
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Anal canal epithelioid sarcoma: Case report and literature review
Cárdenas-Almaraz Bárbara V; Capdeville-Jímenez Gabriela; Molina-Botello Diego*; Pérez-Martínez Ignacio J
Department of Neurological Surgery, National Institute of Neurology and Neurosurgery “Manuel Velasco Suarez” (INNN), 3877 Insurgentes Sur Av, La Fama, Tlalpan, 14269 Mexico City, Mexico.
*Corresponding Author: Molina-Botello Diego
Department of Neurological Surgery, National Institute of Neurology and Neurosurgery “Manuel Velasco
Suarez” (INNN), 3877 Insurgentes Sur Av, La Fama,
Tlalpan, 14269 Mexico City, Mexico.
Email: diegombotello@gmail.com
Received : Oct 09, 2021
Accepted : Nov 08, 2021
Published : Nov 15, 2021
Archived : www.jcimcr.org
Copyright : © Molina-Botello D (2021).
Abstract
Soft tissue tumors account for less than 0.1% of colon and rectum malignant neoplasms. Epithelioid sarcoma is a subtype of undifferentiated soft tissue neoplasia that makes up 1% of this category; it is characterized by a slow progression, commonly affecting young male adults, with little or no response to chemotherapy and radiotherapy, leaving surgical resection their main therapeutic option to reduce recurrence. We here present the case of a 71-year-old male patient admitted for major rectorrhagia after evacuations and anal pain. During physical examination, a posterior anal sphincter induration was noted, which extended to the puborectal muscle. Anoscopy was performed where a thrombosed hemorrhoidal bundle was detected adjacent to a mass. In the later biopsy with immunohistochemistry, a proximal ulcer type, histological grade three epithelioid sarcoma was diagnosed. Subsequently, traditional abdominal perineal resection with colostomy was performed, resulting in favorable postoperative evolution and discharge after six days of the procedure.
Keywords: soft tissue tumors; epithelioid sarcoma.
Citation: Cárdenas-Almaraz BV, Capdeville-Jímenez G, Molina-Botello D, Pérez-Martínez IJ. Anal canal epithelioid sarcoma: Case report and literature review. J Clin Images Med Case Rep. 2021; 2(6): 1404.
Introduction
Anal duct cancer account for 4% of all lower gastrointestinal (GI) tract neoplasia [1]. Malignant anal lesions can be divided in two categories: those that affect the anal margin and those that comprise the anal canal [2]. Both are frequently associated with Human Papillomavirus (HPV) infections; however, in rare cases tumors can be found in the anus, such as, soft tissue tumors, which constitute less than 0.1% of colon and rectal tumors [1,3]. Within this rare heterogeneous tumors, the epithelioid sarcoma (ES) constitutes less than 1% of all soft-tissue sarcomas; ES is characterized by its slow growth, predominance in young male adults, the tendency to originate in extremities and its resistance to chemo and radiotherapy. There is a poorly described proximal variant, that affects the trunk, pelvis, perineum and genitalia, which comes with a worse prognosis for its lack of histological differentiation, aggressive behavior, high recurrence rate and lymphatic spread causing metastasis to the lungs [4,5]. We present the case report of a 71-year-old male with an proximal epithelioid sarcoma of the anal canal which was successfully removed.
