who received TXA, with a fourfold increase in thromboembolic events in this group [9].
Another unresolved issue is the best time to administer TXA. CRASH-2 showed reduced haemorrhage mortality when TXA was administered within 3 hours of injury [7,8]. TXA increased the risk of mortality when administered after 3 hours [7,8,12]. The time-dependent effectiveness of TXA in trauma patients was recently confirmed in a cell-based model [13,14].
Whether blind or goal directed TXA administration is justified in trauma patients undergoing delayed surgery is another unanswered question. The pathophysiology of Traumatic Induced Coagulopathy (TIC) is not yet elucidated. Dysregulated fibrinolysis is one of many hemostatic abnormalities in the bleeding trauma patient [15]. Patients with normal levels of fibrinolysis have the lowest mortality [16,17], while hyperfibrinolysis or fibrinolysis inhibition are associated with increased mortality [17].
The aim of this retrospective study was to investigate whether the prophylactic TXA administration in trauma patients undergoing orthopaedic surgery after 12 hours from initial injury was associated with less blood loss and transfusion rates. The impact of Rotational Thromboelastometry (ROTEM) in clarifying the hemostatic profile of patients and its contribution on the decision about TXA administration was also studied.
Materials and methods
Design and study population
A retrospective cohort study among trauma patients who underwent non-emergency major orthopaedic surgery (>12 hours from admission) was performed. The study was approved by the Ethical Committee and the institutional review board of the University Hospital of Heraklion (Approval number, 304/9/24-7-2019). Because of the retrospective design of the study, the need to obtain informed consent was waived by the ethics committee.
Data were collected from medical notes of trauma patients admitted to the University Hospital of Heraklion during oneyear period (January 1st, 2017, to January 1st, 2018). Trauma patients >18 years old who underwent major orthopaedic surgery >12 hours from admission to the Emergency Department (ED) were included in the study. Data from anaesthetic charts and intensive care unit records were analyzed regarding age, sex, weight, height, Body Mass Index (BMI), ASA physical status, Injury Severity Score (ISS), Caprini Score, intraoperative blood loss, number of packed red blood cells (pRBC) units transfused, volume of crystalloids administered, duration of operation, preoperative and postoperative Haemoglobin (Hb) values and days from hospital admission to surgery. Blood loss was measured by weighing gauzes and the use of a collector bag and suction system in the operating theatre. The design of the study did not allow information on possible side effects of TXA treatment.
Surgery was defined as “Urgent” if the patient’s vital signs were stable, but the surgical problem could deteriorate significantly if left untreated for >24 hours. Otherwise, the surgical problem was considered non-critical, and the patient was admitted and scheduled for surgery within the following 15 days. Patients with severe trauma were transferred to ICU after being resuscitated in the ED for stabilization before surgery. Major orthopaedic surgery included pelvic reconstruction for pelvic and acetabular fractures, spine reconstruction for fractures and dislocations and operations for hip and femoral fractures [18].
Since there is no universal definition of critical intraoperative haemorrhage, haemorrhage was defined as “significant” when >2 pRBCs were transfused in a 2-hour period. The risk of venous thromboembolism was assessed using the Caprini risk score and the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) Surgical Risk score [19,20]. The effect of tranexamic acid was compared between patients who received TXA early prior to surgical incision (TXA group) and patients who did not receive TXA (control group).
The primary outcomes were intraoperative blood loss and amount of transfused blood units (pRBCs). The following parameters were pre-defined as possible confounders of the association of tranexamic acid administration and primary outcomes: patient’s age, weight, height, BMI, ASA physical status, Injury Severity Score, preoperative Hb value, volume of fluids administered and duration of operation.
In a subgroup of patients rotational thromboelastometry (ROTEM, delta device; Tem Innovations GmbH, Munich, Germany) was used to define the hemostatic profile of the patient and guide the decision for tranexamic acid administration. Unlike conventional, plasma-based tests, viscoelastic assays quantify whole-blood clot formation and degradation and can identify hypercoagulability as well as fibrinolysis shutdown [21,22].
