
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Determinants of postnatal care supplements in Bole Sub-City health centers under the COVID-19 environment: Analysis of service user’s perspective
Nolawit Kebede1*; Nigatu Regassa2
1 Department of Maternal and Child Health Care Service, Hidase Health Center, Addis Ababa, Ethiopia.
2 Center for Population Studies, College of Development Studies, Addis Ababa University, Sidist Kilo Campus, Ethiopia.
*Corresponding Author: Nolawit Kebede
Hidase Health Center, Department of Maternal and
Child Health Care Service, Addis Ababa, Ethiopia.
Email: nolakebede7@yahoo.com
Received : Oct 12, 2021
Accepted : Nov 29, 2021
Published : Dec 06, 2021
Archived : www.jcimcr.org
Copyright : © Kebede N (2021).
Abstract
Background: PNC visits helps decrease maternal morbidity and mortality after delivery. The services (both provision and utilization) are severely affected during crisis, such as the recent COVID-19 pandemic due to health care services being suspended and shifting to combat the pandemic.
Objective: To assess the determinants and challenges of postnatal care service utilization, specifically intake of key supplements (iron, folic acid, and antibiotics) among pregnant women attending Bole Sub City Health Centers under the COVID-19 pandemic.
Method: A sample size of 405 mothers with most recent births who got the service in the selected Bole Sub-City health centers were interviewed. A negative binomial regression analysis was used to assess the determinants of postnatal supplement intake.
Result: 44.9 percent of the respondents used PNC services but only 10.6 percent of them took the postnatal supplements. For respondents in the age group 25-34, the expected mean number of postpartum intakes increased by 1.22 (95% CI: 1.121-1.346) compared to women 35 and above. The expected mean number of postpartum intake decreased by 38.1 percent (IRR = 0.619; 95% CI: 0.548-0.700) for women who were currently living with their husbands when compared to those who don’t. For women who had 2-3 children, the expected mean number of postpartum supplement intake decreased by 32.8 percent (IRR = 0.672; 95% CI: 0.618 - 0.730) compared to the reference category. Women with primary education, had an expected mean number to decrease by 10 percent (IRR = 0.903, 95% CI: 0.825- 0.987) than those who had college or university education. Those with very low and low household income, the expected mean number of postnatal supplement intake decreased by 25.7 percent (IRR = 0.743, 95% CI: 0.678-0.814) and 22.9 percent (IRR = 0.771, 95% CI: 0.706- 0.841) respectively. But increased by 1.257 (95% CI: 1.227-1.403) for women in the moderate household wealth. Orthodox Christian and Muslim women had the expected mean number to increase by 1.092 (95% CI: 1.010-1.180) and 1.24 (95% CI: 1.136-1.354) respectively when compared to the reference category. Working women had an expected mean number of postnatal supplement intake of 1.13 (95% CI: 1.063-1.202) when compared with those who don’t have work.
Lastly for women who had PNC visits, the expected mean number of postnatal supplement intake increased by 1.138.
Conclusion: Maternal morbidity and mortality is the highest during post-partum period. But this could be minimized by attending postnatal care services. This study suggests increasing awareness in mothers to attend the recommended number of visit to secure health of the mothers and their newborn.
Keywords: postnatal service; iron; folate; supplement; health center.
Abbreviations: CI: Confidence Interval; CSA: Central Statistics Agency; COVID-19: Coronavirus disease 2019; EDHS: Ethiopian Demographic Health Survey; IRR: Incidence Rate Ratio; PNC: Postnatal Care; PPE: Personal Protective Equipment; SVD: Simple Vaginal Delivery; WHO: World Health Organization.
Citation: Kebede N, Regassa N. Determinants of postnatal care supplements in Bole Sub-City health centers under the COVID-19 environment: Analysis of service user’s perspective. J Clin Images Med Case Rep. 2021; 2(6): 1457.
Background
The WHO defines the postnatal period as the time between an hour after the placenta is delivered and six weeks after the child is born. To ensure safe delivery for mothers and their infants, proper care, skilled birth attendants, and a sanitary environment must be in place. According to a WHO report, approximately 295,000 women died during and after pregnancy and childbirth in 2017 [1,2]. The majority of the deaths occurred in low-resource settings and could have been avoided. The main cause of death was complications such as severe bleeding, infections after childbirth, delivery complications, and high blood pressure during pregnancy [2].
