
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Lofgren’s syndrome: A case report and review of the literature
Dong Bingzi1,2; Zhao Qian1; Wang Mei1; Li Jinfeng1; Wang Lina1; Du Chunhua1*
1 Department of Respiratory and Critical Care Medicine, the Affiliated Hospital of Qingdao University, Qingdao, 266003, China.
2 Department of Endocrinology and Metabolism, the Affiliated Hospital of Qingdao University, Qingdao, 266003, China.
*Corresponding Author: Du Chunhua
Department of Respiratory and Critical Care Medicine,
the Affiliated Hospital of Qingdao University, 16 Jiangsu
Road, Qingdao, 266003, China.
Email: duchunhua99@sina.com
Received : Sep 25, 2021
Accepted : Oct 26, 2021
Published : Nov 02, 2021
Archived : www.jcimcr.org
Copyright : © Chunhua D (2021).
Abstract
Lofgren’s syndrome is a variant of acute-onset sarcoidosis, characterized as Hilar Lymphadenopathy (HL), Erythema Nodosum (EN) and bilateral arthritis or arthralgia, with elevated serum Angiotensin Converting Enzyme (ACE) and calcium level. It is relatively common in Caucasians, but rarely reported in Asian countries. We reported a 72-year old Chinese female with HL, acute onset EN, multiple arthritis and arthralgia, and achieved remission with prednisolone treatment. We summarized reported cases in European and Asia countries, and investigated the characteristics of etiology, genetics, prognosis and therapeutic strategy variants due to different ethnicities. Almost all the patients showed HL, and half of them exhibited classical triad. ACE, the biomarker of Lofgren’s syndrome, elevated in more than half of the European cases, but only 30% in Asian patients. NASID is considered as the first choice of Lofgren’s syndrome, and glucocorticoid may be necessary in severe cases. One quarter of the cases from European countries need steroid therapy. However, the proportion is much higher (64.3%) to achieve symptomatic relief. Considering Lofgren’s syndrome is rare and less recognized from sarcoidosis in Asian patients, further investigation is needed to achieve clinical experience.
Keywords: lofgren’s syndrome; lymphadenopathy; erythema nodosum; arthritis; sarcoidosis.
Citation: Bingzi D, Qian Z, Mei W, Jinfeng L, Lina W. Lofgren’s syndrome: A case report and review of the literature. J Clin Images Med Case Rep. 2021; 2(6): 1395.
Introduction
Sarcoidosis is a chronic systemic granulomatous disorder, characterized as the non-caseating granulomatous inflammation [1]. Lung is the most frequently involved organ (>90%) [2], even progressive fibrosis and interstitial lung disease could occur. Lofgren’s syndrome is considered as a variant of acute sarcoidosis, with the clinical features of Hilar Lymphadenopathy (HL), Erythema Nodosum (EN) and bilateral arthritis or arthralgia, with or without fever. Sven Halvar Lofgren firstly described it in 1953 [3]. Serum Angiotensin Converting Enzyme (ACE) and calcium are usually elevated. Lofgren’s syndrome is relatively common in Caucasian and America black populations, but very rare in East Asian such as Japan or South Korea [4,5]. To our knowledge, this is the first report of Chinese patient with Lofgren’s syndrome.
The etiology and pathogenesis is still uncertain. Recent studies demonstrate that HLA (human leukocyte antigen)-DRB1*03 may be associated with Lofgren’s syndrome [6]. The outcome of Lofgren’s syndrome is favorable, and most patients fully recovered with non-steroidal anti-inflammatory drugs (NASIDs) administration within two years [7]. However, steroid therapy is necessary to severe cases. The therapy strategy of Lofgren’s syndrome remains controversial.