Extrinsic, fibrin based and intrinsic thromboelastometry (EXTEM, FIBTEM, INTEM) was performed on a blood sample to assess clot function. Parameters measured included clotting time (CT; the time from the start of the test to initial clot formation; normal range, 42-74 seconds), alpha angle (α; the slope of the tracing, which represents the rate of clot formation; normal range, 63-81 degrees), and maximum clot firmness (MCF; the greatest amplitude of the tracing, which illustrates clot strength; normal range, 49-71 mm). MCF in EXTEM reflects platelet-fibrin interactions, a component involved in both clot formation and degradation, and has been shown to correlate with hypercoagulability in trauma and other surgical populations [21]. Patients were classified as hypocoagulable (MCF<49 mm), normocoagulable (MCF 49-71 mm), or hypercoagulable (MCF>71 mm). Maximum clot firmness greater than 71 mm has been associated with thromboembolic events in another series [22].
The difference between the MCF and the lowest clot amplitude after MCF is reached, is defined as maximum lysis (ML, %) and is used to measure fibrinolysis [21]. In a recent study an EXTEM ML value <3.5% had the best Youden index (J = 0.19) to define fibrinolysis shutdown [23].
In this subgroup of patients with ROTEM analysed blood samples, emphasis was given on assessing which patients were hypercoagulable (MCF>71 mm) or had fibrinolysis inhibition (ML <3.5%). The patient’s hemostatic profile integrated with anesthesiologist’s clinical judgement guided the decision for TXA prophylactic administration.
Statistical analysis
Descriptive statistics were used to report patient characteristics and outcomes. Logistic and linear regression models were used to assess the relationship between outcomes and early vs no tranexamic acid administration. The multivariate models were adjusted for measured pre-defined confounders based on observed differences between the comparison groups.
The discrete variables were expressed in terms of frequency and % frequency while continuous ones with mean and standard deviation. The independent samples t-test was used to find mean differences between two discrete groups. Chi-square test (χ2 ) was used to test the correlation of two discrete variables. All analyses and graphical representation of the data were done with Microsft Excel and IBM SPSS statistics 24.0 software. The statistic acceptance threshold was set at α=0.05.
We observed that patients with a blood loss >900 ml were more likely to be transfused and assuming that a decrease of 30% is significant, it was estimated that 15 patients per group with a 5% confidence level and a 30% confidence level [1-β] were required.
Results
Patient characteristics
