
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Triphasic dysnatremia complicated by generalized convulsions following craniopharyngioma resection in a pediatric patient
Nikhil Swarnkar*; Anshul Yadav
Department of Neurosciences, Medanta Hospital, Vijay Nagar, Indore 452010, India.
*Corresponding Author: Nikhil Swarnkar
Department of Neurosciences, Medanta Hospital
Vijay Nagar, Indore 452010, India.
Email: nik272001@yahoo.com
Received : Oct 10, 2021
Accepted : Nov 26, 2021
Published : Dec 03, 2021
Archived : www.jcimcr.org
Copyright : © Swarnkar N (2021).
Citation: Swarnkar N, Yadav A. Triphasic dysnatremia complicated by generalized convulsions following craniopharyngioma resection in a pediatric patient. J Clin Images Med Case Rep. 2021; 2(6): 1453.
Introduction
Craniopharyngiomas are benign epithelial tumors arising from craniopharyngial duct. Although rare, these are the most common suprasellar, non-glial tumors in children constituting about 50% of all sellar / suprasellar tumors. The management of these tumors can be very challenging not only periopratively but also in postoperative phase as it can lead to extremes of dysnatremias ranging from central diabetes incipidus (CDI), syndrome of inappropriate anti diuretic hormone (SIADH) to cerebral salt wasting syndrome (CSWS). We present a triphasic sodium imbalance following craniopharyngioma resection complicated by generalized convulsions.
Case presentation
A 6 years old child presented with one month’s history of headache, vomiting and diminution of vision. Preoperative scans revealed a suprasellar lesion measuring 3 X 2.3 X 3.8 cm.
Tumor was resected completely with surgery lasting 8 hours. On post operative day 1 patient developed CDI with serum sodium levels reaching 164.8 meq/l and urine output exceeding 2.5 ml/kg/hr. This episode was managed with desmopressin 10 ug intranasal puff and appropriate oral fluid intake since child was conscious, alert and cooperative and was accepting feeds freely. Sodium levels normalize over next 48 hours ranging in the mid 140’s but by day 3 levels started declining to a level of 128 meq/l. On the same day evening, patient had one episode of generalized convulsions which was managed with Injection midazolam. Patient was intubated, sedated with midazolam infusion and electively ventilated. S. BUN & creatinine, S./U. uric acid and U. Na were ordered to establish the diagnosis of SIADH. Management at this time included fluid restriction to 2/3rd of total daily maintenance fluid, sodium supplement in the form of hyper tonic saline along with 4 hourly S. Na monitoring. Any hypokalemia at this stage should also be corrected as S. Na level is determined by exchangeable cations (Na & K) and total body water. Once Na levels normalized over next 36 hours, patient was extubated. By day 6 onwards, the patient’s sodium started rising again but he was able to correct it himself and did not require any intervention (permanent CDI phase).
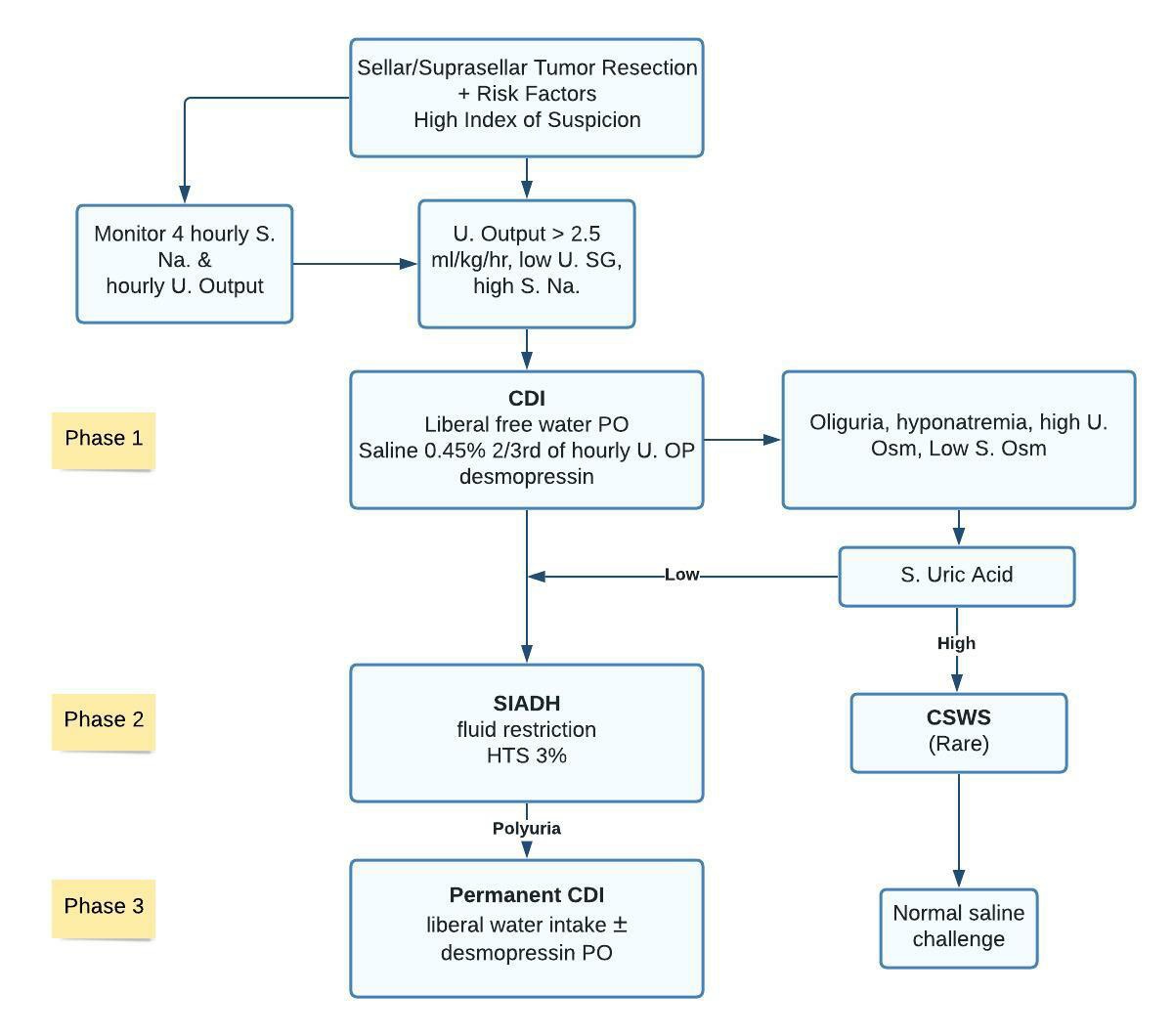
Risk factors include male child, radical resection, CSF leak and prolonged duration of surgery. U-Urine, SG-Specific Gravity, S-Serum, Osm-Osmolality. Desmopressin given 10 ug puff each nostril or 100 ugorally per day. HTS-Hyper tonic saline 3% given at 2 ml/kg body weight to maximum 3 boluses. (Each bolus resulting in expected Serum sodium rise of 2 meq/L.) S. Uric Acid cut off is 4 mg/dl.

Discussion