Postnatal care service also serves as medium for intake of supplements that are taken after delivery. As per the WHO Standards of maternal and neonatal care; iron and folate must be given for six month during pregnancy and continued for three month after delivery. This is important to prevent and treat iron deficiency during and after pregnancy [3]. In addition antibiotics given after delivery by simple vaginal delivery or caesarian section minimizes infection to the mother [4].
Furthermore, WHO recommendations state that when labor is attended in a health facility via Simple Vaginal Delivery (SVD), ordinary newborns must be given a minimum of 24-hour care [2]. However, if the birth takes place outside of a health facility, it’s crucial that the first postnatal visit must take place within the first 24 hours of delivery. In addition, regardless of where the baby is born, at least three additional postnatal visits must be scheduled for all mothers and newborns. This visit occurs on the third day following delivery, between the first and second weeks, and six weeks after delivery. Despite this, less than a quarter of newborns in developing countries receive PNC within 48 hours of birth [1].
Many factors determine the use of PNC service utilization and provisions. The factors could be demographic and socioeconomic factors, obstetric characteristics and physical accessibility of the health care services [4-8]. Previous studies conducted on the subject showed that women’s education positively impacts the use of PNC services [5,9,10]. Though it is not as strong as maternal education, husband’s education also reflects preferences for health-care utilization [11]. Mothers’ age [12,13], household wealth status [14,15] and difficulty or complications from previous labor increases the use of PNC services were reported as important determinants of PNC [16]. Maternal autonomy and decision-making power is another factor which. increases mothers’ ability to seek services, as well as access and receiving medical care, even in places where services are readily available [17,18].
The COVID-19 pandemic has affected maternal health care services in various ways. Lockdown and movement restrictions that were put up to control the spread of the virus have acted as a barrier for service utilization [19]. Supply and delivery of sexual and reproductive health commodities is also affected by the lockdown measures due to the low priority given to these products [20]. In addition, fear of contracting the virus has also decreased the health-seeking behavior of mothers. This is similar to the Ebola outbreak in West Africa [17] with a drop in maternal health care service coverage resulted in more maternal and child death [21].
Meanwhile, health care workers are facing risk of exposure due to their direct contact with patients, inadequate supply of personal protective equipment, draining shifts, staff shortage, and scarce supplies. In addition, being isolated from their families is affecting them emotionally and physically. These mental health problems coupled with the deficient supplies takes a toll on the health care service delivery and overall wellbeing of the health care providers [22]. Maternity hospitalizations postdelivery have been shortened as little as 24 hours, limiting the opportunity for staff-supported labor recovery, breastfeeding support, education in infant care, and planning for postpartum mental health management [23].
This study aims to assess postnatal supplement utilization and provision under the COVID-19 pandemic. It also tries to assess the determinants as well as the challenges and quality of care during the pandemic.
Methods and materials
Study context
The study was conducted in Addis Ababa, the capital city of Ethiopia. According to the Addis Ababa City Administration Health Bureau; the total population residing in the city administration is 3,686,068. From this 1,769,313 were male and 1,879,895 were female [24]. There are 11 sub-cities and 117 districts called ‘woredas’. There are a total of 14 hospitals; seven of them are under the Federal Ministry of Health and the remaining are under Addis Ababa City Administration Health Bureau. Furthermore, there are 98 functional health centers and 23 are being constructed [24]. The study was done in selected Bole Sub City health centers in Addis Ababa, Ethiopia. The study population were women of the reproductive age group who visited the health centers for maternal and reproductive health care services during the reference period of 12 months.
Data sources
Primary data was collected through a quantitative individual survey and interviews of selected key informants. Secondary data was collected from the registry of PNC from the selected health centers. Other facility-based information was also taken from the institution concerned.
Sampling method
The primary objective of the study focused on postnatal supplements, hence it was important to make the most suitable indicator for the sampling purpose. As the prevalence of these indicators varies and the most current/accurate proportion of the parameters may not be readily available for facility-level studies, the default 50% (p = 0.50) was used for maximum effects. Thus sample size was estimated using the following formula:
Replacing the components of the formula with values, the sample size computed was:
Adding a 5% for non-response rate; overall sums it up to a total of 404 clients who were interviewed in the three health centers (Bulbula, Goro, and DilFrie) which were selected using a simple random sampling method. Lastly, three clinical nurses and one health officer were recruited to collect the data after receiving intensive training.
