
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Endocarditis following an unsuccessful attempt to remove a gastric GI stromal tumor by laparoscopic endoscopic cooperative surgery
Ali Abdullah; Marina Somi; Pavel Alin; Sara Shimoni; Stephen Malnick*
Department of Internal Medicine C, Heart Institute, Kaplan Medical Center, Rehovot 76100, Israel.
*Corresponding Author: Stephen Malnick
Department of Internal Medicine C, Kaplan Medical
Center, Rehovot 76100, Israel.
Email: stephen@malnick.net
Received : Sep 22, 2021
Accepted : Nov 16, 2021
Published : Nov 23, 2021
Archived : www.jcimcr.org
Copyright : © Malnick S (2021).
Abstract
Gastrointestinal Stromal Tumors (GIST) are the most common subepithelial lesions of the gastrointestinal tract. Treatment of lesions greater than 2 cm in diameter is by laparoscopic wedge resection.
We report a 77-year-old man who was diagnosed with a 2.3 cm diameter gastric GIST. He had a thickened mitral valve, severe mitral annular calcification, mild mitral regurgitation and moderate aortic stenosis.
One week after undergoing an unsuccessful attempt at Laparoscopic Endoscopic Cooperative Surgery (LECS), he was admitted with a fever of 40.2o C. Blood cultures grew Staphylococcus lugdunensis. Transthoracic and transesophageal echocardiography revealed moderate mitral regurgitation and an 8 X 5 mm vegetation on the mitral valve and posterior annulus.
This is the first report of endocarditis following LECS. Physicians need to be aware of this possible complication.
Keywords: endocarditis; GI stromal tumor; endocarditis; endoscopic tumor.
Citation: Abdullah A, Somi M, Alin P, Shimoni S, Malnick S. Endocarditis following an unsuccessful attempt to remove a gastric GI stromal tumor by laparoscopic endoscopic cooperative surgery. J Clin Images Med Case Rep. 2021; 2(6): 1420.
Introduction
Gastrointestinal Stromal Tumors (GIST) are common malignant subepithelial tumors [1]. The preferred treatment for endoscopically unresectable lesions is laparoscopic wedge resection. Recently a new method of surgery, laparoscopic endoscopic cooperative surgery (LECS), has been developed and some cases of GIST resection have been described.
We report an unique case of infective endocarditis following an unsuccessful attempt at LECS resection of a gastric GIST tumor.
Case report
A 77-year-old man presented with a 2-day history of fever of 40o C, confusion and dysuria, with no hematuria. There were no gastrointestinal or respiratory complaints.
His past medical history included hypertension, atrial fibrillation, hyperlipidemia, and a previous ischemic, cerebrovascular event. Two-dimensional transthoracic echocardiography revealed a thickened mitral valve with severe mitral annular calcification, mild mitral regurgitation, diastolic LV dysfunction, and moderate aortic stenosis. Three years previously he had a right colectomy for moderately differentiated adenocarcinoma and was assessed as being disease free. CT scan 2 years previously revealed a gastric diverticulum, with no evidence for recurrence or metastasis. A year later repeat CT scan showed a 2.3 cm diameter lesion on the lesser curvature of the stomach. Gastroscopy and biopsy of this lesion was consistent with a Gastrointestinal Stromal Tumor (GIST).
One week previously before he underwent an unsuccessful attempt at Laparoscopic Endoscopic Cooperative Surgery (LECS) to remove the GIST. On examination, temperature was 40.2°C, blood pressure 165/70 mmHg and the pulse rate was 97 per minute. Heart sounds were normal and regular with a systolic murmur of 2/6 intensity audible at the apex and radiating to the axilla. Pulmonary and abdominal examination were noncontributory. Laboratory tests revealed a mild neutrophil leukocytosis to 14000/µL, hyperglycemia of 236 mg/dL and hyponatremia of 127 mEq/l. The C reactive protein level was increased to 9.5 mg/dL (Table 1).
Table 1:Laboratory investigations during the hospital admission.
