
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Vertebrobasilar and anterior cerebral circulation dolichoectasia in a 67-year-old woman presenting as stroke
Omolola M Akinwunmi
Department of Radiology, College of Medicine, University of Ibadan, Oyo State, Nigeria.
*Corresponding Author: Omolola M Akinwunmi
Department of Radiology, College of Medicine, University of Ibadan, Oyo State, Nigeria.
Email: omololakinwunmi@gmail.com
Received : Oct 05, 2021
Accepted : Nov 23, 2021
Published : Nov 30, 2021
Archived : www.jcimcr.org
Copyright : © Akinwunmi OM (2021).
Abstract
Background: Dolichoectasia is an anomalous condition of the blood vessels that arise due to architectural abnormalities in the weakened walls.
Case description: This is a case of a 67-year-old woman being managed for chronic hypertension who initially presented with features of left hemispheric stroke. Neurovascular imaging revealed dolichoectasia of both the vertebrobasilar and anterior cerebral circulations.
Conclusion: This clinical scenario is peculiar because simultaneous affectation of both vascular territories is extremely rare. Management of her condition was a diagnostic dilemma due to the rarity of her pathology and the low-resource setting of our environment.
Keywords: dolichoectasia; vertebrobasilar; anterior cerebral circulation
Citation: Akinwunmi OM. Vertebrobasilar and anterior cerebral circulation dolichoectasia in a 67-year-old woman presenting as stroke. J Clin Images Med Case Rep. 2021; 2(6): 1438.
Introduction
Dolichoectasia, sometimes known as dilative arteriopathy, derives its name from a Greek word, “dolichos” which means long, and “ektasis” meaning elongation. It usually affects the vertebral and basilar arteries. The involvement of the anterior circulation is uncommon, with a combination of both being rare [1].
It has a male preponderance [2]. Dolichoectasia is associated with atherosclerosis, dyslipidemia, congenital anomalies in internal elastic fibers of the endothelium (Ehler-Danlos syndrome, Marfan syndrome), and chronic systemic hypertension [3]. Other risk factors such as increasing age, male sex, and previous history of myocardial infarction have been identified [4,5].
Intracranial dolichoectasia may cause compression of adjacent soft tissue structures such as cranial nerves and brainstem. This may lead to hemifacial paresis, spasm, trigeminal neuralgia, or brainstem dysfunction [1]. Intracranial bleed is another complication that could occur due to rupture of the weak endothelium of the affected vessels that is often life-threatening. It may also cause cerebral infarction due to thrombosis, embolism, or occlusion of deep penetrating arteries [6].
This case report is on a 67-year-old woman with extensive dolichoectasia of the right anterior and posterior cerebral circulation arteries who presented with sudden onset right hemiparesis (stroke-like symptoms) of 8 hours duration at a tertiary teaching hospital in Nigeria. The rarity, extent, and characteristic radiological features of this pathology prompt the presentation of this case.
Case report
O. F was a 67-year-old business woman who presented with sudden onset weakness of the right upper and lower limbs for 8 hours at the Accident and Emergency Unit. It occurred just after taking her bath. She had no history of headache, head trauma, loss of consciousness, or seizure. She was diagnosed with systemic hypertension 30 years ago and was compliant with her antihypertensive medications until four months before her presentation. She had been managed for paroxysmal ventricular tachycardia and hypertensive heart disease by the Cardiology Unit of the hospital. She had a history of transient ischemic attack (TIA) six years earlier, but no radiological investigation was done at that time. She also had hyperlipidemia eight months earlier but was yet to commence medications. She neither smoked cigarettes nor drank alcohol. Her family history was not contributory.
Her neurologic examination showed reduced power in the right upper and lower limbs (power= grade 4). The review of other systems was unremarkable. An assessment of a left hemispheric stroke, likely hemorrhagic, involving the left middle cerebral artery territory was made. Her laboratory tests revealed lipid abnormalities such as total cholesterol of 400 mg/dl, LDL of 345 mg/dl, and triglycerides of 250 mg/dl. These were all consistent with her hyperlipidemic status.
