
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Vanishing hyperintensity in MRI: Vascular or epileptic origin?
Rodriguez-Rivas Luis Ricardo1; Reyes-Vaca Jorge Guillermo1; Vázquez-Guevara Damaris Daniela1; Rodriguez-Leyva Ildefonso1*
1 Neurology Service, Faculty of Medicine, Universidad Autonoma de San Luis Potosi, Hospital Central “Dr. Ignacio Morones Prieto”, San Luis Potosí, SLP Mexico.
2 Radiology Service, Faculty of Medicine, Universidad Autonoma de San Luis Potosi, Hospital Central “Dr. Ignacio Morones Prieto”, San Luis Potosí, SLP Mexico.
*Corresponding Author: Ildefonso RodriguezLeyva
Neurology Service, Faculty of Medicine, Universidad
Autonoma de San Luis Potosi, Hospital Central “Dr.
Ignacio Morones Prieto”, San Luis Potosí, SLP Mexico.
Email: Ildefonso.rodriguez@uaslp.mx
Received : Sep 22, 2021
Accepted : Nov 16, 2021
Published : Nov 23, 2021
Archived : www.jcimcr.org
Copyright : © Rodriguez-Leyva I (2021).
Introduction
Status Epilepticus and epilepsy-related MRI vanishing changes have been reported in the literature since the 1980s; hypoxia and hypoperfusion have been related to these image modifications. These alterations and their disappearing characteristics can cause trouble among work up and their diagnosis, especially if there is no exact etiology of what is causing seizures. We present a case of a 37-year-old righthanded man with a 6-year history followed up after seizure debut, with no exact etiology at the first event, considering an ischemic event as etiology. After a six-year follow-up seizure-free and no sequels, the patient newly developed aphasia, seizures, and status epilepticus, with a now evident vascular abnormality (cavernous cerebral malformation) etiology in MRI imaging. The cumbersomeness of the clinical picture in its presentation, the seriousness to which it reached, and the complete resolution of the problem with medical treatment make this clinical case especially attractive.
Keywords: status epilepticus; vascular; cavernous cerebral malformation; vanishing lesions; magnetic resonance imaging.
Abbreviations: ER: Emergency Room, ICU: Intensive Care Unit, SE: Status Epilepticus, CCM: Cavernous Cerebral Malformation.
Citation: Luis Ricardo RR, Guillermo RVJ, Daniela VGD, Ildefonso RL. Vanishing hyperintensity in MRI: vascular or epileptic origin?. J Clin Images Med Case Rep. 2021; 2(6): 1419.
Case presentation
A 37-year-old right-handed man presented to the ER in August of 2020. The patient was awake, but he had difficulty speaking, and he did not understand verbal commands. We took the clinical history from his wife, who explained that the patient, an hour before arriving at the hospital, started with confusion and an impossibility to communicate verbally; despite being conscious, he did not answer to verbal stimulus pronounced words.
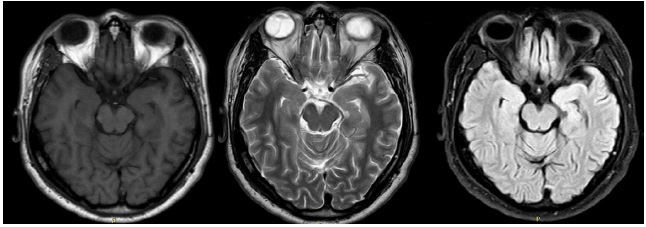
His past medical history included a previous hospitalization six years ago when he presented a similar “state of confusion” (a brief period of mutism, automatisms, and unresponsiveness) and an episode of a tonic-clonic seizure. During medical attention in the ER, he developed refractory status epilepticus, leading to ICU attention. An MRI was performed with T2/FLAIR sequence, showing a hyperintensity in the left parietal and temporal lobes with some DWI restriction. A cerebral biopsy was conducted in the core of the lesion, revealing data of an ischemic event. He was treated with FAE (VPA and LEV), statins, and anti-aggregating drugs. The patient was finally discharged home with bradypsychia, hiccups, and mild cognitive deficits affecting his language and memory. He improved progressively within the following months, regaining his complete previous functionality. During neurology follow-up visits, MRI findings disappeared completely; four years after he was functional, he was promoted in his job and left his medication.