Suprasellar/seller lesions are known to cause wide spectrum of sodium and water imbalances specially in post operative period. Therefore one must be vigilant enough to recognize them timely. Various risk factors have been identified and they include young male patient, radical resection, cerebral spinal fluid leak and prolonged surgical duration are some of them [1]. Although CDI is most common presentation in the initial postoperative period, it may also lead to SIADH followed by permanent CDI known as Triphasic dysnatremic response (Chart 1) [2]. In this case, on 2nd postoperative day child had polyuria and hypernatremia with low urine specific gravity, clinical hallmark of CDI. Management in this phase includes free water intake if possible along with desmopressin Intranasal puffs 10 ug in each nostril. Saline 0.45% should be preferred intravenous fluid over dextrose 5% as dextrose infusion is associated with worse clinical outcome [3]. This initial phase of CDI was followed by SIADH where injured neurons or degenerating posterior pituitary begin to release ADH excessively. Diagnosis at this requires high index of clinical suspicion as presentation mimics that of CSWS and patient’s volume status cannot be established reliably. High urine osmolality, high urine sodium and low serum osmolality in the face of normal renal, thyroid and adrenal function might help in this regard. Normal saline fluid challenge is not always feasible in intensive care units and it may worsen the hyponatremia in SIADH so in this case we relied on serum uric acid concentration to help in differential diagnosis [4]. Hypouricemia (S. Uric acid ≤ 4 mg/dl) favors SIADH [5]. Hyper tonic saline 3% 2 ml/kg body weight bolus (maximum 3 boluses) can be used to correct sodium level if symptomatic along with fluid restriction. Seizure may complicate clinical scenario at this time which mainly depends on rate and intensity of fall in sodium concentration rather than any arbitrary level therefore any sodium level if symptomatic should be dealt with accordingly [6]. Finally patient develops a permanent phase CDI but with intact thirst mechanism they do not usually require any active medical intervention as was the case with this child.
Conclusion
In conclusion, sodium and water imbalance following sellar and suprasellar tumor resection presents a lot of challenges post operatively, high degree of clinical suspicion is the cornerstone of management. Hyponatremia may result in seizure complication irrespective of any arbitrary sodium level so if symptomatic, it should be addressed on emergent basis. Although less common, CSWS must be excluded while contemplating the diagnosis of SIADH.
References
- Loh JA, Verbalis J G. Diabetes insipidus as a complication after pituitary surgery. Nat Clin Pract Endocrinol Metab. 2007; 3: 489 94.
- Lindsay RS, Seckl JR, Padfield PL. The triple-phase responseproblems of water balance after pituitary surgery. Postgrad Med J. 1995; 71: 439-441
- Mukherjee KK, Dutta P, Singh A, Gupta P, Srinivasan A, Bhagat H, et al. Choice of fluid therapy in patients of craniopharyngioma in the perioperative period: A hospital based preliminary study. Surg Neurol Int. 2014; 5: 105.
- Sterns RH, Silver SM: Cerebral salt wasting versus SIADH: what difference? J Am Soc Nephrol. 2008; 19: 194-196.
- Decaux G, Dumont I, Waterlot Y, Hanson B. Mechanisms of hypouricemia in the syndrome of inappropriate secretion of antidiuretic hormone. Nephron. 1985; 39: 164-8.
- Overgaard-Steensen C, Ring T: Clinical review: Practical approach to hyponatraemia and hypernatraemia in critically ill patients. Critical Care. 2013; 17: 206.