This cohort study included 46 trauma patients who underwent major orthopaedic surgery: spine reconstruction (n=25), pelvic surgery (n=12) and hip or femoral fracture operations (n=9). The study group comprised of 25 patients who received a bolus of tranexamic acid prior to the surgical incision (TXA group). There were no differences in demographic characteristics among patients in control and TXA groups (Table 1). Most patients (60.8%) were classified as ASA 3 or 4 status. More than half of ASA 3 or 4 patients received TXA compared to only 38.8% of ASA 1 or 2 patients.
Table 1: Patients’ characteristics in the control and study (TXA) group.
|
Control group |
TXA group |
|
||
n |
mean±SD |
n |
mean±SD |
p (t-test) |
|
Age (yr) |
21 |
52.6±16.1 |
25 |
49.4±20.2 |
0.564 |
Weight (kg) |
20 |
82.9±16.9 |
24 |
78.4±23.6 |
0.482 |
Height (cm) |
20 |
1.7±0.1 |
24 |
1.7±0.1 |
0.320 |
BMI (kg/m2) |
20 |
29.3±5.5 |
24 |
26.2±5.4 |
0.064 |
Caprini Score |
20 |
14.7±6.3 |
25 |
15.4±5.6 |
0.695 |
Blood loss (mls) |
10 |
615.0±627.2 |
17 |
926.5±697.8 |
0.257 |
Pre-operative Hb (g/dl) |
17 |
11.5±2.2 |
25 |
12.4±2.1 |
0.219 |
Post-operative Hb (g/dl) |
14 |
9.6±1.0 |
19 |
10.4±1.6 |
0.122 |
Days from ED admission to surgery |
21 |
7.4±6.5 |
25 |
5.8±4.2 |
0.325 |
ISS score |
15 |
20.6±8.5 |
20 |
23.1±10.2 |
0.446 |
Duration of operation (hours) |
21 |
3.64±1.96 |
25 |
4±1.62 |
0.508 |
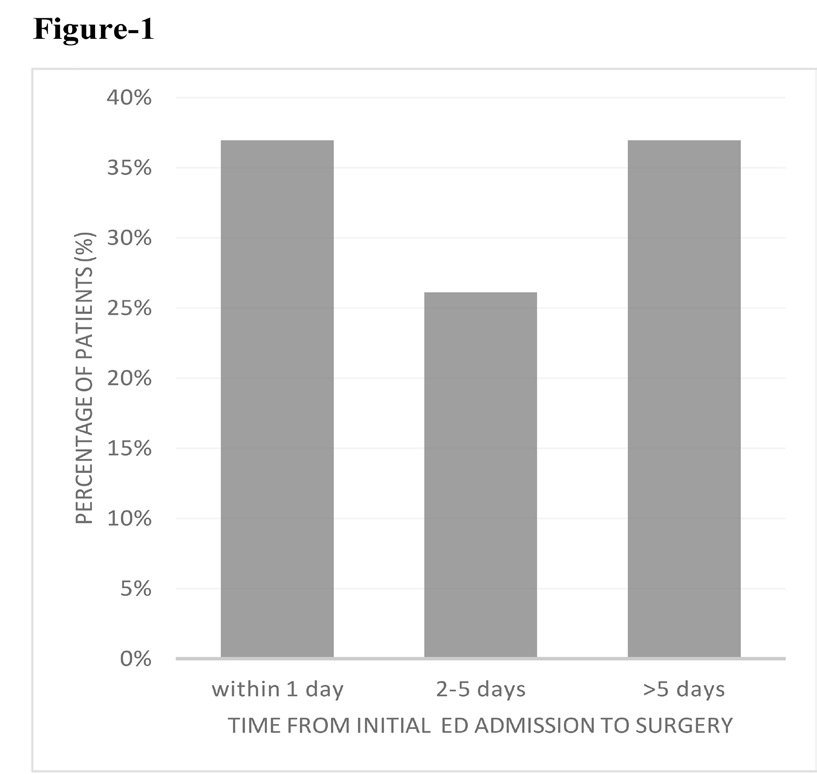
No differences were noted between the 2 groups regarding ISS score, pre-operative Hb, post-operative Hb, time delay from admission to surgery, duration of operation, volume of crystalloids administered and Caprini score (Table 1). The most common co-injuries were pneumothorax, chest wall fractures and lung contusions. Most patients (84.7%) had high venous thromboembolism risk (4-10%) as calculated by the ACS NSQIP Surgical Risk score, while 91% of patients and Caprini Score >5. Approximately one third of patients were operated after 12 hours (36.95%), whereas a delay >10 days was observed in 23.91%. Figure 1 shows the percentage of patients and the time delay from initial ED admission to surgery.
Significant haemorrhage and patient characteristics
Significant haemorrhage was defined as the need to transfuse ≥2 pRBCs over a period of 2 hours. Nineteen patients (41%) had significant haemorrhage in the operating theatre. No association with age, weight, height or BMI was observed (Table 2). The amount of blood loss was significantly higher in the group with significant haemorrhage (1291 ± 679.9 mls vs 426.7 ± 365.4 mls, p=0.001). No difference was noted on preoperative Hb value between groups, whereas a slightly lower postoperative Hb was observed in the group of patients with significant haemorrhage requiring transfusion (Table 2). Significant haemorrhage was not associated with time delay from initial admission to surgery or duration of operation (Table 2). Patients with significant haemorrhage had a higher Caprini score (18.7 ± 4.3 vs 12.7 ± 5.6, p=0.001). Trauma severity, assessed by ISS score, was not associated with the presence of significant haemorrhage (Table 2).
Table 2: Patients with and without significant hemorrhage. Association with characteristics of the patient and the procedure.
