
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A pneumatocele observed in the thoracic cavity after bronchoalveolar lavage
Satoshi Tanaka, MD*; Riiko Kitou, MD; Kiyohide Komuta, MD; Satoshi Tanizaki, MD; Tomohiro Kanai, MD; Junji Uchida, MD, PhD; Kiyonobu Ueno, MD, PhD
Department of Respiratory Medicine, Osaka General Medical Center, 3-1-56 Bandai-higashi, Sumiyoshi, Osaka 558-8558, Japan.
*Corresponding Author: Satoshi Tanaka, MD
Department of Respiratory Medicine, Osaka General
Medical Center, 3-1-56 Bandai-higashi, Sumiyoshi,
Osaka 558-8558, Japan
Email: satoshi112427@yahoo.co.jp
Received : Oct 20, 2021
Accepted : Nov 11, 2021
Published : Nov 18, 2021
Archived : www.jcimcr.org
Copyright : © Tanaka S (2021).
Citation: Tanaka S, Kitou R, Komuta K, Tanizaki S, Kanai T, et al. A pneumatocele observed in the thoracic cavity after bronchoalveolar lavage. J Clin Images Med Case Rep. 2021; 2(6): 1412.
Description
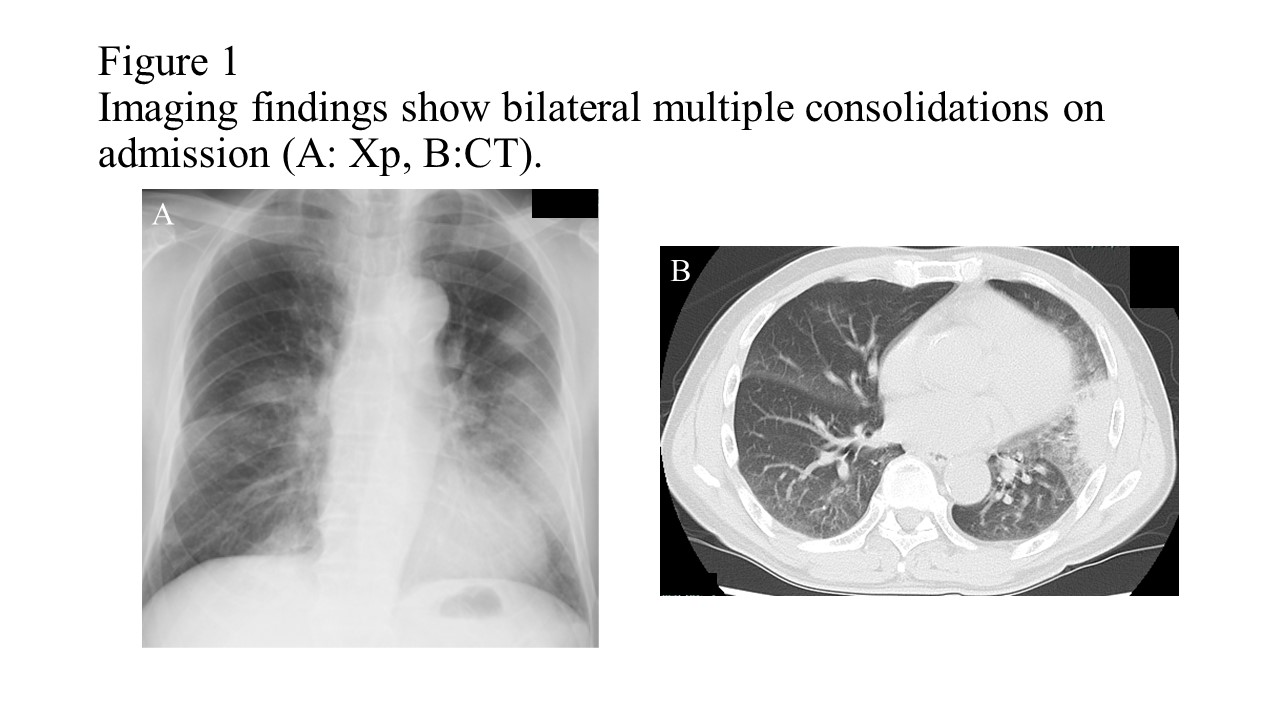
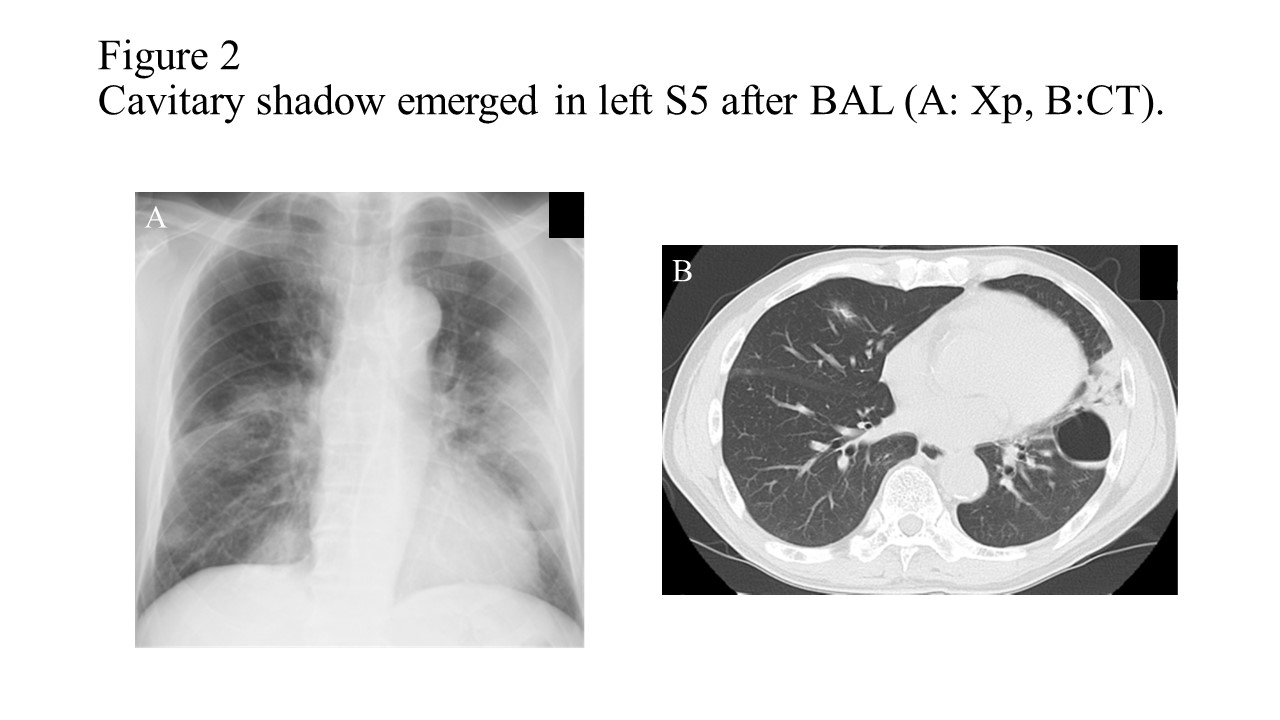
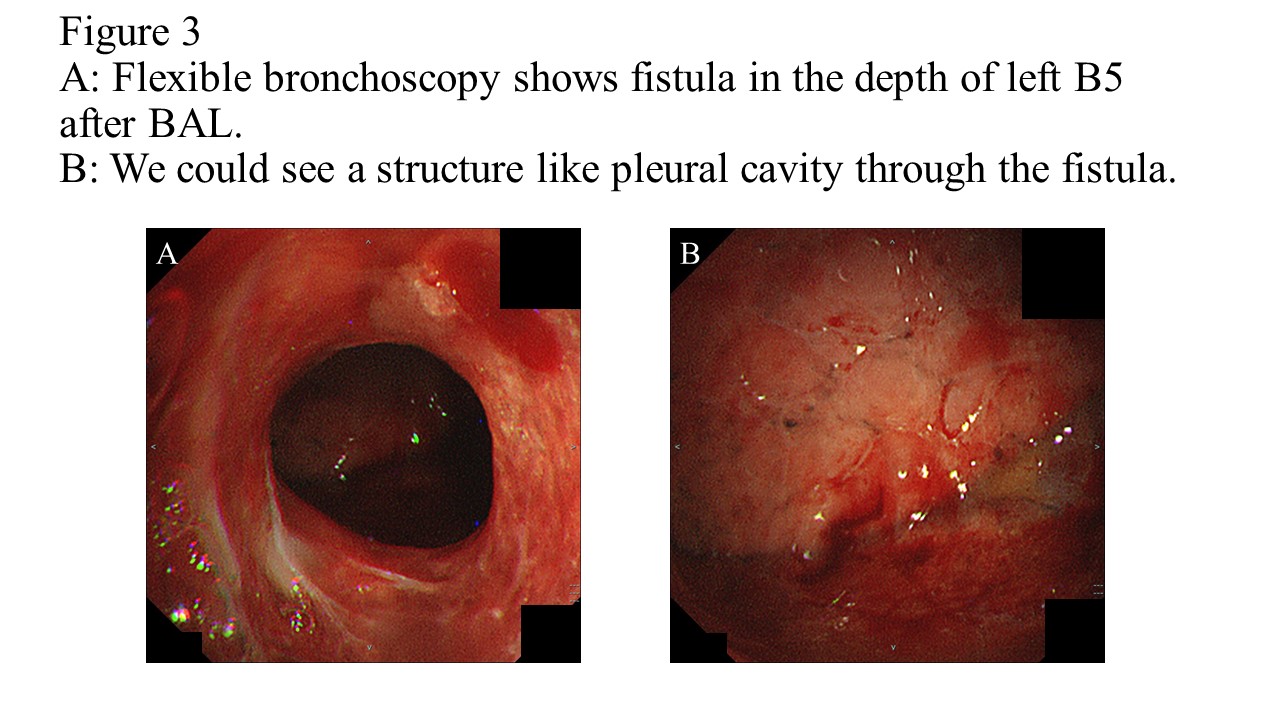
A 76-year-old man was admitted to the respiratory medicine department with 5 days of a non-productive cough and exertional dyspnea. A computed tomography revealed multiple mild patchy