
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
MIS-A associated myocardial injury: The art of diagnosis and follow-up
Bellony Nzemenoh1; Arianne C Agdamag2; Valmiki Maharaj2; Victoria Charpentier3; Kellen Albrecht2; Tamas Alexy2*
1 Department of Medicine, University of Minnesota, Minneapolis, MN 55455, USA.
2 Department of Medicine, Division of Cardiology, University of Minnesota, Minneapolis, MN 55455, USA.
3 University of Minnesota Medical School, Minneapolis, MN 55455, USA.
*Corresponding Author: Tamas Alexy
Department of Medicine, Division of Cardiology, University of Minnesota, Minneapolis, MN 55455, USA
Email: alexy001@umn.edu
Received : Oct 05, 2021
Accepted : Nov 08, 2021
Published : Nov 15, 2021
Archived : www.jcimcr.org
Copyright : © Alexy T (2021).
Abstract
Multisystem inflammatory syndrome in adults (MIS-A) is a rare but severe condition in adults with a clinical course similar to that described in children (MIS-C) following infection with the SARS-CoV-2 virus. Here we describe a case of a 21-year-old, otherwise healthy female who presented with chest pain and signs of sepsis six weeks after recovering from coronavirus disease 2019 (COVID-19). Early identification of MIS-A led to a favorable clinical course and full recovery. Given the highly variable disease presentation yet potentially deadly outcome, providers must remain vigilant to recognize and treat MIS-A early
Keywords: MIS-A; myocardial inflammation; SARS-CoV-2; COVID-19 disease.
Citation: Nzemenoh B, Agdamag AC, Maharaj V, Charpentier V, Albrecht K. MIS-A associated myocardial injury: The art of diagnosis and follow-up. J Clin Images Med Case Rep. 2021; 2(6): 1405.
Introduction
Multisystem Inflammatory Syndrome in Children (MIS-C) is a rare but severe condition that was first identified in April 2020. It develops in children under the age of 21 years approximately four weeks after contracting the SARS-CoV-2 virus (Coronavirus disease 2019; COVID-19). Isolated case reports of adults presenting with symptoms and clinical course resembling to MIS-C started to emerge subsequently. The Centers for Disease Control and Prevention (CDC) first recognized the new entity as Multisystem Inflammatory Syndrome in Adults (MIS-A) in May 2020 and developed diagnostic guidelines for healthcare providers [1]. We present a rare case of MIS-A with cardiac involvement in a young, otherwise healthy individual emphasizing the importance of early recognition, timely intervention, and the need for close follow-up to reduce the risk of devastating complications.
Case presentation
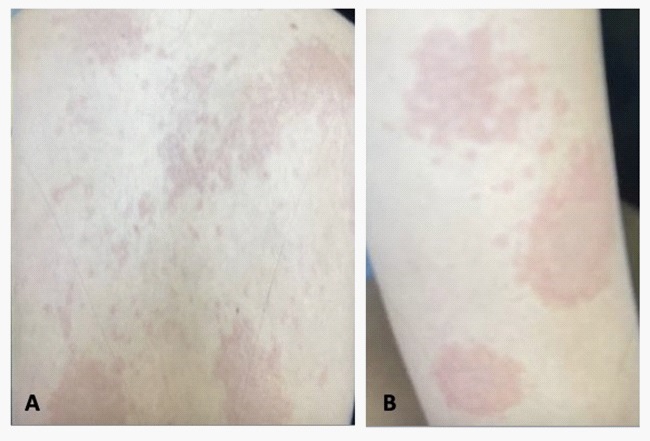
A 21-year-old healthy Caucasian female was diagnosed with SARS-CoV-2 infection in the setting of mild, transient symptoms including sore throat, fatigue, loss of taste and smell. She presented to the Emergency Department (ED) with new-onset chest pain 6 weeks after her recovery. She characterized the pain as sharp, radiating to the left shoulder that worsened with inspiration and improved when leaning forward. There was no associated dyspnea, nausea, or lower extremity edema. However, on further questioning, she endorsed intermittent episodes of watery diarrhea a few days prior to her presentation. In addition, new patches of erythematous, macular rash were present on her torso and arms (Figure 1). Initial vital signs in the ED included: fever of 102.2 F, heart rate of 130 beats per minute, blood pressure of 103/63 mmHg, and oxygen saturation of 97% on room air. Laboratory parameters showed normal white blood cell count (WBC), normal renal and liver function but troponin-I was severely elevated at 5.937 цg/L (normal range: <0.045 цg/L; Table 1). Twelve lead electrocardiogram revealed diffuse PR segment depression and T-wave inversion in leads III and aVF. Urgent transthoracic echocardiogram (TTE) showed normal left ventricular function (LVEF: 55-60%) with no evidence of regional wall motion abnormalities or pericardial effusion. The diagnosis of myopericarditis was made in the setting of potential MIS-A and treatment was initiated with a non-steroidal anti-inflammatory agent. Infectious disease team recommended against intravenous immunoglobulin (IVIG) or steroid administration, given patients’ hemodynamic stability but agreed to proceed with further viral studies and empirical broad-spectrum antibiotic administration.