Significant Haemorrhage |
|
||||
No |
Yes |
|
|||
|
n |
mean ± SD |
n |
mean ± SD |
p (t-test) |
Age |
27 |
50.5±17.7 |
19 |
51.4±19.7 |
0.872 |
Weight (Kg) |
26 |
76.6±19.5 |
18 |
85.9±21.7 |
0.142 |
Height (cm) |
26 |
1.7±0.1 |
18 |
1.7±0.1 |
0.148 |
BMI (Kg/m2) |
26 |
26.9±5.2 |
18 |
28.6±6.2 |
0.346 |
Caprini Score |
27 |
12.7±5.6 |
18 |
18.7±4.3 |
<0.001 |
Blood loss |
15 |
426.7±365.4 |
12 |
1291.7±679.9 |
<0.001 |
Preoperative Hb (g/dl) |
26 |
12.5±2.0 |
16 |
11.4±2.3 |
0.110 |
Postoperative Hb (g/dl) |
21 |
10.5±1.3 |
12 |
9.2±1.2 |
0.008 |
|
Significant Haemorrhage |
|
|||
No |
Yes |
|
|||
|
n |
mean ± SD |
n |
mean ± SD |
p (t-test) |
Days after trauma |
27 |
5.9±5.0 |
19 |
7.6±5.9 |
0.303 |
ISS score |
19 |
21.1±8.5 |
16 |
23.2±10.6 |
0.513 |
Duration of operation (hours) |
27 |
3.42±1.86 |
18 |
4.47±1.5 |
0.053 |
Tranexamic acid administration and primary outcome
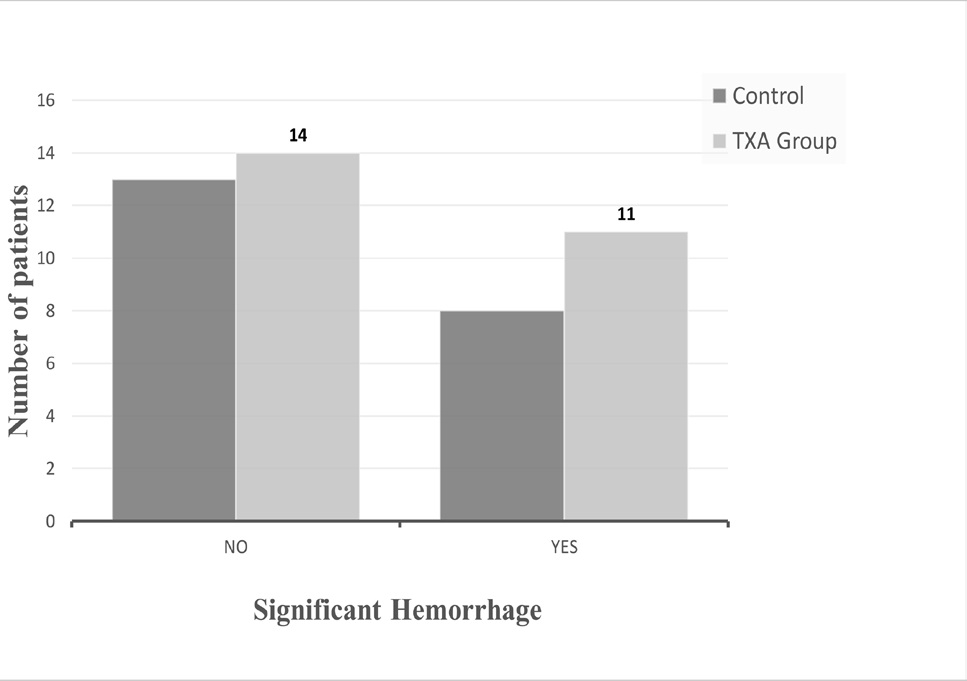
The dose of TXA ranged from 1 to 2 g and was administered as a bolus prior to surgical incision. Significant haemorrhage did not differ between TXA and control groups (p=0.685, Figure 2). Furthermore, no significant statistical difference was observed in blood loss among patients, as the mean total blood loss was 926.5 ml ± 697.8 ml in the TXA group and 615ml±627.2ml in the control group (p=0.182). Transfusion was required in 56.5% of all patients. Most of the transfused patients (38.4%) underwent spine surgery, followed by pelvic reconstruction surgery (34.6%) and hip-femoral surgery (26.9%). Most transfused patients (76.92%) required ≥ 2 pRBCs while the amount of pRBCs transfused ranged from 1 to 10 (average number 3 units of pRBCs).