Measure of outcome and exposure variables
The outcome variable was postnatal supplement intake. It was measured by linearly combining three binary responses (yes/no) on intake of key supplements during PNC visit.
For this analysis, the explanatory variables were divided into three major categories: Maternal and child factors (which includes, birth order, parity, mothers' education, age, work status, ever experiencing pregnancy termination, etc.), household factors (which include household income, religion, husbands’ education and occupation, and type of family structure). The supply side determinants/problems (providers’ perspective) included institutional variables and community variables such as distance to the health facility, availability of services, type of provider, etc.
Statistical analysis
The collected data was cleaned, checked for completeness, compiled, and entered into SPSS version 23. Simple descriptive statistics such as frequencies were employed to report the socio-demographic characteristics and service characteristics.
Both bivariable and multivariable logistic regressions was performed to identify the presence of a significant association between selected independent variables and the dependent variables of interest. Those variables with p < 0.2 in the bivariate analysis was considered for multivariable negative binomial regression analysis [25]. Multi-collinearity among the potential predictors was checked using a correlation matrix. An adjusted odds ratio for a 95% confidence interval was employed to see the strength and directions of association between independent variables and the outcome variables. All statistical tests were two-sided, and the significant association was declared at a p-value less than 0.05.
Result
Table 1 displays the background characteristics of the study participants. Around 65 percent of the study participants were in the age group 25-34 and 40 percent of the respondents had already given birth at least once. With regards to educational status, 46 percent of the women and 40 percent of their husbands had completed primary education. 51 percent reported living in a household size of 4-6. Most of the respondents (74%) stated that they were not working during the survey period. Close to two-thirds (63%) of the study participants were Orthodox Christian followers.
Table 1:Demographic and socio-economic characteristics of the respondents, Addis Ababa Bole Sub city health centers (n = 405).
Background Variables |
No. |
Percentage |
Age of the respondents |
||
15-24 |
113 |
27.9 |
25-34 |
263 |
64.9 |
35+ |
29 |
7.2 |
Parity |
||
1 |
160 |
39.5 |
2 |
138 |
34.1 |
3 |
63 |
15.6 |
≥4 |
44 |
10.9 |
Educational Status of the respondents |
||
No formal education |
64 |
15.8 |
Primary education |
187 |
46.2 |
Secondary education |
87 |
21.5 |
College or Higher |
67 |
16.5 |
Household size |
||
1-3 |
188 |
46.4 |
4-6 |
206 |
50.9 |
>6 |
11 |
2.7 |
Work status respondents |
||
Not working |
299 |
73.8 |
Working |
106 |
26.2 |
Educational status of the husband |
||
No formal education |
34 |
8.4 |
Primary education |
161 |
39.8 |
Secondary education |
117 |
28.9 |
College or University |
91 |
22.5 |
Religion of the respondent |
||
Orthodox Christian |
256 |
63.2 |
Muslim |
89 |
22 |
Others |
60 |
14.8 |
The outcome variable had a Poisson distribution with significantly different mean and standard deviation. As the outcome is a count variable with a right-skewed distribution (Figure 1), a negative binomial regression was fitted.
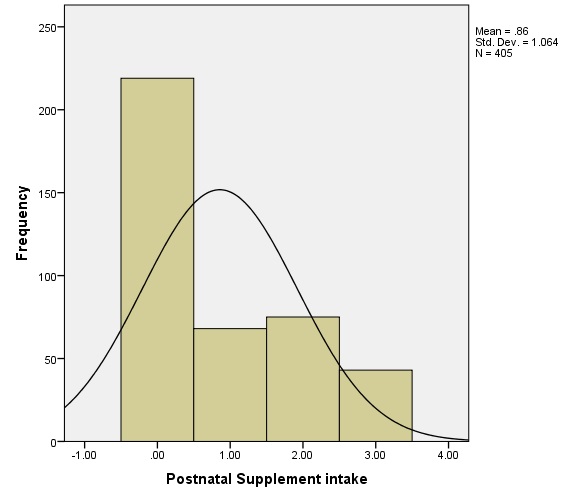
Table 2 presents the results of bivariable negative binomial regression for postpartum supplement intake. The expected mean number of postpartum intake increased by 1.11 (95% CI: 1.027-1.204) times for women in the age group 25-34 when compared to the age group 35 and above. When we look at the household income of the respondents, the expected mean number of postpartum supplement intake decreases by 11.6 percent (IRR = 0.884; 95% CI: 0.821-0.952) and 7.7 percent (IRR = 0.92; 95% CI: 0.855-0.997) for very low income and low-income categories, respectively. But the expected mean increased by 1.32 (95% CI: 1.194 - 1.468) for the moderate-income category.
