Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Massive pneumomediastinum following orotracheal intubation in an emergency setting
Lucas Ferreira Theotonio dos Santos*; Daniel Joelsons; Ho Yeh Li
ICU division, Infectious and Parasitic Diseases Department, Faculty of Medicine, University of Sao Paulo, Brazil.
*Corresponding Author: Lucas Ferreira Theotonio dos Santos
ICU division, Infectious and Parasitic Diseases Department, Faculty of Medicine, University of Sao Paulo, Brazil.
Email: theotonio.lucas.epm@gmail.com
Received : Sep 19, 2021
Accepted : Nov 12, 2021
Published : Nov 19, 2021
Archived : www.jcimcr.org
Copyright : © dos Santos LFT (2021).
Citation: dos Santos LFT, Joelsons D, Yeh Li H. Massive pneumomediastinum following orotracheal intubation in an emergency setting. J Clin Images Med Case Rep. 2021; 2(6): 1414.
Clinical image description
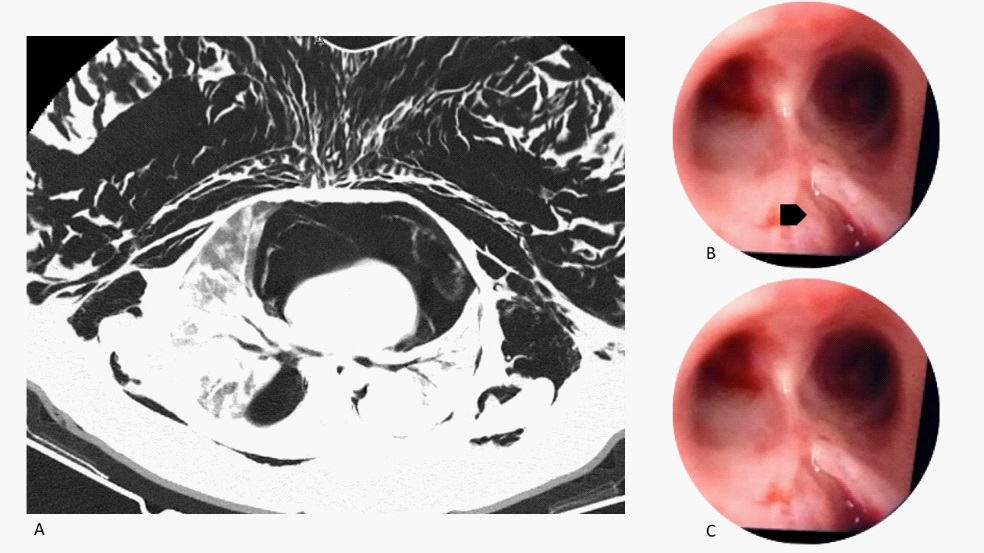
We admitted in our intensive care unit, a 34-year old, Female patient from the emergency room, with a hypothesis of COVID-19 disease, who was intubated before transportation due to hypoxemic respiratory insufficiency. In physical examination the patient showed a massive subcutaneous emphysema. A computed tomography confirmed the hypothesis of pneumomediastinum/pneumothorax (Figure 1A). Refractory hypoxemia issued despite optimized mechanical ventilation, so we opted to submit the patient to Extracorporeal Membrane Oxygenation (ECMO). A diagnostic bronchoscopy showed an important laceration of the trachea (Figure 1B, black arrow, and Figure 1C), near the carina. Despite rare, tracheal lesion after intubation may have a dramatic outcome.