Examination at the new clinical presentation found patient GCS 15 points, awake, now following some basic commands, with profound difficulty finding words and names, and failing executive function tasks. During the subsequent two-day evaluation in-hospital, the patient persisted with the same cognitive alterations. On the third night, he developed four tonic seizures that started with a loss of consciousness and dystonic limb posturing and then evolved to tonic-clonic attacks; the patient developed anxiety and aggressivity between episodes. The last seizure had status epilepticus criteria (more than 5 minutes), so he was treated with midazolam, and Levetiracetam was started with the resolution of status epilepticus. The patient remained conscious and developed continuous hiccups. During the week, the patient was discharged, but he still had language problems.
Investigations
During hospitalization, he underwent several studies for investigation.
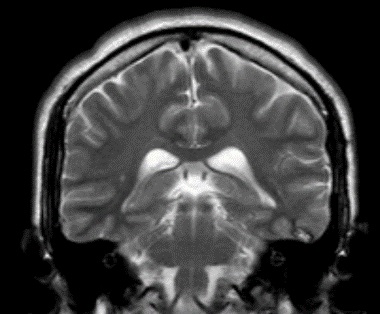
A general blood test was performed with no alterations. The CT scan was an initial imaging study with only findings related to a biopsy taken six years ago, but the rest of the study was normal. Next, an MRI was performed, with a “popcorn ball” like lesion in the left temporal lobe, T1WI C+ showing no enhancement, FLAIR with minimal edema surrounding the lesion, T2WI small popcorn ball lesion with a hypointense rim.
EEG was performed a day after the clinical convulsive seizures and resolved status epilepticus; EEG showed a background rhythm reaching 8-10Hz, reactive to external stimulation, with non-frequent epileptiform activity in the left temporal lobe.
Differential diagnosis
The differential diagnosis initially focused on a cerebrovascular event, our main possibilities being an arterial or venous ischemic event (mainly since it was evanescent in the previous event). However, the finding of the cavernous angioma and the presence of seizures that led to status epilepticus both on this occasion and the previous one forced us to consider the possibility that the language alterations and apparent confusion were more than episodes associated with the presence of cavernous angioma and that the lesion seen in the vicinity was related to the critical event presented.
Treatment
After being diagnosed with cavernous hemangioma and epilepsy, Levetiracetam was started as a daily dose of 1 gr twice daily and escalated to 1.5 gr twice a day. Metoclopramide was started 10 mg twice daily for control of hiccups.
Outcome and follow-up
The patient gradually improved; he maintained complete attention and had non-cognitive deficits on day 5. However, hiccups lasted for almost an entire week. After being discharged home, a neurology external consult follow up 15 days post hospitalization showed a completely recovered patient with no new seizure events or spells.

Discussion
Vanishing lesions in epilepsy and cerebrovascular diseases have been reported in the last 30 years as complex to work up and get to a final etiology. The importance of this clinical case is the coincidental situation of both problems in the same patient [1-3].
The temporal lobe is a common localization for focal epilepsy; it is essential to recognize its clinical presentation to correct it. Temporal mesial lobe seizure typically starts with aura (déjà vu, jamais vu, or a strange sensation of "butterflies" in the patient's stomach) and loss of consciousness/awareness prominent oral and manual automatisms. Ictal manifestations like dystonic limb posturing are important manifestations [4,5].
Our patient started with a very similar clinical presentation of symptoms like he did six years ago; both times, he developed a classical temporal lobe aura and ictal manifestations that evolved to secondarily generalized seizures that led him to status epilepticus. This time, on guard physicians, reported aggressiveness, anxiety, and disorientation between attacks, the last one led to physical restrain of the patient as he started destroying his surroundings; episodes of confusion and anxiety are typically reported and localized at temporal lobe origin, although the frequency of postictal violence it has considered rare [6-8].
The etiology of temporal lobe epilepsy has been associated with a back history of prolonged febrile seizure; with our patient not having this antecedent, other etiology's like cavernous hemangiomas, gliosis, or tumours had to be considered [9].
The etiology of this patient was finally found. Six years ago, he presented to ER with clinical characteristics of an epileptic seizure (epilepsy debut) that developed refractory status epilepticus. At that time, on MRI (which was done a day after the onset of refractory status epilepticus), cavernoma was not found.
Instead, cortical hyperintensity was found on temporal and slightly on parietal lobe in T2/FLAIR MRI sequences, as well as some DWI restriction; at that time, not having a specific etiology, a lumbar puncture was performed to diagnose an inflammatory process (autoimmune, infectious) but CSF analysis was utterly normal. Therefore, vascular etiology appeared to be a possible diagnosis. However, the patient's age, diet and exercise history, and no smoking background, drugs, or drinking made doubt remained. Again, no abnormality was found on blood tests related to stroke on a young patient, so a biopsy was performed with necrosis findings.