Table 2:Results of bivariable Negative Binomial regression (unadjusted) for postpartum supplement intake, Addis Ababa Bole Sub City Health centers (n = 405).
95% CI |
||||
Variables |
p-value |
IRR |
Lower |
Upper |
Age of the respondent |
||||
15-24 |
0.769 |
0.986 |
0.899 |
1.082 |
25-34 |
0.009 |
1.112 |
1.027 |
1.204 |
35+ RC |
- |
1.00 |
- |
- |
Educational status of the respondent |
||||
No formal education |
0.811 |
0.99 |
0.91 |
1.076 |
Primary education |
0.052 |
0.932 |
0.867 |
1.001 |
Secondary education |
0.216 |
0.95 |
0.875 |
1.03 |
College or University RC |
- |
1.00 |
- |
- |
Living arrangements |
||||
Currently living with husband |
0.000 |
0.677 |
0.604 |
0.757 |
Currently not living with husband RC |
- |
1.00 |
- |
- |
Planned for pregnancy |
||||
Yes |
0.000 |
0.798 |
0.744 |
0.857 |
No RC |
- |
1.00 |
- |
- |
Household Income |
||||
Very low |
0.001 |
0.884 |
0.821 |
0.952 |
Low |
0.041 |
0.923 |
0.855 |
0.997 |
Moderate |
0.000 |
1.324 |
1.194 |
1.468 |
High RC |
- |
1.00 |
- |
- |
Religion of the respondent |
||||
Orthodox Christian |
0.495 |
1.025 |
0.954 |
1.102 |
Muslim |
0.002 |
1.135 |
1.046 |
1.231 |
Others RC |
- |
1.00 |
- |
- |
Children ever born |
||||
≤1 |
0.488 |
0.973 |
0.902 |
1.05 |
2-3 |
0.000 |
0.754 |
0.703 |
0.809 |
≥4RC |
- |
1.00 |
- |
- |
Work status of the respondent |
||||
Not Working |
0.19 |
1.023 |
0.968 |
1.081 |
Working RC |
- |
1.00 |
- |
- |
Finally, the expected mean number of postpartum supplement intake increased by 24.6 percent (IRR = 0.754; 95% CI: 0.703- 0.809) for those who had 2-3 children.
Table 3 presents the results of multivariable negative binomial regression analysis for postpartum supplement intake. For respondents in the age group 25-34, the expected mean number of postpartum intakes increased by 1.22 (95% CI: 1.121-1.346) compared to women in the age group 35 and above. The mean expected number of postpartum intakes decreased by 38.1 percent (IRR = 0.619; 95% CI: 0.548-0.700) for women who were currently living with their husbands in contrast to women who were currently living with their husbands. Similarly, the mean expected number of postpartum supplement intake for women who had 2-3 children decreased by 32.8 percent (IRR = 0.672; 95% CI: 0.618-0.730) compared to the reference category.
Table 3:Results of multivariable negative binomial regression analysis (adjusted) for postpartum supplement intake, Addis Ababa Bole Sub City health centers (n = 405).