Use of rotational thromboelastometry (ROTEM) in a subgroup of patients
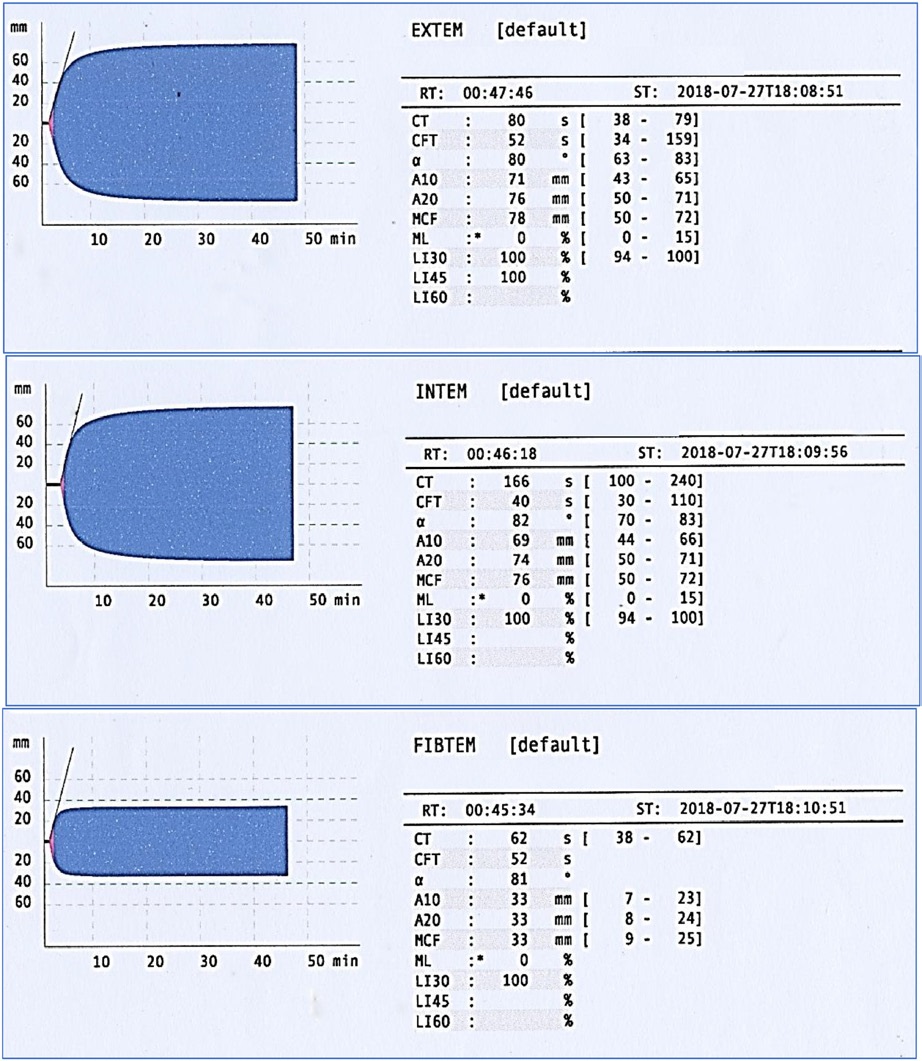
In 14 out of the 46 patients, ROTEM was used to demonstrate the coagulation phenotype and guide the decision for TXA administration. ROTEM revealed either hypercoagulable state or normal coagulation and TXA was not administered in any of these patients. Eight patients (57%) were hypercoagulable, as defined by Maximum Clot Firmness (MCF) >71 mm in EXTEM [21], while six patients (42.85%) had a normal coagulation temogram (Table 3). The temograms (EXTEM, FIBTEM, INTEM) of a patient operated within 24 hours are presented in Figure 3, revealing a hypercoagulable state. Despite the high hemorrhagic risk of the procedure, TXA was not administered prophylactically.
None of the 14 patients had hyperfibrinolysis as defined by Maximal Lysis (ML) >15% 60 min after clot formation. 50% of the patients analyzed with ROTEM demonstrated a phenotype of fibrinolysis inhibition (shutdown) as defined by EXTEM ML< 3.5% [23]. ASA physical status 3 or 4 was associated with fibrinolysis shut down (p=0.03).
No demographic parameter was associated with hypercoagulability according to EXTEM MCF (Table 3). In patients with hypercoagulability the mean delay time from initial ED admission to surgery was 5 days (5.1 ± 4.9 days).
Discussion
The present study examined the effectiveness of TXA in trauma patients undergoing major orthopaedic surgery 12 hours after initial ED admission. Our findings showed that TXA did not affect blood loss and transfusion requirements. In the subgroup of patients assessed with ROTEM, fibrinolysis shutdown and hypercoagulability were the most prevalent phenotypes.
The present study has several limitations. First, it was a nonrandomized, retrospective, cohort, single-center study, so there may have been selection and/or surveillance bias. Second, a major consideration was the definition of significant intraoperative haemorrhage. In the literature, massive haemorrhage is defined either as blood loss exceeding Circulating Blood Volume (CBV) within 24-hours, or blood loss of 50% of CBV within a 3-hour period, or blood loss >150 ml/min, or blood loss that necessitates plasma and platelet transfusion [25]. However, critical haemorrhage can occur even when these criteria are not met. Factors other than volume or speed of blood loss can threaten surgical patients, such as co-morbidities, preceding anemia and delay of blood transfusion [26]. Therefore, haemorrhage severity was assessed as means of transfusion intensity. Significant haemorrhage occurred when administration ≥ 2 pRBCs within 2 hours of operation was required.