Case report
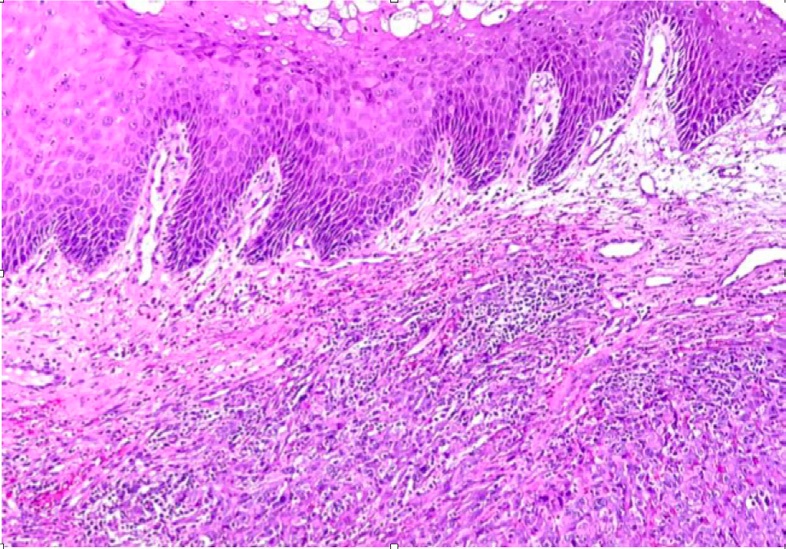
A 71-year-old male with a protruding indurated and bleeding mass in the anus, with initial diagnosis of external hemorrhoidal disease, was admitted to the emergency department of Dalinde Medical Center in Mexico City after a month of abundant rectorrhagia, clots after every evacuation, accompanied by intense anal pain. On digital rectal examination, a posterior anal sphincter induration that extended to the puborectal muscle, was noted. A subsequent anoscopy was performed, noticing a thrombosed right posterior hemorrhoidal bundle with an underlying tumor, involving the internal anal sphincter and puborectal muscle. Hemorrhoidectomy was performed and the tumor was removed; a transoperative anatomopathological exam exhibit four perianal skin biopsy fragments, the largest being of 2.1 X 1.5 X 0.7 cm and of 0.6 X 0.5 X 0.3 cm the smallest. The latter being positive for the immunohistochemical marker: cytokeratin AE1/AE3 and negative for HMB - 45, Melan-A, CD34, Desmin, ERG and INI-1, integrating the microscopic diagnosis of a proximal ulcerated epithelioid sarcoma, histologic grade 3 (NaCLF) with positive margins and tissue necrosis.
Afterwards, the patient was referred to the oncology service, performing traditional abdominal and perineal resection with left colostomy. A 33.5 cm long by 4.1 cm diameter piece was obtained containing anal margin, mesorectum, rectum and distal portion of sigmoid colon, along with 15 perirectal lymph nodes. The anatomopathology study identified the tumor in the anal canal measuring 5.5 X 4.5 cm, with an ulcerated surface, lobed and digitiform areas (Annex 2). It was also reported the infiltration of neoplasic cells from dermis to striated muscle of the anal canal with proximal, distal and radial free margins of 26.5 cm, 1.5 cm and 0.5 cm margin respectively (Annex 3). Perirectal nodes were reported with mixed hyperplasia. In the postoperative care unit, analgesics, low molecular weight heparinic (LMWH) and double antibiotic scheme was given. The patient showed a favorable evolution, presenting evacuations by colostomy on the third day; however on the fifth day, it was required a red blood cell transfusion due to severe anemia with hemoglobin 8 mg/dL. Patient was discharged on the sixth day
Diagnosis
Patients with epithelioid sarcoma display a great variety of non-specific symptoms such as: constipation, diarrhea, rectal pain, tenesmus, loss of weight and rectal bleeding. The latter, combined with its low incidence, makes this a diagnostic challenge. Therefore, imaging studies play a crucial role in the evaluation of this group of tumors [1,3,4].
Computed tomography (CT) and magnetic resonance imaging (MRI) have been proposed as equally specific and sensitive to evaluate soft tissue tumors. Thus, it has been shown that using both does not increase accuracy of the diagnosis [3].
Sigmoidoscopy and colonoscopy with biopsy are the diagnostic go to methods of choice. In addition, the entire colon should be evaluated due to the common presence of synchronous tumors [1,3]. Endoscopic rectal ultrasound is a very useful tool for inconclusive tumors (ie submucosal tumors) biopsied by colonoscopy. Finally the definitive diagnosis of these tumors must be done histopathologically, being positive for immunohistochemical epithelial and mesenchymals markers such as vimentin, cytokeratin and CD34 characteristic of epithelial sarcomas [1,3,6].
Treatment
The standard curative treatment for soft tissue tumors is surgical excision, being the local wide excision the most frequently performed [1,4,5]. Transanal excision should be reserved for tumors with benign characteristics, such as: smaller than 3 cm and located more than 8 cm from the anal margin. For lower rectum neoplasia, the minimum margin needed to preserve the anal sphincter is 2 cm, on the contrary, as presented in this case, where there was sphincter involvement per se abdominoperineal resection (APR) is of choice [1]. Variants of this surgical procedure are selected according to the lateral extension of the excision and the structures to be removed. Traditional extrasphincteric APR consists of resection of the distal colon, rectum and mesorectum, anal canal and anal margin with subsequent colostomy [8]. Follow-up is done with CT every 3-6 months in the first 2-3 years after the surgical excision; thereafter, every 6 months for 2 years and then annually.