Day 13 |
Day 6 |
Day 3 |
Day 1 |
|
9.2 |
9.2 |
10.4 |
14 |
WBC (k/ul) |
76.20 |
72.20 |
77.20 |
89.90 |
Neut (%) |
12.2 |
12.3 |
12.8 |
13.3 |
HB (g/dL) |
213 |
133 |
104 |
127 |
PLT (k/ul) |
130 |
159 |
160 |
236 |
Glucose (mg/dL) |
0.96 |
0.8 |
0.95 |
1.25 |
Creatinine (mg/dL) |
34 |
39 |
56 |
48 |
UREA (mg/dL) |
5.57 |
9.87 |
* |
9.52 |
CRP (mg/dL) |
|
|
|
|
|
The ECG showed normal sinus rhythm and on chest x ray there were signs of pulmonary congestion. Urinalysis revealed only traces of ketone and glucose. Several blood cultures and a urine culture were taken. Empirical antibiotic therapy with intravenous ceftriaxone was commenced.
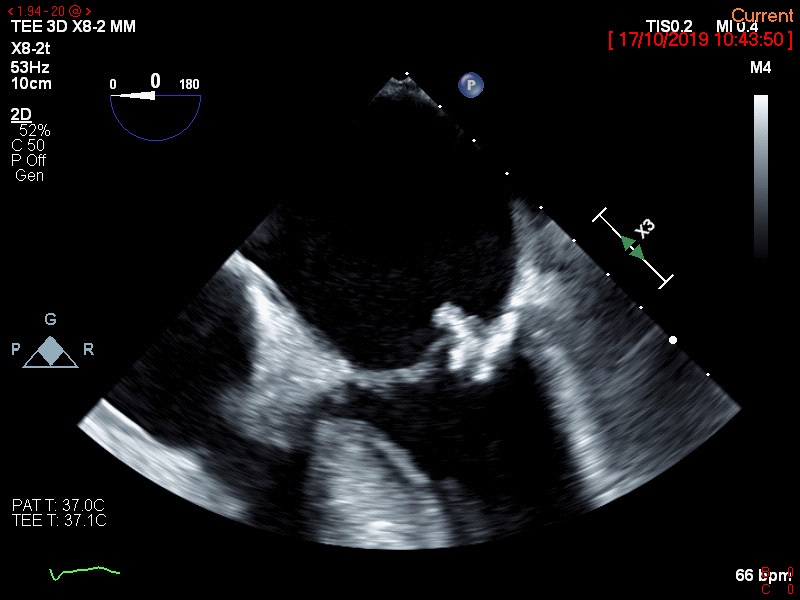
Staphylococcus lugdunensis was cultured from two separate blood cultures and the urine was sterile. Trans thoracic and subsequently trans-esophageal echocardiography were performed. They revealed vegetations on the mitral valve (8 X 5 mm in diameter) and on the posterior annulus (Figure 1). Severe mitral annulus calcification and moderate mitral regurgitation were also present. The patient was treated with intravenous cloxacillin. The risk for operative treatment of the mitral valve was judged to be too high and the decision was made to give longterm antibiotic treatment.
Discussion
We present a case of Staph. Lugdunensis endocarditis following an unsuccessful attempt by LECS to remove a gastric GIST. The patient fulfills the modified Duke Criteria [2] on the basis of two major clinical criteria (blood cultures positive for endocarditis and evidence of endocardial involvement) and one minor clinical criterion (fever) .
Staphylococcus lugdunensis is a Coagulase-Negative Staphylococcus (CoNS) inhabitant of the human skin flora. S lugdunensis has been linked to skin and soft tissue infections resulting in bacteremia and native valve endocarditis [3,4]. Interestingly, 29 (81%) of 36 cases had a history of surgical procedures or an implanted medical device [4].
Antibiotic prophylaxis is indicated for patients at highest risk for IE, including patients with any prosthetic valve, a previous episode of IE, and congenital heart diseases. Antibiotic prophylaxis is not, however, recommended for gastroscopy, colonoscopy, or transesophageal echocardiography [5].
The treatment of IE includes long-term antibiotic treatment and possible surgical intervention for repair or replacement of the infected valve. The operative risk on this patient was assessed as being very high and the decision was made to give long-term antibiotic treatment.
