
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Unilateral colonization of fungal infection presenting as renal mass in young patient: A case report
Mahabuba Shirin*; Salahuddin Al-Azad; Farzana Alam; Anil Yadav
Department of Radiology & Imaging, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh.
*Corresponding Author: Mahabuba Shirin
Associate Professor, Department of Radiology & Imaging, Bangabandhu Sheikh Mujib Medical University
(BSMMU), Dhaka, Bangladesh.
Email: m.shirin1970@gmail.com
Received : Sep 23, 2021
Accepted : Nov 17, 2021
Published : Nov 24, 2021
Archived : www.jcimcr.org
Copyright : © Shirin M (2021).
Abstract
Fungal ball or fungal bezoar is the saprophytic colonization of a preformed cavity by a conglomerate of fungal mycelia without invasion of the adjacent tissue. Fungal bezoar is seen commonly in immunocompromised individuals. We present a case of urinary tract infection, complicated by unliateral fungus balls in a 25-year old female whose imaging findings (USG and CT scan), laboratory investigation and histopathological findings are consistent with renal fungal ball.
Keywords: fungal ball; urinary tract infection.
Citation: Shirin M, Al-Azad S, Alam F, Yadav A. Unilateral colonization of fungal infection presenting as renal mass in young patient: A case report. J Clin Images Med Case Rep. 2021; 2(6): 1421.
Introduction
Primary urinary tract infection due to Candida is usually seen in patients with immunocompromised risk factors such as diabetes mellitus, prior antibiotic therapy urinary tract drainage devices, urinary tract pathology and malignancy.
Candida albicans is a ubiquitous fungus and can be detected in approximately 32-55% of health individuals [1]. Infection of urinary tract by C. Candida can be from blood or retrograde infection [2]. Candidiasis can occasionally present as mass lesions. Localized renal Candida infection is rare. It can be a renal fungal ball, or rarely can Candida renal infection present as a granulomatous pyelonephritis [3,4]. In this report, we described a renal candidiasis in a 25-year-old patient presenting as a fungal bezor.
Case report
A 25- year old female presented with complaints of recurrent UTI for 10 yrs and painless hematuria for 3 yrs. She was unresponsive to prolonged antibiotic use since 10 years. Urinalysis showed hematuria, with 10-20 white blood cells per high power field, but a urine culture was negative.
Ultrasonography showed a mixed echogenic mass lesion involving mid & lower polar calyces and renal pelvis of right kidney measuring about 4.8.5 X 3.83 cm (Figure 1). On color Doppler ultrasonogram no blood flow is seen in the mass lesion (Figure 2). Plain CT imaging of the abdomen confirmed the presence of mass in the mid &lower polar calyx and renal pelvis associated with ipsilateral pelvic dilatation. And remaining part of the ureter is not dilated (Figure 3). Left Kidney was normal. The mass contained no visible calcification, involved the renal capsule, and infiltrated the perinephric fat. Renal veins are normal in caliber. No lymphadenopathy was noted.

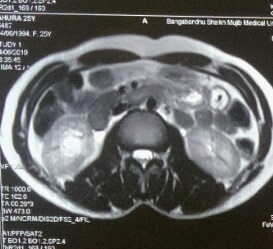
MR urogramT2W axial showed heterogeneously hypertintense lesion measuring about AP 2.2 X TD X 2.6 x CC 3.1 was noted at mid and lower polar calyx and renal pelvis of right kidney causing mild dilatation of involved part but remaining pelvi-calycael was not dilated (Figure 4). The right kidney appears normal in size, shape and position.

Ureteroscopy was done which reveals a polypoid lesion at the right renal pelvis.
Histopathology findings were compatible with a renal aspergilloma. No malignancy was seen.
As per clinical information and imaging findings are consistent with right renal fungal ball.
Discussion
Upper urinary tract fungal infections are relatively uncommon. Literature review reveals that renal involvement is commonly caused by disseminated candidiasis, but a primary infection can be caused by an ascending process or via urinary catheter drainage [5]. It can affect the renal parenchyma or the drainage system and cause a cortical abscess or an obstructive intrarenal mass, commonly in the pelviureteric junction [6]. It can present as renal colic, fever, dysuria, chills, vomiting or decreased urine output, and the age at presentation can vary from newborn to elderly [7].
Majority of the cases described in the literature suggests that diabetes, immunosuppressed state, bladder catheterization and prolonged antibiotic use are a few of the high risk factors for opportunistic infection by fungus. Aspergillus, Mucormycetes, Cryptococcus and Histoplasma are other organisms known to infect the urinary system [8]. A case of renal fungal ball with Geotrichumcandidum has been reported in a post-partum patient [9]. G. candidum infection has been reported commonly in renal transplant recipients.
Conclusion
The kidney is a common site of end-organ disease in disseminated candidiasis, with a variety of clinical manifestations including abscess (solitary or multiple), pyelonephritis, and fungal bezoar in the renal pelvis causing obstruction. Large doses of the Candida led to multisystem disease with a poor prognosis. Smaller doses, however, created low-grade disease in organs such as the kidney, where chronic renal atrophy and fungal ball formation were observed.
Ultrasonography is essential to rule out a fungal bezoar in the renal pelvis that could result in obstruction. If a fungus ball is present, percutaneous nephrostomy is recommended. Percutaneous nephrostomy definitively relieves obstruction and prevents ongoing parenchymal insult, provides a “clean” specimen and an accurate diagnosis of the fungal infection, and allows treatment of the infection with local instillation therapy complementing systemic therapy
References
- Stenderup. Ecology of yeast and epidemiology of yeast infections. Acta Dermato-Venereologica. 1986; 66: 27–37.
- Fisher JF, Kavanagh K, Sobel JD, Kauffman CA, Newman CA. Candida urinary tract infection: pathogenesis. Clinical Infectious Diseases, vol. 52, supplement. 2011; 6: S437–S451, 2011.
- Korkes, Favoretto RL, Bróglio M, Silva CA, Castro MG, Perez MDC. “Xanthogranulomatous pyelonephritis: clinical experience with 41 cases,” Urology. 2008; 71: 178–180, 2008.
- Özdemir BH, Sar A, Uyar P, Suren D, Demirhan B. “Posttransplanttubulointerstitial nephritis: clinicopathological correlation. Transplantation Proceedings. 2006; 38: 466–469.
- Kawashima Sandler CM, Goldman SM, Raval BK, Fishman EK. CT of renal inflammatory disease. Radiographics 1997; 17: 851–66.
- Kale H, Narlawar RS, Rathod K. Renal fungal ball: An unusual sonographic finding. Inc. J Clin Ultrasound. 2002; 30: 178–80.
- Lee SW. An aspergilloma mistaken for a pelviureteral stone on nonenhanced CT: a fungal bezoar causing ureteral obstruction. Korean J Urol. 2010; 51: 216.
- Ahuja A, Aulakh BS, Cheena DK, Garg R, Singla S, et al. Aspergillus fungal balls causing ureteral obstruction. Urol J 2009; 6: 127–9.
- Prakasha PY, Seetaramaiah VK, Thomas J, Khanna V, Rao SP. Renal fungal bezoar owing to geotrichumcandidum. Med Mycol Case Rep. 2012; 1: 63–5.