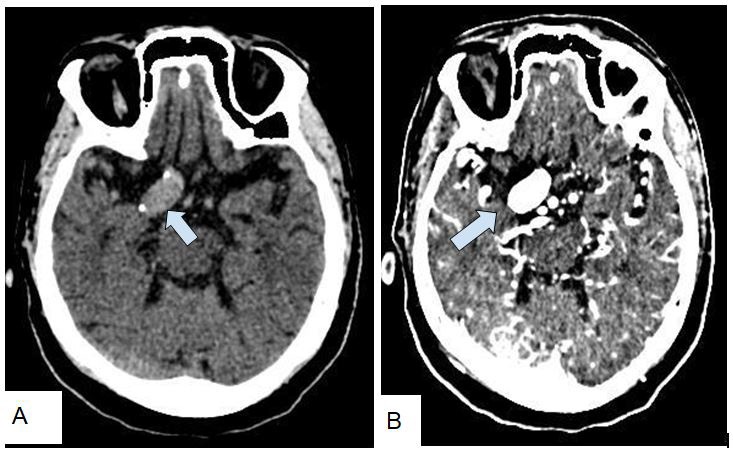
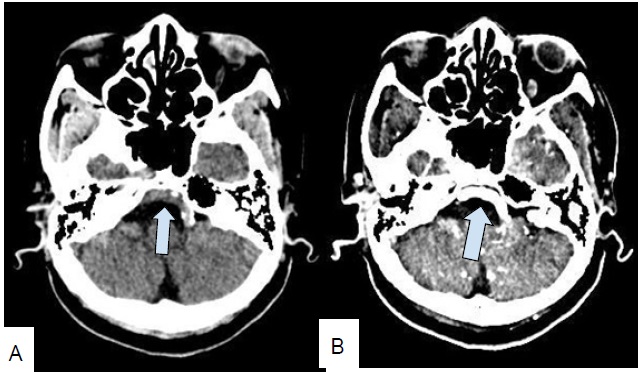
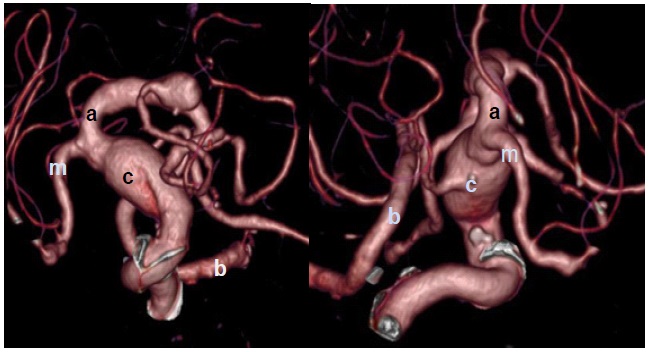
She was subsequently admitted into the hospital by the Neurology team. Due to financial constraints and inadequate health insurance coverage, there was a delay in carrying out the requested cranial Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) examinations. The cranial CT angiography (CTA) done five days after admission demonstrated extensive atheromatous plaques in the intracranial portion of the right internal carotid artery (Figure 1A) and the basilar artery (Figure 2A) on the pre-contrast images. The post-contrast images showed an extensive and marked dilation of these vessels (Figures 1B and 2B). No thrombus was within them. The 3-D reconstructed images of the CTA showed severe fusiform dilation, deformity, superior displacement, and tortuosity of these vessels (Figure 3). The basilar artery was displaced laterally to the right of the pons, and it showed a serpentine course. The intracranial portion of the right internal carotid artery and basilar artery measured 1.27 cm and 0.48 cm, respectively, in their widest diameters. The left anterior and middle cerebral arteries were within normal limits. There was no sub-arachnoid hemorrhage, intracranial collection, or area of brain infarction. The brain magnetic resonance imaging (MRI) confirmed these markedly dilated vessels as signal void structures. They showed avid homogeneous contrast enhancement on post gadolinium images. She also had mild to moderate periventricular white matter changes on fluid-attenuated inversion recovery (FLAIR) images. Based on these findings, the diagnosis of extensive dolichoectasia involving both the anterior circulation (right anterior and middle cerebral arteries and intracranial portion of right internal carotid artery) and posterior circulation (right vertebral and basilar arteries) was made.