In this case, we reported a 72-year old Chinese female, exhibiting HL, acute onset EN, multiple arthritis and arthralgia. After treatment with NASID, the symptom relief was not obvious, then prednisolone was administrated to achieve remission rapidly
Case presentation
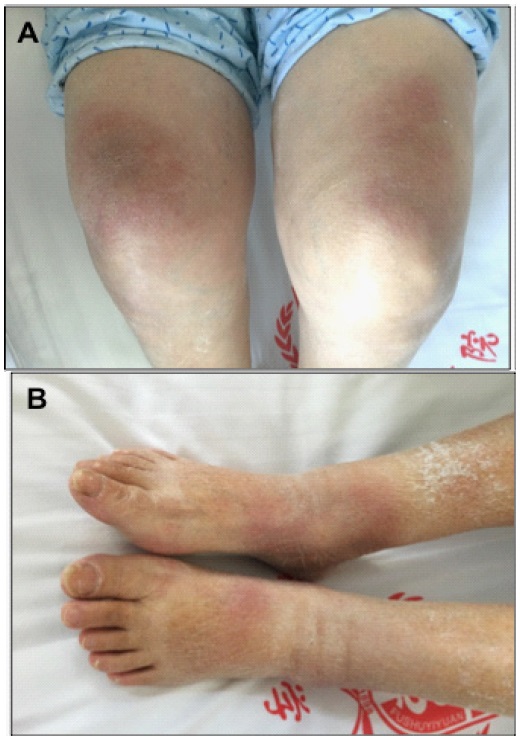
A 72-year old female patient was hospitalized because the hilar and mediastinal lymph nodes enlargement was observed in her health examination within two months. She had no symptoms such as fever, cough, hemoptysis, night sweats, chest pain and tightness, shortness of breath or dyspnea. One week ago, after footbath using traditional Chinese herbal medicine, she exhibited acute onset of symmetric EN on the lower extremities, with itchy and painful skin lesions. She also complained about pain and swelling of keen, ankle, elbow and shoulder joints. She denied usage of other special drugs, or history of contact with chemical toxins. No neurological, cardiac or ophthalmological abnormalities were observed. Physical examination revealed that symmetric EN and mild edema on lower extremities (Figure 1), and swelling of joints without motion range limitation.
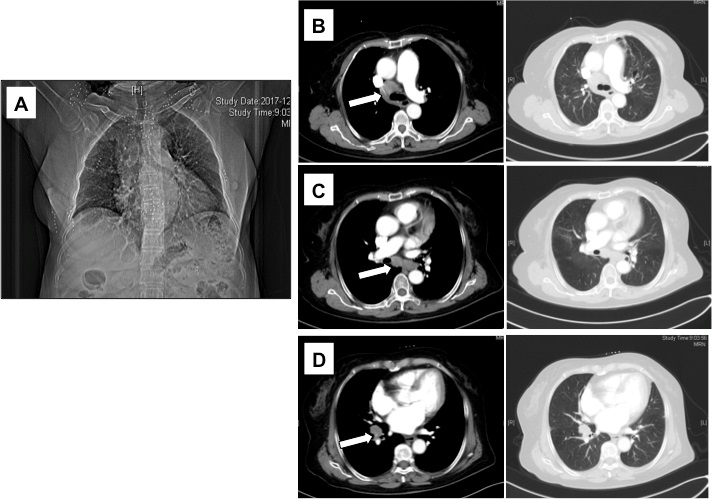
Laboratory examination revealed that C-reactive protein (CRP, 41.79mg/L) and erythrocyte sedimentation rate (ESR, 68 mm/h) were significantly elevated. Serum calcium was 2.4 mmol/L (normal 2.11-2.52 mmol/L), and urinary calcium (uCa/ uCr 0.74, normal<0.2) was increased, with normal parathyroid hormone (PTH) level (22.43 pg/mL, normal range 15-65 pg/mL). Anti-Nuclear Antibody (ANA) was positive with titer 1:320, and anti-cyclic Citrullinated Peptide (CCP) antibody, Rheumatoid Factor (RF) was negative. Blood routine test, uric acid, coagulation, renal and liver function tests were not remarkable (Table 1). Tumor biomarkers including Neuron-Specific Enolase (NSE), pro-Gastrin Releasing Peptide (pro-GRP), Cancer Antigen 125 (CA125), Carcinoembryonic Antigen (CEA), squamous cell carcinoma antigen (SCC) were negative. Enhanced Computerized