95% CI |
||||
Variable |
p-value |
IRR |
Lower |
Upper |
Intercept |
0.001 |
1.406 |
1.156 |
1.711 |
Age of the respondent |
||||
15-24 |
0.916 |
0.994 |
0.889 |
1.112 |
25-34 |
0.000 |
1.228 |
1.121 |
1.346 |
35 + RC |
- |
1.00 |
- |
- |
Educational status of the respondent |
||||
No formal education |
0.551 |
0.969 |
0.872 |
1.076 |
Primary education |
0.025 |
0.903 |
0.825 |
0.987 |
Secondary education |
0.48 |
1.033 |
0.945 |
1.128 |
College or University RC |
- |
1.00 |
- |
- |
Living arrangement |
||||
Currently living with husband |
0.000 |
0.619 |
0.548 |
0.7 |
Currently not living with husband RC |
- |
1.00 |
- |
- |
Planned for pregnancy |
||||
Yes |
0.000 |
0.779 |
0.721 |
0.842 |
No RC |
- |
1.00 |
- |
- |
Household income |
||||
Very low |
0.000 |
0.743 |
0.678 |
0.814 |
Low |
0.000 |
0.771 |
0.706 |
0.841 |
Moderate |
0.000 |
1.257 |
1.127 |
1.403 |
High RC |
- |
1.00 |
- |
- |
Religion of the respondent |
||||
Orthodox Christian |
0.027 |
1.092 |
1.01 |
1.18 |
Muslim |
0.000 |
1.24 |
1.136 |
1.354 |
Others RC |
- |
1.00 |
- |
- |
Children ever born |
||||
≤1 |
0.231 |
0.944 |
0.86 |
1.037 |
2-3 |
0.000 |
0.672 |
0.618 |
0.73 |
≥4 RC |
- |
1.00 |
- |
- |
Work status of the respondent |
||||
Not working |
0.000 |
1.13 |
1.063 |
1.202 |
Working RC |
- |
1.00 |
- |
- |
Number of PNC visits |
0.000 |
1.138 |
1.119 |
1.158 |
Scale |
1.00 |
|||
Deviance/DF = 1.554 |
||||
Discussion
The study has primarily aimed to estimate the level of postnatal care supplement utilization before and during the COVID-19 pandemic in the selected Bole Sub City Health Centers Addis Ababa, Ethiopia. A total of 405 women were interviewed about their experience of utilization of maternal healthcare services during the pandemic.
Women who attended PNC services were only 44.9%, of which only 10.6 percent of them received all three postpartum supplements. This figure is higher when compared with other similar studies; 2011 EDHS (9.3%) and 2016 EDHS (17%) [26,27]. The study showed that for women who got all the supplements, at least two and at least one was 10.6 percent, 18.5 percent and 16.8 percent, respectively. About 54 percent didn’t receive any of the supplements. This difference could be that the prevalence of Anemia is at 23%, which is lower than the recommended percent set by the WHO (40%). In addition to this iron and folic acid are usually prescribed if a mother lost a lot of blood during delivery [27].
The results obtained from the multivariable analysis showed a range of demographic and socio-economic and service related factors affected the utilization of postpartum supplements. It showed that age of the respondent, education of the respondent, living arrangement, household income, planned pregnancy, number of PNC visits, children ever born, work status of the respondent, and religion were significantly associated with the outcome variable.
Age was found to be significantly associated with the intake of postpartum supplements intake. Women in the age group 25-34 were more likely to utilize the service. This result is inconsistent with a study done in the Hawasa Zuria district which stated that women in the age group below 25 were more likely to use the services [6]. The possible explanation for the results could be that older women probably have experience with childbirth and utilization of the postpartum supplements.
The effect of education on postpartum supplement intake shows a inverse association. Women who had primary-level education were less likely to take the supplements. Comparable studies were not found to confirm this result. But, one study affirmed that literate women were more likely to use the services [28]. Another study also stated that women who had secondary and higher education influenced utilization of the services [5,10]. Even though literacy increases a women’s autonomy and develops the confidence to make decisions on health care, the level of education also plays a role in enabling that decision.
Cohabitation was also another variable that showed an inverse association with postpartum supplement intake. Women who were currently living with their husbands were less likely to use the postpartum supplements. Similarly, a study done in Southwest Shoa found out those women who were married or living with their husbands didn’t attend the services [17]. On the contrary, a study done by Tafesse and Niguse showed that women cohabitating with their husbands used the service [28]. The inconsistency in the results could be due to different study time.
Planned pregnancy was significantly associated with taking postpartum supplements. Women who planned to get pregnant were less likely to adhere to the services provided. This result was not consistent with other local studies [6]. A possible reason for the difference could be the results obtained in this study are during the pandemic. So women who planned to give birth during this time might not visit the health centers after delivery due to the fear of contracting the virus and passing it to their newborns.
The findings show that household wealth status was strongly associated with the intake of postpartum supplements. Women with moderate household incomes were more likely to get the supplements. This is supported by different studies which show similar results [8,10,14,15]. Women in the moderate wealth quintile were more likely to use the service than women in the low-level wealth quintile, and women in the low-level wealth quintile were more likely to use the service than the very low wealth quintile. This could be explained in that women who are financially independent can afford to pay for the supplements and transport costs when visiting the health care services.
