
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Can SARS-CoV-2 infection trigger Parkinson Disease? A case report
Daniel López Domínguez*; Anna Cots Foraster; Berta Solano Vila; Lilian Vivas Villacampa
Movement Disorder Unit. Department of Neurology, University Hospital Doctor Josep Trueta – Santa Caterina Hospital. GironaSalt, Spain. Institut d’Investigació Biomèdica de Girona Dr. Josep Trueta (IDIBGI).
*Corresponding Author: Daniel López Domínguez
Movement Disorder Unit, Department of Neurology,
University Hospital Doctor Josep Trueta, Girona, Spain.
Institutd’InvestigacióBiomèdica de Girona Dr. Josep
Trueta (IDIBGI).
Phone: +34-972-94-02-00
Email: dani89ld@hotmail.com
Received : Oct 04, 2021
Accepted : Nov 22, 2021
Published : Nov 29, 2021
Archived : www.jcimcr.org
Copyright : © Domínguez DL (2021).
Abstract
SARS-CoV-2 infection typically produces respiratory manifestations, although multiple neurological manifestations (seizures, stroke, etc.) have also been reported, it is postulated that SARS-CoV-2 (like most β-coronaviruses), has neurotropic potential.
We present a case of Probable Parkinson’s Disease (PD) after SARSCoV-2 infection.
A 54-year-old male, previously asymptomatic (although, he referred hyposmia for 3 years) presented mild infection (fever, dry cough and anosmia) by SARS-COV-2 (confirmed with positive PCR), with complete recovery after seven days. On the fourteenth day, he developed rest tremor, bradykinesia, and mild rigidity affecting right limbs. Analytical study and brain MRI showed no alterations, DaTSCAN showed asymmetric bilateral putaminal hypocaptation.
The final diagnosis was Probable PD, we started treatment with rasagiline 1 mg/24 h, with good clinical response afterwards.
Post-infectious parkinsonism has been described in relation with different viral agents. In the same way, it has been proposed that SARS-CoV-2 could affect the CNS and trigger a neurodegenerative process and even PD. To date, only four cases have been described worldwide (including the patient we present).
In the case presented, it stands out the asymptomatic state prior to the infection, except for hyposmia (a prodromal symptom of premotor stages of various synucleinopathies). Given the development of parkinsonism two weeks after the onset of respiratory symptoms, we propose that SARS-CoV-2 could have precipitated parkinsonian symptoms in a patient in the premotor phase of PD.
In patients that develop tremor after SARS-CoV-2 infection, a thorough neurological examination should be performed, searching for symptoms suggestive of parkinsonism.
Keywords: SARS-CoV-2; secondary parkinsonism; post-infectious parkinsonism; hypokinetic movement disorders; hyposmia; β-coronavirus.
Abbreviations: PD: Parkinson Disease; CNS: Central Nervous System; PCR: Real time positive quantitative reverse transcription polymerase chain reaction; SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2..
Citation: Domínguez dl, Foraster AC, Vila BS, Villacampa LV. Can SARS-CoV-2 infection trigger Parkinson Disease? A case report. J Clin Images Med Case Rep. 2021; 2(6): 1433.
Introduction
In December/2019 began the outbreak of the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), with rapid worldwide expansion, persisting until the present time [1]. According to World Health Organization data, there have been 185,291,530 confirmed cases, including 4,010,834 deaths.
SARS-CoV-2 infection usually produces fever, cough, dyspnea and other respiratory manifestations [2]. Different authors propose that SARS-CoV-2 and most β-coronaviruses have neuroinvasive potential, and although the physiopathology is still unknown [3], multiple neurological manifestations have been reported in the context of SARS-CoV-2 infection including hyposmia, seizures, stroke, headache, etc.
On the other hand, Parkinson Disease (PD) is the second most frequent neurodegenerative disease, behind Alzheimer’s Disease, affecting 6.2 million patients worldwide. The high prevalence of hyposmia in patients with SARS-CoV-2 infection raised theories about possible parkinsonian symptoms secondary to this infection, similar to the supposed link between Lethargic Encephalitis and Spanish flu [2] in the 1920s (although still highly controversial).
We report a case of Probable PD after SARS-CoV-2 infection.
A 54-year-old right-handed male, with no personal history of interest and no family history of PD, developed in October/2020 fever, fatigue, myalgias, diarrhea, dry cough and anosmia. Real time positive quantitative reverse transcription polymerase chain reaction (PCR) test for SARS-COV-2 performed by nasopharyngeal swab resulted positive, so SARS-CoV-2 infection was diagnosed. Given the mild symptomatology, he didn’t require hospital admission, and recovered after seven days of clinical debut. At the fourteenth day, he noticed rest tremor affecting the upper right limb, micrographia and greater difficulty in performing precision tasks, with progressive worsening for the next six months. When questioned about it, the patient also reported three years evolution of hyposmia, which worsened during SARS-CoV-2 infection. He didn’t refer REM sleep behavior disorder, constipation or depression.