Α third challenge was detection of “occult” hyperfibrinolysis, where pathologic active fibrinolysis at a local injury level fails to extend into the circulation remaining undetectable by VHAs [10]. Raza et al compared results from ROTEM with other fibrinolysis assay methods and found that the majority of patients with ongoing fibrinolysis were not identified by ROTEM [26]. The literature supporting TXA-guided therapy based on hyperfibrinolysis measure by VHAs remains unclear [10]. In the future, combination of VHAs with multichannel microfluidic ex vivo recapitulation studies will reflect more accurately the hemostatic derangements in trauma [27].
Lastly, the retrospective nature of this study prevents indepth understanding of the incidence of venous thrombotic events. Better knowledge of any association of TXA with VTE requires a prospective study.
TXA has been widely advertised as saving lives after traumatic haemorrhage in CRASH-2, MATTERs, and PED-TRAX trials [7,10,28,29]. CRASH-2 trial showed a survival benefit but no reduction in blood loss and transfusion rates [7]. Thereafter non-randomized controlled trials provided conflicting evidence regarding the efficacy of TXA on a broad spectrum of trauma patients who showed a benefit in CRASH-2 study [8,9,10,30].
Traumatic Induced Coagulopathy (TIC) is now regarded a complex endogenous response to tissue injury and hypoperfusion. The underlying mechanisms include from early critical deficits of fibrinogen and other clotting factors to endotheliopathy and excessive fibrinolysis [31-34]. Τhe balance between clot formation and degradation, that normally serves to stop haemorrhage while preventing microvascular thrombosis, is disrupted. As the balance is restored, patients can shift in a continuum between hypo- and hyper-coagulable states over time. Furthermore, in orthopaedic surgery it has been shown that endothelial cells synthesize and release plasminogen activator inhibitor-1 (PAI-1) in response to an unknown plasma mediator [10].
While the discussion around TXA primarily focuses on hyperfibrinolysis, in fact, the predominant pattern seen with viscoelastic hemostatic assays (VHAs) in severely injured trauma patients is fibrinolysis shutdown [17]. It must be noted that acquired fibrinolysis resistance between 4 and 12 hours after injury is not associated with increased morbidity and represents a physiologic response to injury and recovery from hemorrhagic shock [10]. The transition to pathologic acquired fibrinolysis resistance becomes evident at 24 hours after injury, presumably due to persistently elevated PAI-1. TXA administration at that point prolongs fibrinolysis shutdown, which is a risk factor for delayed mortality [10]. Furthermore, TXA’s role in patients with physiological fibrinolysis remains unclear [10]. For all these reasons, exogenous inhibition of fibrinolysis in severe trauma requires careful selection of patients since inappropriate administration may adversely affect survival [10,15]. In our study, 50% of patients analyzed with ROTEM had fibrinolysis shut down and TXA was not administered.
Data from the subgroup analyses of CRASH-2 patients showed that the TXA’s effect depends significantly on the time interval between injury and initiation of treatment [8]. Accumulating data on the time dependency of TXA’s effect are reflected on the recently published European guidelines, where it is recommended that TXA should be administered to trauma patients bleeding or at risk of significant haemorrhage as soon as possible and within 3 h after injury (Grade 1A) [34].
There are no data to support TXA’s administration in trauma patients beyond 3h from injury, as its effect on bleeding, immunity and inflammation is not clear [35]. In order to examine TXA’s effect beyond 3 hours, true orthopaedic emergencies that require immediate surgery such as acute compartment syndromes and fractures or dislocations associated with vascular injury were excluded from our study.
In our study, most patients were characterized by an increased VTE risk. The transition from hypo- to hyper-coagulability after physiologic stress was first recognized in 1914, but the timing of this change remains poorly understood [36,37]. Only a few studies have explained the dynamic nature of coagulation status as patients progress through their hospital course, and they have focused on trends in hypercoagulability [37-39].
In a recent study, serial TEMs were used to characterize the transition from hypo- to hyper-coagulability and determine the time to resolution of TIC [21]. It was shown that TIC largely resolves within 24 hours, after which hypercoagulability becomes increasingly more prevalent [21]. The proportion of hypercoagulable patients increased after 24 hours escalating significantly to 53% at 120 hours. By using the same criteria to define normal and hyper-coagulability, we found a non-significant difference towards hypercoagulability when the delay time from injury to operation increased (5.1±4.9 days in hypercoagulable vs 1±0 days in normal coagulation patients, p=0.06).