Religion was also another variable that influenced intake of the postpartum supplements. The results from this study showed that Orthodox Christians and Muslims were more likely to get the services compared to catholic and protestant. This is supported by a study done in South West Shoa [17]. The pathways through which religion influences PNC services may need further investigation.
The effects of children ever born is also worth mentioning. Women who had 2-3 children were less likely to take the supplements. This finding contradicted with a study done by Berhan, et.al. Possible reason for the difference might be the respondents might not have time to visit the health care facility since they are busy with taking care of their children and their work at the same time. In addition, since they have experience with previous birth they might not think it is essential to visit the health care facility to get the services. On top of that, this study is only done in Addis Ababa, whereas the latter study analyzed the 2016 EDHS [8].
Work status of the mother shows an influence on the uptake of the postnatal supplements. Women who were working were more likely to take postpartum supplements than those who don’t work. A study done by Kassu and Eshetu supports this finding. Working women have the economic ability to pay for the services. Besides they are more empowered when it comes to decision-making regarding their health and are also close to getting information [13].
The last variable that showed a strong association with postpartum supplement intake is the number of PNC visits. Women who had PNC visits were more likely to take the supplements. This can be explained in that; the supplements are available during a PNC visit.
Strengths and limitations
This study has some strengths and limitations. To start with the strength; this study revolved around the determinants and challenges of postnatal care service during the COVID-19 pandemic. Thus the findings might be useful for informing health planners and policy makers of the importance of PNC visits for mothers to decrease maternal morbidity and mortality. In addition the results could be useful for geographic targeting, monitoring and evaluation programs. As this study tried to assess the postnatal care service during the ongoing pandemic, the results obtained might serve as a body of knowledge for future research. Then again the study is not far from pitfalls. First, the study design is a cross-sectional one which doesn’t address the cause-and-effect relationship. Therefore, care must be taken when interpreting the results. Second, there wasn’t enough literature on postpartum supplements (mainly iron, Folate, and an antibiotic) to compare the results with. Since the supplements are given during PNC visits, studies regarding PNC visits were used to compare and contrast the results found in this study.
Conclusion
Close to half of the respondents used PNC services, while only 10.6 percent of them took the postnatal supplements. Age of the respondent, education of the respondent, living arrangement, planned pregnancy, household income, religion, children ever born, work of the respondent, and number of PNC visits were significantly associated with postnatal supplement intake.
As stated above, the PNC visit attendance rate is at 44.9 percent which is below the WHO recommended rate of 90 percent. It is important to have a PNC visit in that most of maternal death occur during postpartum period. There are a number of services under PNC, as it is crucial to ensure the healthy growth of the newborn as well as the health of the mother. It is recommended to work more on creating awareness by health professionals for mothers to know the need for and importance of PNC services and making it convenient for clients to attend the services. In addition government bodies should pay attention to this service especially during a crisis time like this current pandemic.
Declarations
Ethics approval and consent to participate: Ethical clearance was obtained from the Institution Review Board of the University of Addis Ababa. Verbal informed consent was obtained from respondents prior to administration of the questionnaire.
References
- Zemenu Tadesse Tessema, Lake Yazachew, Getayeneh Antehunegn Tesema, Achamyeleh Birhanu Teshale. Determinants of postnatal care utilization in sub-Saharan Africa: a meta and multilevel analysis of data from 36 sub Saharan countries. Italian Journal of Pediatrics. 2020; 46.
- WHO.com. Maternal mortality. WHO official website. 2019.
- WHO. Standard of maternal and neonatal care, Iron and folate Supplementation. Integrated management of pregnancy and childbirth (IMPAC). 2006
- Bonet M, Ota E, Chibueze CE, Oladapo OT. Routine antibiotic prophylaxis after normal vaginal birth for reducing maternal infectious morbidity. Cochrane Database of Systematic Reviews. 2017; CD012137.
- Netsanet Abera Asseffa NA, Bukola F, Ayodele A. Determinants of use of health facility for childbirth in rural Hadiya zone, Southern Ethiopia. BMC Pregnancy and childbirth. 2016; 16.
- Shambel Yosef, Azmach Dache, Aregahegn Dona. Prevalence of early postnatal care service utilization and its associated factors among mothers in Hawassa Zuria District, Sidama Regional State Ethiopia: A cross sectional study. Hindawi Obstetrics and Gynecology International. 2021.