consolidations in both lungs (Figure 1). Despite antibiotic therapy, there was poor improvement in laboratory and radiological parameters. A bronchoscopy was performed on day 5. The bronchoscopy was wedged in left B5 and a bronchoalveolar lavage (BAL) was performed. After the BAL, we noticed a fistula in the depth of left B5 and saw a structure like a pleural cavity in the back of the fistula (Figure 2). We diagnosed the patient’s condition as pneumatocele (PC). BAL showed 46% lymphocytes and the CD4/8 ratio as 3:7. These findings suggested cryptogenic organizing pneumonia (COP). It took 3 weeks for the PC to improve. Bilateral multiple consolidations improved after the administration of a steroid (PSL 0.5 mg/kg). PCs can occur in infections, chest trauma, barotrauma from mechanical ventilation, and bronchial interventions [1,2]. The mechanism of PC formation is closely related to that of a check valve. The check valve may be composed of exudate from inflammation and the destroyed wall of the respiratory tract [3]. In this case, it was considered that the wedged bronchoscopy and collapsed bronchial wall became the check-valve. PCs can be a severe condition including tension pneumothorax, bronchopleural fistula, and secondary infections [4]. In our case, as we were concerned about new complications due to the PC we did not prescribe a steroid for COP until the PC had improved. To our knowledge, no papers have reported internal observations of PC. We herein report the first case of PC observed in the thoracic cavity after BAL.
Declarations
Author contribution statement: All authors participated in the treatment of this case, and the first author drafted the manuscript. All authors read and approved the final manuscript.
Conflict of interest: The authors declare no conflicts of interest.
Founding statement: This study has no funding.
References
- Tuhina R, Neil M, Bharat A. Pneumatocele as a complication of bronchoscopy: a case report and review of literature. 2007; 14: 2: 101-104.
- Lestelle F, Fumat R, Didier A,CollotSamia, Egenod T, et al. Pneumatoceles after bronchoscopic lung volume reduction with valves. ERJ open Res. 2021; 7: 00747-2020
- Quigley MJ, Fraser RS. Pulmonary pneumatocele: Pathology and pathogenesis. AJR Am J Roentgenol. 1988; 150: 1275-1277.
- Mathew PR, Nainesh KT, Basti SR, Suresh BH. Pulmonary pneumatocele: Its significance, aetiology, imaging features and follow up. Eurorad. European Society of Radiology [ESR]; 2015.