Table 1: Selected laboratory values on admission (Day 1) and subsequent hospital days. CRP: C-reactive protein; IL-6: Interleukin-6; NT-proBNP: N-terminal pro-brain natriuretic peptide; PTT: partial thromboplastin time; TEG: thromboelastography; WBC: white blood cell count.
|
Day 1 |
Day 2 |
Day 3 |
Day 4 |
Day 5 |
Day 6 |
Day 7 |
WBC (109/L) |
8.1 |
7.3 |
6.4 |
14.6 |
13.8 |
14.5 |
14.6 |
Creatinine (mg/dL) |
0.75 |
0.79 |
0.70 |
0.87 |
0.85 |
0.85 |
0.79 |
Troponin-I (цg/L) |
5.937 |
1.542 |
0.325 |
0.195 |
0.144 |
0.088 |
0.048 |
NT-proBNP (pg/mL) |
|
15,391 |
7,494 |
4,806 |
3,583 |
2,729 |
1,126 |
CRP (mg/L) |
250 |
180 |
190 |
93 |
39 |
24 |
12 |
IL-6 (pg/mL) |
|
257.73 |
|
|
|
|
|
Ferritin (ng/mL) |
|
162 |
216 |
208 |
146 |
|
|
Procalcitonin (ng/mL) |
|
0.3 |
0.17 |
0.1 |
<0.05 |
<0.05 |
|
PTT (sec) |
|
48 |
34 |
29 |
28 |
26 |
26 |
INR |
|
1.27 |
1.23 |
1.10 |
1.06 |
1.08 |
1.07 |
D-Dimer (цg/ml) |
2.7 |
2.8 |
2.6 |
1.9 |
1.5 |
1.4 |
1.5 |
Fibrinogen (mg/dL) |
|
686 |
772 |
633 |
500 |
495 |
431 |
Factor 8 assay (%) |
|
208 |
292 |
284 |
288 |
327 |
300 |
TEG with heparinase |
|
5.7 |
7.6 |
5.8 |
|
|
|
The patient’s clinical condition worsened within the next 6 hours. Her temperature rose to 103.5 F, blood pressure decreased to 81/45 mmHg and sinus tachycardia persisted. She required continuous intravenous fluid administration with intermittent boluses to maintain a mean arterial pressure (MAP) of 65-70 mmHg. With the aggressive fluid resuscitation, she became increasingly hypoxic and required 6 liters of oxygen supplementation via nasal cannula. Chest X-ray findings were consistent with pulmonary edema and serum N-terminal probrain natriuretic peptide (NT-proBNP) level was severely elevated at 15,391 pg/mL. Fluid administration was discontinued at this time.
Hematology team recommended obtaining further laboratory tests including C-reactive protein (CRP), Interleukin-6 (IL-6), Procalcitonin, Ferritin, INR, partial thromboplastin time (PTT), Fibrinogen level, D-Dimer, Factor 8 activity and thromboelastography (TEG) with heparinase (Table 1). Given the change in patient’s clinical course, Ibuprofen was discontinued and methylprednisolone 1 mg/kg twice daily, aspirin 975 mg twice a day, enoxaparin 40 mg daily, as well as colchicine 0.6 mg daily were initiated. Intravenous immune globulin (IVIG) administration was deferred. Workup for infectious etiologies, including viral and bacterial, remained negative and antibiotics were discontinued (Table 2). Cardiac magnetic resonance imaging (CMRI) was performed on hospital day 3 and revealed a LVEF of 52%, normal right ventricular function, mild to moderate mitral regurgitation with no evidence for myocardial fibrosis, infarction, infiltrative diseases, or pericardial enhancement. T1 value was diffusely elevated while T2 signal was normal suggesting myocardial inflammation (Figure 2).
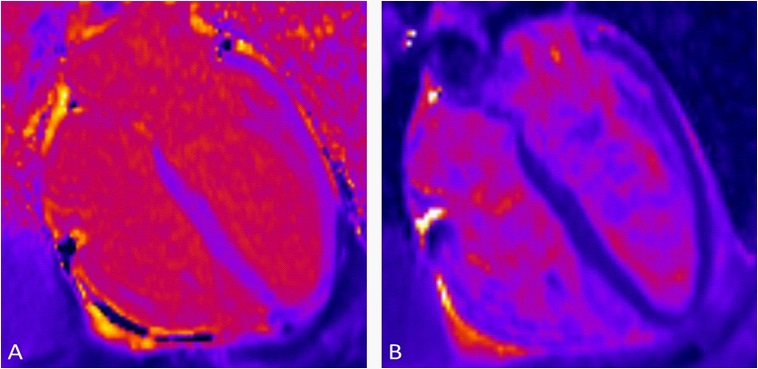
Table 2:Results of the infectious disease evaluation.