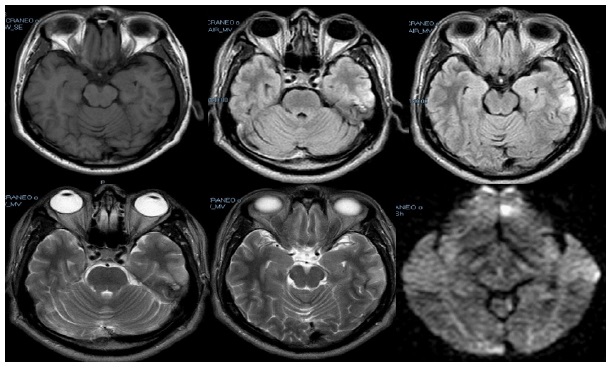
The patient presented this time with the same spot hyperintensity on T2/FLAIR MRI and DWI sequences; it has been described that focal epilepsy and especially status epilepticus can have these abnormalities on imaging cytotoxic edema and laminar necrosis. Status epilepticus has previously been proven to produce MRI modifications in the neocortical region related to the zone of seizure onset, with reversible diffusion and perfusion changes in non-convulsive SE [10].
Several papers even describe MRI enhancement patterns typically related to SE; most reported a hippocampal alteration (the most common one) related to temporal lobe epilepsy. And cortical changes are commonly found in patients with hypoxia or hypo-perfusion (both patterns appreciated on initial MRI 6 years ago and cortical pattern in this hospitalization). These MRI findings are generally reversible and can re-emerge in the same area as a focal area of epilepsy. Our patient MIR imaging showed in the follow up of first status epilepticus six years ago and then re-emerging this hospitalization as he had the same seizure clinical characteristics [10].
Final Etiology was a cavernous cerebral malformation known as cavernomas or cavernous hemangiomas; these are clusters of abnormal and hyalinized capillaries without intervening brain tissue, though lesions in the basal ganglia, brainstem, cerebellum, and spine also can occur. Epileptic seizures are the most common form of clinical presentation of a CCM. However, they are usually found more commonly incidentally when performing imaging studies for other causes (frequency of incidental findings in patients presenting with epilepsy is the same as in the general population: 0.4-0.9%). CCMs are lesions that can occur at any site within the central nervous system. Most of them are found in a supratentorial location. Their progression can vary from shrinking to an overgrowth in time. Sometimes the lesion is so small it is difficult to localize [11-13].
Declarations
Formatting of funding sources: The case report did not receive any financial or political funding.
Patient consent: We received the absolute consent of the patient to make use of the information presented in this case.
References
- Chopra JS., et al. “Vanishing CT lesions in epilepsy.” Journal of the neurological sciences. 1992; 107.1: 40-49.
- Rao T. Hemanth Richard B. Libman, and Mahendra Patel. “Seizures and ‘disappearing’ brain lesions.” Seizure. 1995; 4.1: 61- 65.
- Ferro José M, and Patrícia Canhão. “Cerebral venous sinus thrombosis: update on diagnosis and management.” Current cardiology reports. 2014; 16.9: 523.
- Tatum WO 4th. Mesial temporal lobe epilepsy. Journal of Clinical Neurophysiology. 2012; 29: 356-365.
- Loddenkemper T, Kotagal P. Lateralizing signs during seizures in focal epilepsy. Epilepsy and Behavior 2005; 7: 1-17.
- Marsh L, Krauss GL. Aggression and violence in patients with epilepsy. Epilepsy Behav. 2000; 1: 160–8.
- Gerard ME, Spitz MC, Towbin JA, Shantz D. Subacute postictal aggression. Neurology. 1998; 50: 384–8.
- Ito M, Okazaki M, Takahashi S, Muramatsu R, Kato M, Onuma T. Subacute postictal aggression in patients with epilepsy. Epilepsy Behav. 2007; 10: 611–4.
- Skidmore C. Adult focal epilepsies. Continuum (Minneap Minn). 2016; 22: 94–115.
- Milligan T, Cavani A, Bromfield E. Frequency and patterns of MRI abnormalities due to status epilepticus. Seizure. 2009; 18: 104–108
- Rosenow F, Alonso M, Baumgartner C, Blümcke I, Carreño M et al. Cavernoma-related epilepsy: Review and recommendations for management — Report of the Surgical Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2013; 54: 2025–2035.
- Dalai RT, Ghobrial G, Awad I, Tjoumakaris S, Gonzalez LF, et al. Management of incidental cavernous malformations: a review. Neurosurg Focus. 2011; 31: E5.
- Ene C, Kaul A, Kim L. Natural history of cavernous cerebral malformations. Handb Clin Neurol. 2017; 143: 227-232.