
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Saber sheath trachea: A radiological sign of severe airway obstruction
Ram Babu Sah*; Ramesh Singh Pal
Department of Pulmonary Medicine, ESI- PGIMSR, Basaidarapur, New Delhi, India.
*Corresponding Author: Ram Babu Sah
Medical Officer, Department of Pulmonary
Medicine, ESI-PGIMSR, Basaidarapur, New Delhi110015, India.
Email: rambabusah1008@gmail.com
Received : Sep 24, 2021
Accepted : Nov 17, 2021
Published : Nov 24, 2021
Archived : www.jcimcr.org
Copyright : © Sah RB (2021).
Abstract
A middle-aged man, chronic smoker, presented with complaints of productive cough & exertional breathlessness (mMRC grade III) for 3 years with frequent episodes of exacerbation in the past. There was no other comorbidity or significant past history. His chest radiograph showed narrowing of trachea. Evaluation with computerized tomography of thorax showed normal extra-thoracic trachea with narrowing of the coronal diameter with increase in the sagittal diameter of the trachea along with thickening and calcification of the tracheal wall seen in saber sheath trachea.
Keywords: forced expiratory volume; tracheal narrowing; saber sheath trachea.
Citation: Sah RB, Pal RS. Saber sheath trachea: A radiological sign of severe airway obstruction. J Clin Images Med Case Rep. 2021; 2(6): 1422
Clinical image description
A middle-aged man, chronic smoker, presented with complaints of productive cough & exertional breathlessness (mMRC grade III) for 3 years. He had frequent episodes of exacerbation in the past. There was no other comorbidity or significant past history. His general physical examination was unremarkable. Examination of respiratory system revealed rhonchi. On other system examination there was no significant findings.
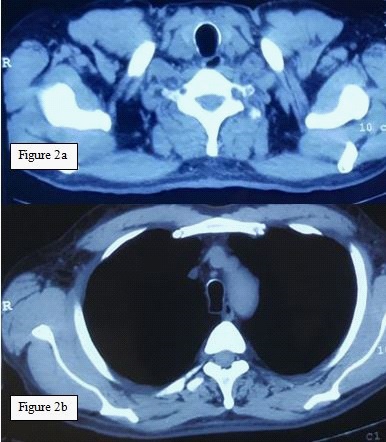
His routine hematological & biochemical tests were normal. Chest radiograph postero-anterior view revealed narrowing of tracheal lumen and hyperinflation (Figure 1). His spirometry showed reduced ratio of forced expiratory volume in one second (FEV1) to forced vital capacity (59.33) with decreased FEV1 - 1.80 Litres (43% of predicted) indicative of severe obstructive abnormality. Further evaluation with high resolution computed tomography (HRCT) of thorax was done, which showed- Normal extra-thoracic trachea (Figure 2a). There was narrowing of the coronal diameter with increase in the sagittal diameter of the trachea along with thickening and calcification of the tracheal wall giving a bullet shape appearance to the trachea (Figure 2b)
Saber-sheath trachea is a fixed deformity of the intra-thoracic trachea, which is characterized by reduction in coronal diameter associated with an increase in sagittal diameter, as conventionally measured 1 cm above the aortic arch. The extrathoracic trachea is normal. When the tracheal index, i.e., ratio of coronal to sagittal diameter is <0.50 diagnosis is considered [1]. It is considered as diagnostic of COPD. The sensitivity of this sign is above 90% but the specificity is below 40% [2]. Sabersheath trachea may provide a clue to the presence of COPD when other radiological signs are absent.
Degeneration and ossification of the cartilage, calcification and bending of the tracheal cartilage to form a rigid noncollapsible trachea, due to repetitive cartilaginous injury from excessive coughing, and elevated intra-thoracic pressure led to development of saber sheath trachea.
Radiography is the modality of choice for diagnosis. Computed tomography can help in delineating the extent of involvement.
There is no specific treatment for this condition. Treatment of underlying disease e.g. COPD is the mainstay of treatment. Air leak can be a major concern if a patient requires intubation.

References
- Marom EM, Goodman PC, McAdam HP. Diffuse abnormalities of the trachea and main bronchi. AJR Am J Roentgenol. 2001; 176: 713-7.
- Tsao TC, Shieh WB. Intrathoracic tracheal dimensions and shape changes in chronic obstructive pulmonary disease. J Formos Med Assoc. 1994; 93: 30-4.