Discussion
Anal malignant and potentially malignant lesions are rare and in most cases are associated with HPV infection [1]. For the study of anal lesions, the anus is divided into two regions: the anal margin and the anal canal. Malignant lesions of the anal margin include: squamous cell carcinoma, carcinoma of basal cells, verrucous carcinoma and Kaposi’s sarcoma, on the other hand, premalignant lesions include: Paget’s disease, Bowen’s disease and leukoplakia. Malignant lesions of the anal canal include: epidermoid carcinoma with its different subclassifications: squamous cell, basaloid, basosquamous, epithelioid, transitional and mucoepidermoid, melanoma, adenocarcinomas and soft tissue tumors [1,2].
Within soft tissue tumors, Sarcomas represent 1-2% of all solid neoplasms; their origin can be anywhere, however it is frequent to locate them in extremities (59%), followed by the trunk (19%), retroperitoneum (12%) and head and neck (9%), leaving 1% for other locations [1,5].
Within soft tissue sarcomas, it exists a subclassification of undifferentiated sarcomas, which have an uncertain or non definitive histological origin, so they are catalogued according to the tissue’s predominant cell morphology [7].
Epithelioid sarcoma is an histological subtype part of this heterogeneous group of soft tissue tumors and constitute 1% of it, in addition to being classified as malignant [4,6]. Just like any other sarcoma its usual location is the extremities; however, there is a proximal variant, which has a worse prognosis with higher recurrence rate and it can be distinguished by its location: in the trunk, pelvic region, perineum and genitals, in addition to having a rhabdoid cell morphology compared to the classic, with appearance of granulomatous tissue and spindleshaped cells among other histopathological characteristics [1, 4].
Both epithelioid sarcoma variants are clinically manifested as painless slow growing masses. It has been reported to affect predominantly male individuals between 23 and 40 years old, and are mostly reported to be located in the extremities. They are prone to spread via the lymphatic and show little response to chemotherapy and radiotherapy, being the only treatment radical surgical resection. They have a survival rate of 50-65% in five years [4,6].
Conclusion
Epithelioid sarcoma belongs to the heterogeneous group of soft-tissue tumor which have an extremely low prevalence. Its diagnosis and, even more, its treatment, which involves surgery with high morbimortality as abdominoperineal resection, are complicated so it is necessary to have an interdisciplinary group which ensures that the patient is given an accurate diagnosis, timely treatment and, of course, strict monitoring that gives the patient the best possible prognosis.
References
- Herrera Gómez Á, Ñamendys Silva S, Meneses García A. Manual de Oncología. 6th ed. México: McGraw-Hill; 2017.
- Beck D Timmcke A. Diagnosis of, malignant and potentially malignant anal lesions. Techniques in Gastrointestinal Endoscopy. 2004; 6(1): 17-22.
- Nassif M, Trabulsi N, Bullard-Dunn K, Nahal A, Meguerditchian A. Soft tissue tumors of the anorectum: rare, complex and misunderstood. Journal of Gastrointestinal Oncology. 2013; 4(1): 82-94.
- Santana D, Meyer M, Santos E, Andrade C, Vilela Neto P, Matoso A et al. Hemipelvectomy with laparoscopic abdominoperineal excision for epithelioid sarcoma treatment. Journal of Coloproctology. 2019.
- Wolf P, Flum D, Tanas M, Rubin B, Mann G. Epithelioid sarcoma: the University of Washington experience. The American Journal of Surgery. 2008; 196(3): 407-412.
- Armah H, Parwani A. Epithelioid Sarcoma. Archives of Pathology & Laboratory Medicine. 2009; 133(5): 814 - 819.
- Jo V, Doyle L. Refinements in Sarcoma Classification in the Current 2013 World Health Organization Classification of Tumours of Soft Tissue and Bone. Surgical Oncology Clinics of North America. 2016; 25(4): 621-643.
- Hawkins A, Albutt K, Wise P, Alavi K, Sudan R, Kaiser A et al. Abdominoperineal Resection for Rectal Cancer in the Twenty-First Century: Indications, Techniques, and Outcomes. Journal of Gastrointestinal Surgery. 2018; 22(8): 1477-1487.