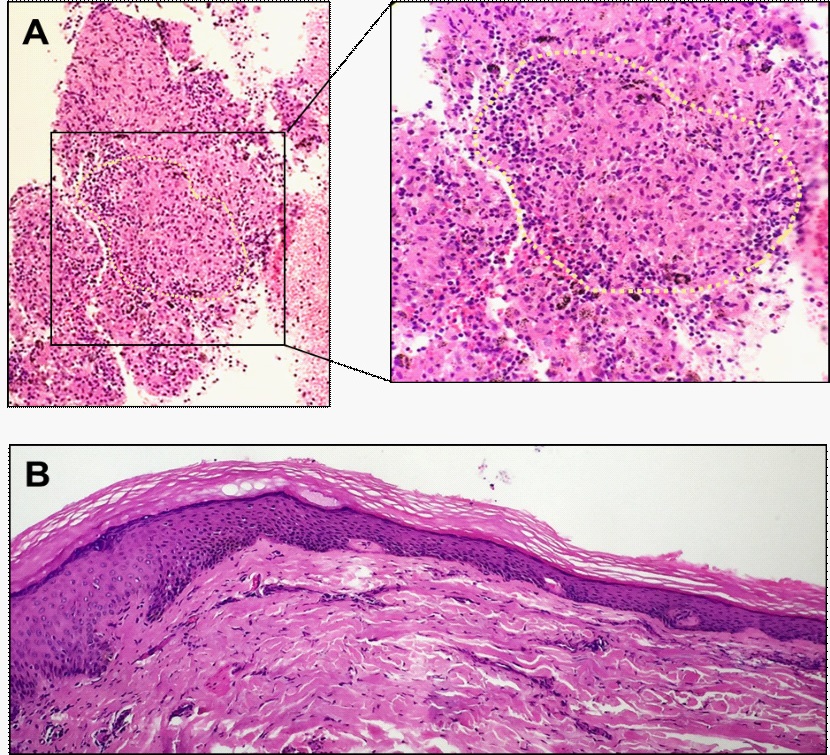
Tomography (CT) scan showed hilar and mediastinal lymphadenopathy (Figure 2). We observed soft tissue swelling and arthroedema by magnetic resonance imaging (MRI) of knee joints. Endobronchialultrasound guided transbronchial needle aspiration (EBUS-TBNA) was performed, and pathologic result of hilar lymph nodes revealed non-caseating granulomatosis, with lymphocytes and neutrophil infiltration (Figure 3A). Skin biopsy showed chronic inflammation with squamous epithelialization (Figure 3B).

In this case, the patient was diagnosed as Lofgren’s syndrome according to the symptoms and signs, including HL, acute onset EN, polyarthritis and multi arthralgia. After treatment with loxoprofen (NASID) for ten days, the symptoms of EN and arthralgia relief were not obvious, then oral administration of prednisolone was initiated. The arthralgia and EN recovered within five days, and CRP was normalized.
Discussion
Lofgren’s symptom, the acute type of sarcoidosis with EN, HL and arthritis or arthralgia, is relatively more common among young women from Northern European countries. However, it is rarely reported in Eastern Asia, especially in Japan [5] and South Korea. To our knowledge, this is the first report of Lofgren’s syndrome from China, though more patients might be underdiagnosed, or haven’t been particularly recognized from sarcoidosis. The diagnosis of Lofgren’s syndrome depends on the classic clinical features, and histologic confirmation is not necessary in typical cases [2].
