
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Anesthesia management in a Down syndrome patient with difficult intubation: Case report
Sogol Asgari; Hamidreza Azizi Faresani; Hamideh Ariannia; Faranak Behnaz*
Anesthesiology Department, ShohdaTajrish Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Faranak Behnaz
Associate, Anesthesiology Department, Shohda Tajrish
Hospital, Shahid Beheshti University of Medical
Sciences, Tehran, Iran.
Email: faranak.behnaz@gmail.com
Received : Oct 13, 2021
Accepted : Nov 25, 2021
Published : Dec 02, 2021
Archived : www.jcimcr.org
Copyright : © Behnaz F (2021).
Abstract
Down syndrome is the common chromosomal abnormality and involves multiple organs. So cardiac and respiratory examinations and management of anesthesia in the patients with this syndrome are essential. Also cardiac and respiratory complications intraoperatively are common. Our case is a 11-year-old patient with Down syndrome who underwent atlas and axis cervical subluxation surgery (C1-C2).
The purpose is to evaluate the anesthesia management in a patient with Down syndrome and to pay attention to the intubation and its complications.
Keywords: anesthesia management; Down syndrome; difficultintubation.
Citation: Asgari S, Faresani HA, Ariannia H, Behnaz F. Anesthesia management in a Down syndrome patient with difficult intubation: Case report. J Clin Images Med Case Rep. 2021; 2(6): 1450.
Introduction
Down syndrome is the most common genetic disorder affecting more than 1 in 1,000 live births Patients with Down syndrome have several congenital anomalies that affect almost all organs such as skull, the face, upper respiratory tract, cardiovascular and gastrointestinal tract [1]. Weak ligaments or skeletal abnormalities, leading to neurological disorders such as quadriplegia are known as one of the most critical considerations of anesthesia [2]. Diagnosing and managing Atlantoccipital instability in patients with Down syndrome is a challenging problem in anesthesia. The risk of spinal cord injury during anesthesia is unknown [3].
Case presentation
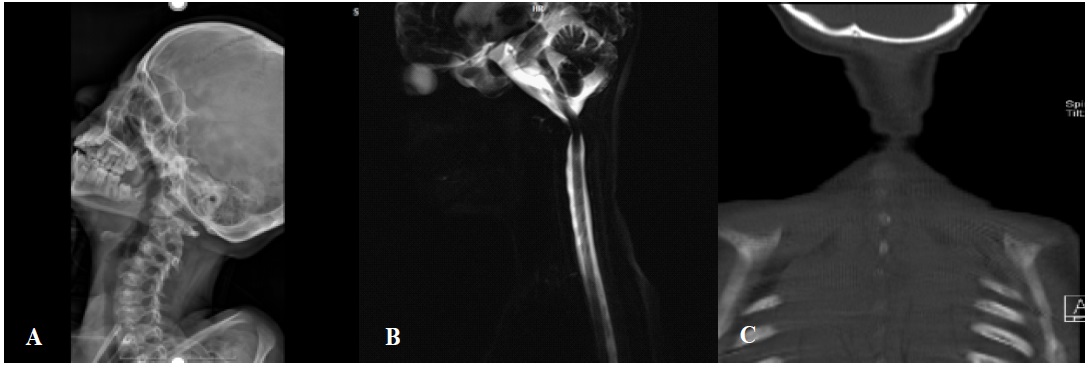
An 11-year-old and 26 Kg weigh child with a Down syndrome history was transferred to an operating room to fix the first and second cervical vertebral dislocations. The patient had no history of heart problems, hypothyroidism, liver and kidney problems, and other disorders. He did not have pulmonary hypertension on echocardiography. On airway examination he had a large tongue, improper teeth, small nose and limited neck movement (figure 1). The patient had no previous history of surgery. He was awake and answered the questions. Hemodynamics and respiration were stable. (HR=120-SPO2=97% -BP=100/50).
Laryngoscope and Video laryngoscope with different blades, Boogie, endotracheal tube in several sizes, laryngeal mask and suction device were prepared.
The patient had an intravenous line (IV) catheter 18 gague. At first, the patient was pre-oxygenated with 100% oxygen for 5-6 minutes at a rate of 5-6 liters per minute that level spo2 Reached 100%.
Induction of anesthesia with midazolam 0.5 mg, fentanyl 50 μg, Nesdonal 80 mg and Atracurium 20 mg was done. Then the patient with videolaryngoscope and spiral tube No 5.5 without opening the neck collar and without moving the neck was intubated. End tidal CO2 was confirmed by capnography.