Test |
Result |
SARS-CoV-2 PCR |
Negative |
COVID-19 Spike RBD antibody |
Positive |
COVID-19 Spike RBD antibody titer |
1:3200 |
Influenza A |
Negative |
Influenza B |
Negative |
Respiratory Syncytial Virus PCR |
Negative |
Epstein-Barr Virus antibody |
Negative |
Coxsackie B virus panel |
Negative |
Blood cultures |
Negative |
Urine analysis/culture |
Negative |
Chest X-ray |
Negative |
Over the course of her 7-days hospitalization, her clinical condition improved, fevers subsided, and inflammatory markers improved significantly (Table 1). Serum troponin-I level normalized. Patient was discharged home with prednisone taper, high dose aspirin twice a day for 3 months and strict restrictions on physical activity. She was followed closely in the outpatient setting and continued to improve clinically. A repeat CMRI five months after her initial admission showed normal biventricular function, no mitral regurgitation, and complete resolution of prior T1 signal abnormalities. Cardiopulmonary exercise stress test (CPX) confirmed normal exercise capacity and no stressinduced cardiac arrhythmias were documented. Patient’s activity restrictions were lifted, and she was cleared to receive the COVID-19 vaccine.
Discussion
MIS-A is a rare, but potentially life-threatening multisystem inflammatory condition that typically develops 2-12 weeks after infection with the SARS-CoV-2 virus [2]. Establishing the diagnosis requires a high index of suspicion given that the presenting symptoms may be non-specific and can mimic numerous, highly diverse disease conditions [3,4]. The CDC defined MIS-A according to the following criteria: 1) severe illness requiring hospitalization in a person aged ≥21 years, 2) a positive test result for current or previous SARS-CoV-2 infection during admission or in the previous 12 weeks, 3) severe dysfunction of one or more extrapulmonary organ systems, 4) laboratory evidence of severe inflammation, and 5) absence of severe respiratory illness [1]. As per the definition, MIS-A develops as a complication of COVID-19 disease, yet individuals may remain completely asymptomatic, or may even be unaware of the index infection. Therefore, a thorough history and physical examination as well as laboratory work-up, including SARS-CoV-2 antibody detection is necessary. Once the diagnosis is established, supportive therapy is always indicated, such as pain/fever control, oxygen administration, hydration, and mechanical circulatory/ventilatory support, if necessary. In addition, interventions to suppress the hyperactive immune response may be required using IVIG, high-dose corticosteroids, anakinra, interleukin-6 inhibitors [5].
The true incidence of MIS-A-associated myocardial injury remains unknown. It may present as asymptomatic troponin elevation, myopericarditis, diffuse myocardial inflammation, acute left ventricular dysfunction, or cardiogenic shock [4,6]. Recognizing the cardiac involvement of MIS-A is of critical importance. It will not only affect immediate medical care but will also determine long-term monitoring requirements. As in our case, repeat cardiac MRI may be necessary to ensure the resolution of myocardial involvement. In addition, performing a supervised exercise stress test 3 to 6 months after the index admission may help to appropriately risk stratify patients prior to permitting athletic activities. These follow-up evaluations are especially important in young, otherwise healthy individuals.
References
- CDC. Multisystem Inflammatory Syndrome in Adults (MIS-A) Case Definition Information for Healthcare Providers. 2021.
- Morris SB, Schwartz NG, Patel P, Abbo L, Beauchamps L, Balan S, et al. Case Series of Multisystem Inflammatory Syndrome in Adults Associated with SARS-CoV-2 Infection - United Kingdom and United States, March-August 2020. MMWR Morb Mortal Wkly Rep. 2020; 69(40): 1450-6.
- Rubens JH, Akindele NP, Tschudy MM, Sick-Samuels AC. Acute covid-19 and multisystem inflammatory syndrome in children. BMJ. 2021; 372: n385.
- Hekimian G, Kerneis M, Zeitouni M, Cohen-Aubart F, Chommeloux J, Brechot N, et al. Coronavirus Disease 2019 Acute Myocarditis and Multisystem Inflammatory Syndrome in Adult Intensive and Cardiac Care Units. Chest. 2021; 159(2): 657-62.
- Cattaneo P, Volpe A, Cardellino CS, Riccardi N, Bertoli G, Ursini T, et al. Multisystem Inflammatory Syndrome in an Adult (MIS-A) Successfully Treated with Anakinra and Glucocorticoids. Microorganisms. 2021; 9(7).
- Janardhanan R. Myocarditis with very high troponins: risk stratification by cardiac magnetic resonance. J Thorac Dis. 2016; 8(10): E1333-E6.