GISTs are largely caused by oncogenic mutations in the tyrosine kinase receptor KIT6 and/or platelet-derived growth factor receptor-α (PDGFR-α) [1]. Approximately 10% to 30% of GISTs have a malignant clinical behavior.
Gastric GISTS more than 2 cm in diameter should be resected. Surgical resection is the preferred treatment for resectable GISTs without evidence for metastasis. Metastatic, unresectable or recurrent GIST tumors are treated by tyrosine kinase inhibitors [7].
Laparoscopic surgery (LSG) is recommended for GISTs that are less than 5 cm and located in the stomach and small bowel [7]. Simple wedge resection is the treatment of choice [7]. Endoscopic Resection (ER) is also an effective method for treating GIST tumors less than 5 cm in size. A recent comparison of 51 endoscopic resection patients matched by propensity score to 403 Surgically Resected (SR) patients, all with tumors less than 5 cm in diameter, found no difference in recurrence or metastasis between the ER or SR groups [8].
Laparoscopic and Endoscopic Cooperative Surgery (LECS) is a novel surgical technique that combines laparoscopic partial gastrectomy and endoscopic submucosal dissection [9].
LECS is performed under general anesthesia for gastric SMTs (mainly GIST), without epithelial lesions including depressed lesions and/or ulcers.
LECS is indicated for gastric GIST with tumor size <50 mm in diameter, regardless of the tumor location, according to the GIST resection guidelines suggested by the National Comprehensive Cancer Network [9].
LECS has demonstrated no mortality and a low incidence of postoperative complications. There are no previous reports of endocarditis associated with LECS. We suggest that the prolonged efforts at resection of the GIST by LECS resulted in a bacteremia and led to the development of endocarditis on an abnormal mitral valve. Physicians need to be aware of endocarditis as a potential complication of LECS. As with any new procedure there is a learning curve and this case demonstrates that not everything new is necessarily better.
References
- Rubin BP, Heinrich MC, Corless CL. Gastrointestinal stromal tumour. Lancet. 2007; 36: 1731-1741.
- Choi SH, Chung JW, Lee EJ, Kim TH, Lee MS, Kang JM, Song EH, Jun J-B,et al. Incidence, characteristics, and outcomes of Staphylococcus lugdunensis bacteremia. Journal of Clinical Microbiology. 2010; 48: 3346-3349.
- Non LR, Santos CAQ. The occurrence of infective endocarditis with Staphylococcus lugdunensis bacteremia: A retrospective cohort study and systematic review. Journal of Infection. 2017; 7: 179-186.
- Nesher L, Tarrand J, Chemaly RF, Rolston KV. Staphylococcus lugdunensis infections, filling in the gaps: a 3-year retrospective review from a comprehensive cancer center. Supportive Care in Cancer. 2017; 25: 1063-1069.
- Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, Bolger A, Cabell CH, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: A guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the C. Circulation. 2007; 116: 1736-1754.
- Nishida T, Hirota S, Yanagisawa A, Sugino Y, Minami M, Yamamuru Y, Otani Y, Shimada Y, et al. Clinical practice guidelines for gastrointestinal stromal tumor (GIST) in Japan: English version. International journal of clinical oncology. 2008; 13: 416-430
- Hu J, Or BHN, Hu K, Wang ML. Comparison of the post-operative outcomes and survival of laparoscopic versus open resections for gastric gastrointestinal stromal tumors: A multi-center prospective cohort study. International Journal of Surgery. 2016; 33: 65-71.
- Kim GH, Choi KD, Gong CS, Lee I-s, Park YS, Han M, Na HK, Ahn JY , et al. Comparison of the treatment outcomes of endoscopic and surgical resection of GI stromal tumors in the stomach: a propensity score-matched case-control study. Gastrointestinal endoscopy. 2020; 91: 527-536.
- Hiki N, Yamamoto Y, Fukunaga T, Yamaguchi T, Nunobe S, Tokunga M, Miki A, Ohyama S, et al. Laparoscopic and endoscopic cooperative surgery for gastrointestinal stromal tumor dissection. Surgical endoscopy. 2008; 22: 1729-1735.