During the operation, an intravenous catheter was inserted due to the possibility of bleeding. Intraoperative monitoring was done by measuring heart rate, temperature, blood pressure and pulse oximetry. Maintenance of Anesthesia was continued with 4 liters per minute 50% oxygen and isoflurane 1% and atracurium 2 mg and 15-20 cc/kg fluid therapy (normal saline). Intraoperative bleeding was about 350 cc, which was compensated by giving a packcell.
Atrial Blood Gas (ABG) was taken two times, which was normal. The surgery longed about 4 hours. The patient is awake and with stable hemodynamics was transferred to recovery and after about 2 hours he was transferred to ICU.
Discussion
In patients with Down Syndrome airway management is difficult due to macroglossia and a narrow hypopharynx. Macroglossia and pharyngeal muscle hypoten cause to block the upper airways. The trachea may be smaller than normal children. Subglottic stenosis is also more common in these people. In 30- 60% of patients, irregular sleep-breathing and obstructive sleep apnea is seen. These patients are at risk for congenital heart disease. Pulmonary hypertension can be caused by heart disease or chronic obstructive sleep apnea. A cardiovascular assessment and pulmonary hypertension should also be performed [4,5]. They are also at risk for atlantoaxial instability.
Preoperative assessment
In physical examination, it should be checked range of motion and tenderness of neck, abnormal gait, weakness, increased tendon deep reflexes, positive Babensky reflex and lower limb clonus.
If there is a suspected history of spinal cord compression, elective surgery should be delayed.
In these patients, the goal is to minimize head and neck movement. So various skills and tools should be considered for airway management during ventilation [6].
Polysomnography should be performed before anesthesia for evaluation of the severity of obstructive sleep apnea [7].
Depending on the child's condition and the type of operation, premedication is necessary. So it is recommended midazolam 0.5 mg/kg orally 15-20 minutes before surgery. Also for patients with behavioral problems, muscle ketamine 1-2 mg/kg is possible [7].
Anesthesia management
To prevent pharyngeal collapse, constant positive pressure by pulling the jaw (Jaw thrust) is recommended. In these patients, predominant parasympathetic response or abnormal sympathetic response can lead bradycardia. They sometimes do not respond to atropine [4]. Inhalation induction is desirable due to minimal airway irritation but increases the incidence of bradycardia. Depending on the patient's hemodynamics, it may be necessary to reduce the concentration of Sevoflurane [7,8].
Preparations for upper airway obstruction with oral airway reduce the risk of induction-induced hypoxia. A smaller mask or endotracheal tube should be available in patients with subglottic laryngeal stenosis to reduce airway trauma risk. Titrated narcotics can be used to control pain during the surgery. Complementary drugs, such as acetaminophen and non-steroids, can help reduce the dose of narcotics. These patients should be monitored in recovery room and then transferred to ICU [7,9].
Conclusion
Consulting with a pediatric cardiologist will reduce complications and mortality. The most common preoperative complications include airway obstruction and bradycardia. Preoperative considerations to prevent hypoxia and airway obstruction are necessary. A systemic examination, focusing on airway, respiratory tract and cardiac systems, is important before surgery.
Declarations
Conflict of interest disclosures: The authors declare that they have no conflict of interest.
References
- HALL J. Chromosomal Clinical Abnormalities”–in Nelson WE– Nelson Textbook of Pediatrics, 15th ed.
- Roizen MF. Anesthetic implications of concurrent diseases. Miller’s anesthesia. 2005; 1100-3.
- Moldoveanu GG, Severin E. Anesthetic Management of a Down Syndrome Patient with Subocclusive Syndrome. Maedica. 2018; 13(2): 159.
- Holzman RS, Mancuso TJ, Polaner DM, editors. A practical approach to pediatric anesthesia. Lippincott Williams & Wilkins; 2008.
- Y, Imai K, Ohyama Y, Fukayama H, Shinozuka O. Oral management of a patient with down syndrome and agammaglobulinemia: A case report. BMC oral health. 2020; 20(1): 1-5.
- EI-Khoury GY, Clark CR. Dietz FR, Harre RG, Tozzi JE, Kathol MH: Posterior atlantooccipital subluxation in Downs syndrome. Radiology. 1986; 159 : 507-9.
- Lewanda AF, Matis off A,Revenis M ,Harahsheha,Futterman C ,etal.Preoperative evaluation and comprenensive risk assessment in Downs syndrome .2016 ;26 : 356-362.
- Roizen MF. Anesthetic implications of concurrent diseases. Miller’s anesthesia. 2005: 1100-3.
- Takahashi T, Sakai N, Iwasaki T, Doyle TC, Mobley WC, Nishino S. Detailed evaluation of the upper airway in the Dp (16) 1Yey mouse model of Down syndrome. Scientific reports. 2020; 10 (1): 1-1.