Controversy exists on safety of TXA in patients at higher VTE risk, since most studies are either underpowered or exclude high-risk patients.
Conclusion
In conclusion, the findings of the present study demonstrate that the use of TXA in trauma patients undergoing delayed major orthopaedic surgery does not affect significant haemorrhage or transfusion rates.
Declarations
Acknowledgements: Helen Askitopoulou, Emeritus Professor of Anesthesiology, Faculty of Medicine, University of Crete, Greece.
We thank prof. Askitopoulou for the continuous support in every phase of the study and critical reviewing of the manuscript.
Funding Statement: “Support was provided solely from institutional and/or departmental sources.”
Conflicts of Interest: “The authors declare no competing interests.”
References
- Gausden EB, Qudsi R, Boone MD, et al. Tranexamic Acid in Orthopaedic Trauma Surgery: A Meta-Analysis. J Orthop Trauma. 2017; 31: 513-519.
- Tengborn L, Blomback M, Berntorp E. Tranexamic acid–an old drug still going strong and making a revival. Thromb Res. 2015; 135: 231-42.
- Ker K, Edwards P, Perel P, et al. Effect of tranexamic acid on surgical bleeding: systematic review and cumulative meta-analysis. BMJ. 2012.
- Kozek-Langenecker SA, Ahmed AB, Afshari A, et al. Management of severe perioperative bleeding: guidelines from the European Society of Anaesthesiology. First update 2016. Eur J Anaesthesiol. 2017; 34: 332-395.
- Henry DA, Carless PA, Moxey AJ, et al. Anti-fibrinolytic use for minimizing perioperative allogeneic blood transfusion. Cochrane Database Syst Rev. 2011; CD001886.
- Yang B, Li H, Wang D, et al. Systematic review and meta-analysis of perioperative intravenous tranexamic acid use in spinal surgery. PLoS One. 2013; 8: e55436.
- CRASH-2 trial collaborators, Shakur H, Roberts I, Bautista R, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomized, placebo-controlled trial. Lancet. 2010; 376: 23-32.
- CRASH-2 collaborators, Roberts I, Shakur H, Afolabi A, et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. Lancet. 2011; 377: 1096-101,1101. e1-2.
- Cole E, Davenport R, Willett K, et al. Tranexamic acid use in severely injured civilian patients and the effects on outcomes: a prospective cohort study. Ann Surg. 2015; 261: 390-4.
- Moore HB, Moore EE, Neal MD, et al. Fibrinolysis Shutdown in Trauma: Historical Review and Clinical Implications. Anesth Analg. 2019; 129: 762-773.
- Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008; 133: 381S-453S.
- Dobson GP, Doma K and Letson HL. Clinical relevance of a p value: Does tranexamic acid save lives after trauma or postpartum haemorrhage? J Trauma Acute Care Surg. 2018; 84: 532-536.
- Diebel ME, Martin JV, Liberati DM, et al. The temporal response and mechanism of action of tranexamic acid in endothelial glycocalyx degradation. J Trauma Acute Care Surg. 2018; 84: 75-80.
- Diebel LN, Martin JV, Liberati DM. Early tranexamic acid administration ameliorates the endotheliopathy of trauma and shock in an in vitro model. J Trauma Acute Care Surg. 2017; 82: 1080- 1086.
- Walsh M, Shreve J, Thomas S, et al. Fibrinolysis in trauma: “myth,” “reality,” or “something in between”. Semin Thromb Hemost. 2017; 43: 200-212.
- Moore HB, Moore EE, Gonzalez E, et al. Hyperfibrinolysis, physiologic fibrinolysis, and fibrinolysis shutdown: the spectrum of post injury fibrinolysis and relevance to antifibrinolytic therapy. J Trauma Acute Care Surg. 2014; 77: 811-7; discussion 817.
- Moore HB, Moore EE, Liras IN, et al. Acute fibrinolysis shutdown after injury occurs frequently and increases mortality: A multicenter evaluation of 2,540 severely injured patients. J Am Coll Surg. 2016; 222: 347-55.
- Piggott RP, Leonard M. Is there a role for antifibrinolytics in pelvic and acetabular fracture surgery? Ir J Med Sci. 2016; 185: 29- 34.
