
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
An unusual case of breast abscess caused by Proteus mirabilis and Prevotella buccalis
Elhanan Parnasa, MD1; Adiel Cohen, MD2; Bar Avital, MD3; Yafa Shani Parnasa, MD4; Yonatan Oster, MD5,6*
1 Department of Internal Medicine, Hadassah Medical Organization and Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel.
2 Department of Obstetrics and Gynecology, Hadassah Medical Organization and Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel.
3 Hadassah-Hebrew University Medical Center, Jerusalem, Israel.
4 Department of surgery, Hadassah Medical Organization and Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel.
5 Department of Clinical Microbiology and Infectious Diseases, Hadassah University Medical Center, Jerusalem, Israel.
6 Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel.
# Equal contribution: Elhanan Parnasa & Adiel Cohen
*Corresponding Author: Yonatan Oster
Department of Clinical Microbiology and Infectious
Diseases, Hadassah-Hebrew University Medical Center, EinKerem POB 12000, Jerusalem 91120, Israel
Email: yonatano@hadassah.org.il
Received : Sep 23, 2021
Accepted : Nov 08, 2021
Published : Nov 15, 2021
Archived : www.jcimcr.org
Copyright : © Oster Y (2021).
Abstract
A 56-year-old nulliparous woman presented to the emergency department with acute onset of redness, sensitivity, and local fever in the left breast. Mastitis with abscess was diagnosed. Unusual pathogens were identified in the culture obtained from the abscess - Proteus mirabilis and Prevotella buccalis.
Keywords: breast abscess; Proteus mirabilis; Prevotella buccalis.
Citation: Parnasa E, Cohen A, Avital B, Parnasa YS, Oster Y. An unusual case of breast abscess caused by Proteus mirabilis and Prevotella buccalis. J Clin Images Med Case Rep. 2021; 2(6): 1406.
Introduction
Mastitis is a common infection, which mostly occurs in young women during the puerperium period. The most common bacteria causing mastitis is Staphylococcus aureus [1]. Among the risk factors for mastitis is the presence of S. aureus in the nipple or breast milk, nipple damage, use of nipple shields for nursing, or oversupply of breast milk [2].
Breast abscesses are an uncommon complication of mastitis. Most of the abscesses can be diagnosed by ultrasound scan [1]. True abscesses require drainage, in addition to antibiotics treatment [3].
We wish to report a case of breast abscess with unusual pathogens.
Case presentation
A 56-year-old nulliparous woman presented to the emergency department with five days of redness, sensitivity, and local fever in the left breast.
Past medical history included ischemic heart disease, dyslipidemia, asthma and G6PD deficiency. Her last routine mammography, in the previous year, was normal.
On physical examination, she did not have a fever. Her left breast was red, with induration and retraction of the nipple, without any discharge. Enlarged lymph nodes were palpated on her left axilla. On the right breast, there was a small hematoma. The rest of the exam was unremarkable.
In the lab, electrolytes and creatinine were in the normal range. There was not any leukocytosis nor thrombocytosis. Creactive protein was 5.71 mg/dl (0-0.5). Two sets of blood cultures were obtained.
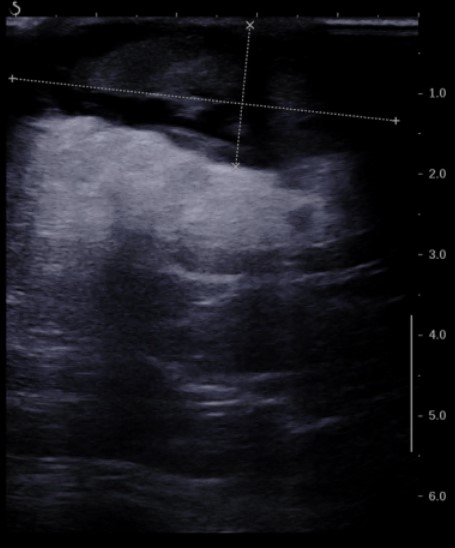
She underwent an ultrasound scan of the left breast which showed a fluid collection about 4 X 1.5 cm behind the nipple, which was diagnosed as an abscess (Figure 1). In addition, a single enlarged lymph node was seen at the left axilla.
The abscess was drained, and the pus was sent for culture. Empiric antibiotic treatment with Cefazolin was started and the patient was hospitalized for further investigation and treatment.
During hospitalization, the results of the blood cultures came back and were negative. However, two microorganisms were identified in the culture obtained from the abscess: Proteus mirabilis and Prevotella buccalis. A resistance profile of the Proteus showed susceptibility to all beta-lactams and aminoglycosides, thus the antibiotic treatment was changed to Ceftriaxone.
Due to lack of clinical improvement, second drainage of the left breast was done two days later, after which the patient improved clinically and was discharged with further antibiotic treatment of oral Cefuroxime Axetil for seven days.
Discussion
Proteus mirabilis as the causative bacteria of breast abscess is uncommon and described before in the medical literature as involved in as much as 5% of all breast abscess [4]. We believe that those reports in the past and this report are important andshould be in the mind of clinicians when they choose empiric antibiotics, or as a possible explanation when there is a treatment failure. Prevotella species has been described as part of the normal microbiome of the human breast tissue, its’ role in the pathogenesis of breast abscess is not known [5].
Moreover, this report shows the importance of abscess drainage not only for the sake of treatment but also for obtaining cultures that would guide the suitable antibiotic treatment in patients with breast abscess.
References
- Boakes E, Woods A, Johnson N, Kadoglou N. Breast Infection: A Review of Diagnosis and Management Practices. Eur J Breast Health. 2018; 14(3): 136-143.
- Cullinane M, Amir LH, Donath SM et al. Determinants of mastitis in women in the CASTLE study: a cohort study. BMC Fam Pract. 2015; 16: 181.
- Townsend, Courtney M., Beauchamp, R. Daniel, Evers, B. Mark, & Mattox, Kenneth L. (2017). Diseases of the Breast. In Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice (20th ed., pp. 816–864). Elsevier.
- Moazzez A, Kelso RL, Towfigh S, Sohn H, Berne TV, Mason RJ. Breast abscess bacteriologic features in the era of communityacquired methicillin-resistant Staphylococcus aureus epidemics. Arch Surg. 2007; 142(9): 881-4.
- Nagy E. Anaerobic infections: Update on treatment considerations. Drugs. 2010; 70(7): 841-58.