On examination, we observed pronation-supination rest tremor, with low frequency (4-5 Hzs) and moderate amplitude, mild bradykinesia and cogwheel rigidity, all of them involving the right limbs. There was a decrease of arm swing and ipsilateral rest tremor while walking. On pull test no retropulsion was observed. No cognitive decline was found (Mini-Mental State Examination of 30/30). The rest of the neurological examination was normal.
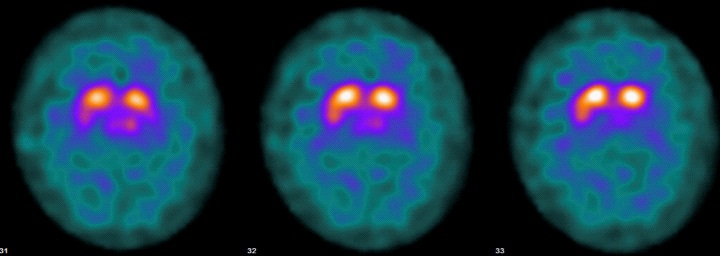
Analytical studies were normal. Brain MRI showed no alterations [1-3]. I-Ioflupane DaT-SPECT showed bilateral asymmetric putamen hypocaptation, with left predominance (Figure 1).
Final diagnosis was Probable PD, fulfilling the Movement Disorders Society Unified PD Rating Scale criteria. We started treatment with rasagiline 1 mg/24 hrs, showing good clinical response that persists up to date, three months later.
Post-infectious parkinsonian symptoms have been described in association with different viral agents (Influenza-A, EBV, VZV, etc.) [4,5].Given its possible neurotropic capacity, some authors have proposed that SARS-CoV-2 and other coronaviruses are capable of affecting the CNS, hypothesizing the olfactory bulb as an entry route, producing direct structural damage of the nigrostriatal system and/or acting as a trigger for an inflammatory response that could generate a neurodegenerative process [4,5].
On the other hand, clinical worsening of chronic neurodegenerative diseases, like PD, in the context of SARS-CoV-2 infection has been reported, possibly associated to these neurotropic properties. The possibility of precipitating motor symptoms in premotor phase PD has not been previously considered, although it seems plausible.
To date, in addition to our patient, three cases of probable PD during the course of SARS-CoV-2 infection have been described [1,4,5]. As in our case, all of them showed DaT-SCAN with presynaptic affection, without lesions at the brain MRI, and at least two of the cases were non-post-encephalitic [4,5].
Our case was asymptomatic prior to SARS-CoV-2 infection (confirmed by relatives and the physicians who had previously examined him), with the only exception of hyposmia (described as a possible prodromic symptom in pre-clinical stages of PD and other synucleinopathies). He developed parkinsonian symptoms two weeks after the onset of respiratory symptoms. We propose three possible explanations:
1. SARS-CoV-2 could have precipitated parkinsonian symptoms in a premotor phase patient, given the presence of hyposmia years before the infection.
2. SARS-CoV-2 could have triggered a central neurodegenerative process, as has been suggested before [1,3-5]. However, none of the described cases in the literature showed structural lesions on neuroimaging, and CSF studies usually showed no alterations.
3. Chance occurrence of SARS-CoV-2 infection and PD. Given the high prevalence of both pathologies, this option cannot be ruled out, although all of the published cases were relatively young for PD (the oldest patient was 58 years old) and clinical debut was clearly after the infection.
In any case, more information is needed to draw more weighty conclusions
The neurological consequences produced by SARS-CoV-2 infection in the short and long term are still unknown, and the neurological symptoms derived from this new condition are continuously updated. In patients that develop tremor after SARS-CoV-2 infection, a thorough neurological examination should be performed in search of symptoms suggestive of parkinsonism.
References
- Antonio Méndez-Guerrero; María Isabel Laespada-García; Adolfo Gómez-Grande; Mariano Ruiz-Ortiz; Víctor Antonio BlancoPalmero and Francisco Javier Azcarate-Diazet al. Acute hypokinetic-rigid syndrome following SARS-CoV-2 infection. Neurology. 2020.
- David Sulzer, Angelo Antonini, Valentina Leta, Anna Nordvig, Richard J. Smeyne and James E. Goldmanet al. COVID-19 and possible links with Parkinson’s disease and parkinsonism: from bench to bedside. npj Parkinson’s Disease 6, article number 18 (2020), 2020.
- Wei-Shan Li, Ling-Ling Chan, Yin-Xia Chao & Eng-King Tan. Parkinson’s disease following COVID-19: causal link or chance occurrence? Journal of Translational Medicine 18, article number 493 (2020). 2020.
- Roni Eichel, Bettina Steiner-Birmanns, Amir Janah, Maxim Ioshpa and Rachel Bar-Shalom et al. A case of probable Parkinson’s disease after SARS-CoV-2 infection. The lancet Neuirology Vol 19, 2023. Coronavirus Disease 2019 and Parkinsonism: A Nonpostencephalitic Case.
- Ingrid Faber, Pedro R.P. Brandao, Fiorella Menegatti, Diógenes D. de Carvalho Bispo, Fernando B. Maluf, and Francisco Cardoso. Coronavirus Disease 2019 and Parkinsonism: A Non-postencephalitic Case. Movement Disorders. 2020.