- Caprini JA, Arcelus JI, Hasty JH, et al. Clinical assessment of venous thromboembolic risk in surgical patients. Semin Thromb Hemost 1991;17 Suppl 3: 304-12.
- Bilimoria KY, Liu Y, Paruch JL, et al. Development and Evaluation of the Universal ACS NSQIP Surgical Risk Calculator: A Decision Aide and Informed Consent Tool for Patients and Surgeons. J Am Coll Surg. 2013; 217: 833-42.e1-3.
- Sumislawski JJ, Kornblith LZ, Conroy AS, et al. Dynamic coagulability after injury: Is delaying venous thromboembolism chemoprophylaxis worth the wait? J Trauma Acute Care Surg. 2018; 85: 907-914.
- Hincker A, Feit J, Sladen RN, Wagener G. Rotational thromboelastometry predicts thromboembolic complications after major non-cardiac surgery. Crit Care. 20104; 18: 549.
- Gomez-Builes JC, Acuna SA, Nascimento B, et al. Harmful or Physiologic: Diagnosing Fibrinolysis Shutdown in a Trauma Cohort with Rotational Thromboelastometry. Anesth Analg. 2018; 127: 840-849.
- Irita K. Risk and crisis management in intraoperative haemorrhage: Human factors in hemorrhagic critical events. Korean J Anesthesiol. 2011; 60: 151-60.
- Irita K, Kawashima Y, Morita K, et al. Supplemental survey in 2003 concerning life-threatening hemorrhagic events in the operating room. Masui. 2005; 54: 77-86
- Raza I, Davenport R, Rourke C, et al. The incidence and magnitude of fibrinolytic activation in trauma patients. J Thromb Haemost. 2013; 11: 307-14.
- Li R, Elmongy H, Sims C, et al. Ex vivo recapitulation of traumainduced coagulopathy and preliminary assessment of trauma patient platelet function under flow using microfluidic technology. J Trauma Acute Care Surg. 2016; 80: 440-9.
- Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter MJ. Military Application of Tranexamic Acid in Trauma Emergency Resuscitation (MATTERs) Study. Arch Surg. 2012; 147: 113-9.
- Eckert MJ, Wertin TM, Tyner SD, et al. Tranexamic acid administration to pediatric trauma patients in a combat setting: the pediatric trauma and tranexamic acid study (PED-TRAX). J Trauma Acute Care Surg. 2014; 77: 852-8; discussion 858.
- Sumislawski S, McCollester J, Thomas S, et al. CRASH-2 study of tranexamic acid to treat bleeding in trauma patients: a controversy fueled by science and social media. J Blood Transfus. 2015; 2015: 874920.
- Ostrowski SR, Henriksen HH, Stensballe J, et al. Sympathoadrenal activation and endotheliopathy are drivers of hypocoagulability and hyperfibrinolysis in trauma: A prospective observational study of 404 severely injured patients. J Trauma Acute Care Surg. 2017; 82: 293-301.
- Johansson PI, Stensballe J, Rasmussen LS, et al. A high admission syndecan-1 level, a marker of endothelial glycocalyx degradation, is associated with inflammation, protein C depletion, fibrinolysis, and increased mortality in trauma patients. Ann Surg. 2011; 254: 194-200.
- Chin TL, Moore EE, Moore HB, et al. A principal component analysis of postinjury viscoelastic assays: clotting factor depletion versus fibrinolysis. Surgery. 2014; 156: 570-7.
- Spahn DR, Bouillon B, Cerny V, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition Crit Care. 2019; 23: 98.
- Godier A, Roberts I, Hunt BJ. Tranexamic acid: less bleeding and less thrombosis? Crit Care. 2012; 16: 135.
- Cannon WB, Gray H. Factors affecting the coagulation time of blood. Am J Physiol. 1914; 34: 232–242
- Chapman BC, Moore EE, Barnett C, et al. Hypercoagulability following blunt solid abdominal organ injury: when to initiate anticoagulation. Am J Surg. 2013; 206: 917-22.
- Schreiber MA, Differding J, Thorborg P, et al. Hypercoagulability is most prevalent early after injury and in female patients. J Trauma 2005; 58: 475–481
- Park MS, Martini WZ, Dubick MA, et al. Thromboelastography as a better indicator of hypercoagulable state after injury than prothrombin time or activated partial thromboplastin time. J Trauma. 2009; 67: 266-75.