Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Endotracheal tube mal-insertion via Zenker’s diverticulum to trachea
Yan-Cheng Chen1; Yi-Hsun Chen1,2*
1 Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
2 Graduate Institute of Clinical Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
*Corresponding Author: Chen Yi-Hsun
Graduate Institute of Clinical Medicine, College of
Medicine, Kaohsiung Medical University, Kaohsiung,
Taiwan.
Email: jayshung1985@gmail.com
Received : Oct 11, 2021
Accepted : Nov 04, 2021
Published : Nov 11, 2021
Archived : www.jcimcr.org
Copyright : © Yi-Hsun C (2021).
Citation: Yi-Hsun C, Yan-Cheng C. Endotracheal tube mal-insertion via Zenker’s diverticulum to trachea. J Clin Images Med Case Rep. 2021; 2(6): 1402.
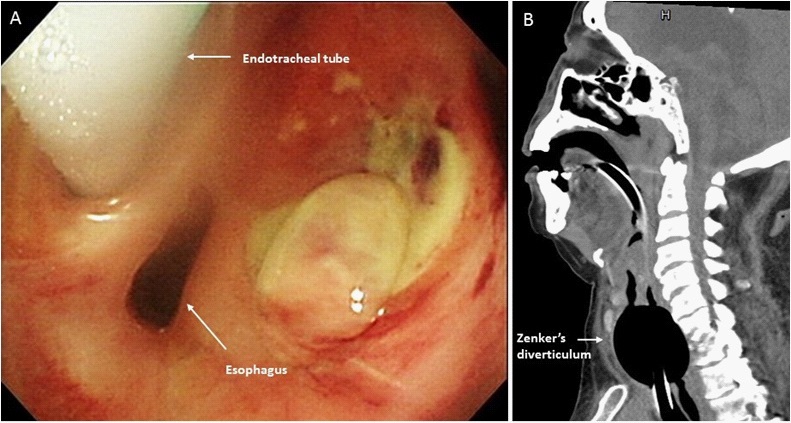
Clinical image description
An 86-year-old woman with chronic respiratory failure was under endotracheal tube insertion and mechanical ventilator support for 2 months due to previous intra-cranial hemorrhage. She presented with difficult nasogastric (NG) tube insertion after changing endotracheal tube and was transferred to our emergency room. The initial vital signs were blood pressure: 136/85 mmHg, heart rate: 100 bpm, respiratory rate: 20 cpm, body temperature: 36.5o c, and SpO2 : 100% under ventilator support, and stupor consciousness was remained as usual. The physical examination showed bilateral clear breath sound. We tried the NG tube insertion again but in vain; therefore, the esophagogastroduodenoscopy (EGD) was performed for NG tube insertion and revealed malposition of the endotracheal tube over upper esophagus and Zenker’s diverticulum with ulcerations (Panel A). Endotracheal tube was inserted to the esophagus, via the Zenker’s diverticulum, and then to the trachea. The neck CT confirmed the diagnosis (Panel B). After endotracheal tube replacement via bronchoscopy and supportive care with antibiotics treatment, the patient was discharged after admission for two weeks.