Table 1: Clinical characteristics of the patient.
|
|
Patient |
Normal range |
- Blood routine test |
|
|
|
White blood cells |
*10^9/L |
7.54 |
3.5-9.5 |
Neutrophils |
% |
68.7 |
40-75 |
Lymphocytes |
% |
23.5 |
20-50 |
Eosinophils |
% |
0.5 |
0.4-0.8 |
Hemoglobin (Hb) |
g/L |
118 |
115-150 |
Platelet (PLT) |
*10^9/L |
275 |
125-350 |
- Biochemistry |
|
|
|
Sodium (Na) |
mmol/L |
142 |
137-147 |
Potassium (K) |
mmol/L |
4.06 |
3.5-5.5 |
Calcium |
mmol/L |
2.4 |
|
Creatine (Cr) |
umol/L |
42 |
31-132 |
Urinary Ca excretion (uCa/uCr) |
|
0.74 |
<0.2 |
Parathyroid hormone (PTH) |
pg/mL |
22.43 |
15-65 |
Uric acid (UA) |
umol/L |
234 |
89.2-339 |
- Autoimmune parameters |
|
|
|
Anti-nuclear antibody (ANA) |
|
Positive 1:320 |
Negative |
Rheumatoid factor (RF) |
U/mL |
11.4 |
Negative<20 |
C-reactive protein (CRP) |
mg/L |
41.68 |
<5 |
Erythrocyte sedimentation rate (ESR) |
mm/h |
68 |
<15 |
In this study, we reviewed the literatures reported in different regions (Table 2), and summarized available data to investigate the clinical characteristics of Lofgren’s syndrome in different ethnicities.
Table 2: Review of literatures and summary analysis of the available data.
|
Asia |
(%) |
Ref. |
European |
(%) |
Ref. |
Patient number |
14 |
|
This case, 10-13 |
741 |
|
4-9 |
Female |
12/14 |
85.7% |
456/741 |
61.5% |
4-9 |
|
Male |
2/14 |
14.3% |
285/741 |
38.5% |
4-9 |
|
Age (years old) |
37.8 |
(Range 23-72) |
36.9 |
(Range 21-79) |
4-9 |
|
Classical triad (HL, EN, arthritis or arthralgia) |
9/14 |
64.3% |
123/254 |
48.4% |
4,5,7,9 |
|
Chest radiography (stage I-II) |
14/14 |
100% |
734/741 |
99.1% |
4-9 |
|
Fever |
8/14 |
57.1% |
19/29 |
65.5% |
4,9 |
|
ACE elevation |
4/13 |
30.8% |
120/222 |
54.1% |
6,9 |
|
Prednisolone |
9/14 |
64.3% |
117/457 |
25.6% |
4,5,8,9 |
|
Fellow-up (recurrence rate) |
All recovered |
55*/607 |
9.1% |
4,5,6,8 |
||
Review of literatures
The epidemiology, etiology, genetics, and prognosis of Lofgren’s syndrome vary due to different ethnicities. It occurs more frequently in female patients, 12/14 (85.7%) in Asian countries (1 from China, this case, 1 from South Korea and 12 from Japan). The rate seems to be higher compared to the reports about European populations (average 61.5%, range 30.5%-84.4%). The mean age of onset in Asian patients is 37.8±14 (range 23-72), similar to that of Caucasians. The typical triad including HL, EN and arthritis/arthralgia were observed in around half of the Lofgren’s syndrome patients (64.3% in Asian and 48.4% in European populations) [8]. Almost all the patients showed lymphadenopathy, and classified into stage I-II according to the chest radiological abnormalities. (Stage I: HL only, stage II: HL with pulmonary infiltrates, stage III: pulmonary infiltrates without BHL, and stage IV: fibrosis). ACE is regarded as biomarker and important clue for the diagnosis of Lofgren’s syndrome. However, the elevation of ACE is reported in 30.7% Asian patients, less frequent compared to 54.1% in European populations (Table 2).
Clinical characteristics
Patients with Lofgren’s syndrome usually present characteristic triad (HL, EN and polyarthritis). However, other signs and symptoms also occur, such as fever, dyspnea, hepatomegaly and splenomegaly. Central nervous system [9] and renal involvement [10] are rarely reported.