The patient immediately commenced medical treatment that included antihypertensive drugs, oral hypolipemic agents, and intravenous hydration. The possibility of her having surgery was discussed but the severity of her condition and prognosis were considered. Her GCS however rapidly deteriorated over the next seven days with the power on the right limbs reducing to zero. Based on this, an assessment of a repeated left hemispheric stroke was made. She subsequently developed respiratory distress and clinically deteriorated after five days. She was admitted into the Intensive Care Unit (ICU) due to repeated episodes of cardiac arrest. She, unfortunately, died two days later.
Discussion
Intracranial dolichoectasia is a rare disorder of the blood vessels of uncertain pathogenesis. It is characterized by dilation/ widening, elongation, and tortuosity of the arteries [7]. It usually affects the vertebrobasilar system. However, simultaneous involvement of the anterior and posterior circulations, as reported in this patient, is very rare [7].
The true prevalence of dolichoectasia is unknown in this environment. A case of dolichoectasia of the vertebrobasilar system was reported earlier at Ahmadu Bello University [4]. The rarity of this pathology in our environment may be attributable to the reduced frequency of autopsies [4].
There are three sub-types of dolichoectasia identified. These include the atherosclerotic, non-atherosclerotic, and dolichoectatic type secondary to an arterial dissection [2]. This patient had an atherosclerotic sub-type due to the extensive atheromatous plaques seen in the cerebral vessels.
Histological studies in the literature showed the presence of background disruption and thinning of the internal elastic fibers and intima-media of the cerebral vessels [7]. As the architecture of the connective tissue is damaged, the vessel wall is no longer able to hold its original conformation. It begins to unravel to form an elongated and tortuous course to with stand the higher systemic blood pressure [3].
The blood flow within the dilated arteries becomes both retrograde and orthograde flow within the same arterial segment predisposing to recurrent thrombus formation [8].
Dolichoectasia may also co-exist with the following diseases: autosomal dominant inherited polycystic kidney disease, sickle cell anemia, Fabry’s disease, and AIDS that were not present in this patient [9].
Multiple risk factors are associated with dolichoectasia. These include chronic systemic arterial hypertension, hyperlipidemia, and extensive atherosclerosis that were all identified in this patient [6,10,11].
The clinical features vary [8]. They could be asymptomatic, present with symptoms associated with compression of adjacent nerve/ brain structures, or present with TIAs or stroke-like symptoms as observed in this patient. They could also present with headache, vertigo, pulsating tinnitus, hemifacial paresis, vision disturbance, and signs of cranial nerve impairment [12]. Some patients develop complications of dolichoectasia caused by hemodynamic disturbance such as cerebral ischemia. Other complications include hydrocephalus or ischemic/ hemorrhagic stroke. The worst complication is the massive subarachnoid hemorrhage as documented by Mohammed et al [4]. This, unfortunately, led to the death of our patient.
Traditionally, dolichoectasia was diagnosed with catheter angiographic studies because interventional procedures could be done simultaneously [7,12]. With the advent of brain CTA and MRA, dolichoectasia can be diagnosed non-invasively. Potential advantages of brain CTA over MRA include faster acquisition times, fewer limitations on patient selection, and reduced morbidity and mortality [10]. It, however, does not provide information about the directionality of flow, unlike brain MRA. Brain MRA, using the time of flight sequence, is non-invasive and nonionizing. It displays the vascular anatomy, the relationship of arteries to the posterior fossa, visualization of mural thrombus dissection, as well as pathological changes in the brain parenchyma without the use of contrast media [9].
Radiographic criteria for diagnosing dolichoectasia on angiography include a diameter of basilar artery >4.5 mm [13,14], diameter of internal carotid artery >6.3 mm; >10 mm deviation of the course of basilar artery from the perpendicular line drawn from its bifurcation to its origin; origin of the basilar artery at the level of pontomedullary junction and bifurcation of the basilar artery above the suprasellar cistern [7,15]. The ectatic vessels identified in this patient showed similar dimensions and morphology. The “S” shaped aneurysm of the vertebrobasilar system described by Drakes and Peerless is similar to the serpentine course of the basilar artery noted on the 3-D reformatted CTA image in this patient [11].
Dolichoectasia of the intracranial arteries is usually treated conservatively if less extensive and not complicated by intracranial bleeding. This includes anticoagulation therapy and management of arterial hypertension. The endovascular intervention of dolichoectasia via Interventional Radiology is adopted in selected cases of patients. This includes proximal occlusion, direct clipping, resection with re-anastomosis, transposition, aneurysmorrhaphy with thrombectomy, and coil-assisted stent reconstruction [7]. However, in this patient, optimal medical care delivery was hampered largely due to the extent and severity of her condition coupled with insufficient funding in our health care system.
Conclusion
Intracranial dolichoectasia is a rare vascular anomaly of the cerebral vessels which often are asymptomatic for a long time and diagnosed incidentally. The clinical presentation may mimic stroke or intracranial space-occupying lesions. Thus a high index of suspicion, detailed clinical history, and neurological evaluation are essential for prompt diagnosis. All patients with stroke or stroke-like symptoms should be evaluated properly with appropriate radiological imaging to diagnose the underlying etiology and forestall preventable morbidities and mortalities from conditions like dolichoectasia in our environment. Prophylactic cardiological examination and cranial CTA/ MRA in patients with dolichoectasia are recommended for successful management.
In summary, this is a case of a 67-year-old woman who presented with stroke-like symptoms. She was diagnosed with extensive dolichoectasia of the anterior and posterior cerebral circulations. She, unfortunately, died after suffering from a repeated left hemispheric stroke and cardiac arrest.
References
- Kwon HM, Lee Y.S. Dolichoectasia of the intracranial arteries. Curr Treat Options Cardiovasc Med. 2011; 13: 261- 267.
- Nakamura Y, Hirayama T, Ikeda K. Clinicoradiologic features of vertebrobasilar dolichoectasia in stroke patients. J Stroke Cerebrovasc Dis. 2012; 21 (1): 5- 10
- Passero, Stefano, G.; Rossi, Simone. Natural history of vertebrobasilar dolichoectasia. Neurology. 2008; 70: 66-72.
- Mohammed A, Maisamari S.J. Apparently asymptomatic atherosclerosis of the vertebrobasilar arteries. Annals Afr Med. 2006; 5: 212- 213.
- Pico F, Labreuche J, Touboul P.J. Intracranial arterial dolichoectasia and its relation with atherosclerosis and stroke subtype. Neurology. 2003; 61: 1736–1742.
- Ince B, Petty G.W, Brown R.D, Chu C.P, Sicks J.D, Whisnant J.P. Dolichoectasia of intracranial arteries in patients with first ischemic stroke- a population-based study. Neurology. 1998; 50: 1694- 1698.
- Sung-Joo Y, Fahad A, Howard L. Dolichoectasia of the vertebral basilar and internal carotid arteries: A case report and literature review. Surg Neurol Int. 2013; 4: 153.
- Titlic M, Tonkic A, Jukic I, Kolic K, Dolic K. Brastis Lek Listy. 2008; 109: 528- 530.
- Boguslawa B, Olga K, Maciei G, Marek S. Dolichoectasia of the circle of Willis arteries and fusiform aneurysm of basilar arteryA case report and review of the literature. Pol J Radiol. 2012; 77: 54- 59.
- Vieco P.T, Shuman W.P, Alsofrom G.F, Gross C.E. A comparison of CT angiography and digital subtraction angiography in the detection of the circle of Willis aneurysms in patients with acute subarachnoid hemorrhage. AJR Am J Roentgenol. 1995; 165: 425- 430.
- Drake C.G, Peerless J.S. Giant fusiform intracranial aneurysms: a review of 120 patients treated surgically from 1965 to 1992. J Neurosurg. 1997; 87: 141–62.
- Vieco P.T, Maurin EE, Gross CE. Vertebrobasilar dolichoectasia: Evaluation with CT Angiography. AJNR. 1997; 18: 1385–1388.
- Borota L, Jonasson P. Basilar and bilateral carotid dolichoectasia with spontaneous dissection of C2 segment of the internal carotid artery. AJNR. 2006; 27: 1241- 1244.
- Kalimo H, Kaste M, Haltia M. Dolichoectasia and fusiform aneurysms. In: Graham DI, Lantos PL, eds. Greenfield’s neuropathology. 7th ed. London: Arnold Publishing; 2002; 281–355.
- Ubogu E.E, Zaidat O.O. Vertebrobasilar dolichoectasia diagnosed by magnetic resonance angiography and risk of stroke and death: A cohort study. J Neurol Neurosurg Psychiatry. 2004; 75: 22-6.