The EN occurs in several conditions including sarcoidosis, tuberculosis, beta-hemolytic streptococci infection, drug usage, and even idiopathic [11], which makes the differential diagnosis to be important. The history of footbath using traditional Chinese herbal medicine (Sophora flavescens, rhodiola, angelica, Salviae Miltiorrhizae) made it difficult to differ from skin infection or autoimmune system activation. Whether the Chinese herbal medicine usage is a trigger of exaggerated inflammatory response, leading to the EN during the disease course is uncertain. However, the typical EN induced by Lofgren’s syndrome is acute-onset, symmetric, mainly on the lower-extremities, and combined with multiple arthritis or arthralgia. The female patients tended to exhibit EN than males, especially older women (>45 years old) [11]. EN, arthralgia and arthritis are commonly observed in various connective tissue diseases, Rheumatoid Arthritis (RA), vasculitis or Tuberculosis (TB). Arthritis and arthralgia in Lofgren’s syndrome are usually symmetrical, and ankles are the most frequently effected. However, radiography usually shows normal image except soft tissue swelling. Elevated serum calcium and ACE are diagnostic clues. Serum ACE increased in 41% sarcoidosis and 15% Lofgren’s syndrome patients [12]. Patients with elevated ACE levels tend to have a relatively more persistent disease course, thus, it could be considered as a monitor of the disease activity [13].
Prognosis
Lofgren’s syndrome is regarded as a self-limiting disease, more than 90% patients achieve manifestations relief within two years, and with a lower rate of recurrence than sarcoidosis [14]. In our investigation of literatures, about 9% Caucasians had recurrence within 2-5 years follow-up. All the patients from China, South Korea and Japan a non-resolving disease course, though the long-term follow-up is necessary.
The predisposing factors and prognosis of Lofgren’s syndrome may be associated with races, sex [8], cytokines [15], and gene polymorphism [16]. It was reported that HLA-DRB1*03 may be associated with Lofgren’s syndrome and its prognosis. All the HLA-DRB1*03-positive patient had a resolving disease within 2 years, but half of the negative patients still had a nonresolving course, even with the oral steroids treatment [6,17]. However, HLA-DR3 was not obtained in any of the Japanese cases of Lofgren’s syndrome. HLA-DR12 was present 55.6% cases suggesting that HLA-DR12 might play an important role in the pathogenesis of Japanese patients [18]. In addition, significantly increased frequency of C-C chemokine receptor 2 (CCR2) polymorphism haplotype2 was detected (74%, compared to control 38%, p<0.0001) in Lofgren’s syndrome [19,20].
Treatment
It is helpful to evaluate prognosis and guide therapeutic strategy. Usually, steroid is not required for the early stages sarcoidosis, while extra-pulmonary complication is considered to be the indication of steroid administration. NASIDs are recommended as the first choice of Lofgren’s syndrome. However, Lofgren’s syndrome may be regarded as the extra-pulmonary manifestations of sarcoidosis, which leading to the excessive usage of glucocorticoid.
The therapeutic strategy of Lofgren’s syndrome remains controversial. Mana et al. reported that NASID administration relief most symptoms of Lofgren’s syndrome, and less than 10% patients required steroid to attain remission [21]. However, unlike Caucasians, the treatment using NASIDs seems not obvious in our case and the review of Japanese and Korean patients. Therapy of glucocorticoid usually obtains remission of symptoms rapidly. The proportion of steroid administration is higher than that in European countries (64.3% in Asian v.s 25.6% in European populations). The different therapeutic effects may be associated with racial differences. Considering about the side effect of long-term administration with steroid, to determine the appropriate therapeutic strategy is important. More clinical cases of Asian patients are needed for further investigation.
Conclusion
We reported a 72-year old Chinese female patient with Lofgren’s syndrome, exhibiting HL, acute onset EN, multiple arthritis and arthralgia. She achieved remission rapidly with prednisolone treatment. The etiology, genetics, prognosis and therapeutic strategy of Lofgren’s syndrome vary due to different ethnicities. Lofgren’s syndrome is rarely reported, especially in Asian population. Thus, further investigation is needed to achieve clinical experience.
Declarations
Acknowledgements: The authors thank the patient for her participation.
Disclosure statement: This work was supported by Shandong Higher Education Young Science and Technology Support Program (2020KJL005) to Bingzi Dong. All authors have no conflict of interest related to this work.
References
- Thomas KW, Hunninghake GW. Sarcoidosis J. JAMA. 2003; 289: 3300.
- Ungprasert P, Carmona EM, Utz JP, et al. Epidemiology of Sarcoidosis 1946-2013: A Population-Based Study J. Mayo Clin Proc. 2016; 91: 183-8.
- Rizzato G, Tinelli C. Unusual Presentation of Sarcoidosis J. Respiration. 2005; 72: 3.
- Newman LS, Rose CS, Maier LA. Sarcoidosis J. N Engl J Med. 1997; 336: 1224.
- Morimoto T, Azuma A, Abe S, et al. Epidemiology of Sarcoidosis in Japan J. Eur Respir J. 2008; 31: 372.
- Baughman RP, Lower EE, du Bois RM. Sarcoidosis J. Lancet. 2003; 361.
- Ubogy Z, Persellin RH. Suppression of Erythema Nodosun by Indomethacin J. Acta Derm Venereol. 1982; 62: 265.
- Grunewald J, Eklund A. Sex-specific Manifestations of Lofgren’s Syndrome J.. Am J Respir Crit Care Med. 2007; 175: 40.
- Terushkin V, Stern BJ, Judson MA, et al. Neurosarcoidosis: Presentations and Management J. Neurologist. 2010; 16: 2.
- Mahevas M, Lescure FX, Boffa JJ, et al. Renal Sarcoidosis: Clinical, Laboretory, and Histologic Presentation and Outcome in 47 Patients J. Medicine (Baltimore). 2009; 88: 98.
- Cribier B, Caille A, Heid E. Erythema Nodosum and Associated Diseases: A Study of 129 Cases J. Int J Dermatol. 1998; 37: 667.
- Studdy PR, Bird R. Serum Angiotensin Converting Enzyme in Sarcoidosis—Its Value in Present Clinical Practice J. Ann Clin Biochem. 1989; 26: 13.
- Ungprasert P, Carmona EM, Crowson CS, rt al. Diagnostic Utility of Angiotensin-Converting Enzyme in Sarcoidosis: A PopulationBased Study J. Lung. 2016; 194: 91-5.
- ManaJ, Gomez-Vaquero C, Montero A, et al. Logren’s Syndrome Revisited: A Study of 186 patients J. Am J Med. 1999; 107: 240.
- Chen ES, Moller DR. Sarcoidosis-Scientific Progress and Clinical Challenges J. Nat Rev Rheumatol. 2011; 7; 457.
- Iannuzzi MC. Advances in the Genetics of Sarcoidosis J. Proc Am Thorac Soc. 2007; 4: 457.
- Vissser H, Vos K, Zanelli E, et al. Sarcoid Arthritis: Clinical Characteristics, Diagnostic Aspects, and Risk Factors J.. Ann Rheum Dis. 2002; 61: 499.
- Ina Y, Takada K, Yamamoto M, et al. HLA and Sarcoidosis in the Japanese J. Chest. 1989; 95: 1257.
- Rossman MD, Thompson B, Frederick M, et al. HLA-DRB1*1101: A Significant Risk Factor for Sarcoidosis in Blacks and Whites J. Am J Hum Genet. 2003; 73: 720-35.
- Mehra NK, Bovornkitti S. HLA and Sarcoidosis J. Sarcoidosis. 1988; 5: 87.
- Kobak S. Sarcoidosis: A Rheumatologist’s Perspective J. Ther Adv Musculoskelet Dis. 2015; 7: 196-205.