- Gudu.W and Addo B. Factors associated with utilization of skilled service delivery among women in rural Northern Ghana: A cross sectional study. BMC Pregnancy and childbirth. 2017; 17.
- Berhan Tsegaye, Belay Amare, Mulu Reda. Prevalence and Factors associated with immediate postnatal care utilization in Ethiopia: Analysis of Ethiopia Demographic Health Survey. International Journal of Women’s Health. 2021; 13: 257-266.
- Banke-Thomas OE, Banke-Thomas OA, Ameh CA. Factors influencing utilization of maternal health services by adolescent mothers in Low-and middle-income countries: a systematic review. BMC Pregnancy and Childbirth. 2017; 17.
- Eshetu E Chaka, Ahmed A Abdurahman, S Nedjat, R Majdzadeh. Utilization and determinants of postnatal care services in Ethiopia: A systematic Review and Meta- Analysis. Ethiop J Health Sci. 2019; 29: 935-944.
- Eyerusalem Dagne. Role of socio-demographic factors on utilization of maternal health care services in Ethiopia, MSc. Thesis (Unpublished). 2010.
- Fantaye Chemir, Melkamu Gelan, Makeda Sinaga. Postnatal Care Services utilization and associated factors among mothers who delivered in Shebe Sombo Woreda, Jimma Zone, Ethiopia. Clinmed, International Journal of women health and wellness. 2019.
- Kassu Mehari and Eshetu Wencheko. Factors affecting maternal health care services utilization in rural Ethiopia: A study based on the 2011 EDHS data. Ethiop. J. Health Dev. 2013; 21.
- Bezawit Adane, Girmatsion Fisseha, Getaw Walle, Melaku Yalew. Factors associated with postnatal care utilization among postpartum women in Ethiopia: a multilevel analysis of the 2016 Ethiopian demographic and health survey. 2020; 78.
- Maleda Mequanent Sisay, Tesfahun Taddege Geremew, Yeshamble Worku Demlie, Asaye Tariku Alem, Desalew Kassahun Beyene, Melkitu Fentie Melak, et al. Spatial patterns and determinants of postnatal care use in Ethiopia: Findings from the 2016 Demographic and Health Survey. 2019.
- Wilunda C, Quaglio G, Putoto G, Takahashi R, Calia F, Abebe D, et al. Determinants of utilization of antenatal care and skilled birth attendant at delivery in South West Shoa Zone, Ethiopia: a cross sectional study. Reproductive Health. 2015; 17.
- ShegawMulu Tarekegne, Lieberman LS, Giedraitis V. Determinants of maternal health services utilization in Ethiopia: Analysis of the 2011 EDHS.BMC Pregnancy and Childbirth. 2014; 14.
- Ahmed S, Creanga AA, Gillespie DG, Tsui A. Economic Status, Education and Empowerment: Implications for Maternal Health Service Utilization in Developing Countries. PLoS One Journal. 2010; 5.
- Headey D, Cho A, Goudet S, Oketch JA, Oo TZ. The impacts of the COVID-19 crisis on maternal and child malnutrition in Myanmar. IFPRI. 2020.
- Church K, Gassner J, Elliot M. Reproductive health under COVID-19- challenges of responding in a global crisis. 2020; 28: 1-3.
- Pant S, Koirala S, Subedi M. Access to Maternal Health Services during COVID-19. Europasian Journal Medical Science. 2020; 2: 48-53.
- Nagesh S, Chakraborty S. Saving the frontline health workforce amidst the COVID-19 crisis: Challenges and recommendations. 2020; 10.
- Lemi Belay Tolu and Wondimu Gudu Jeldu. Guidelines and best practice recommendations on reproductive health services provision amid COVID-19 pandemic. 2020.
- Addis Ababa City Administration Health Bureau E.C Annual report. 2012.
- Hosmer DW, Hosmer T, Le Cessie S. A comparison of goodnessof-fit testsfor the logistic regression model. Stat Med. 1997; 16: 965-980.
- CSA and ICF International. Ethiopia Demographic and Health Survey. Addis Ababa, Ethiopia & Calverton, MD: Central Statistical Agency & ICF International. 2011.
- Central Statistical Agency. Ethiopia Demographic and Health Survey 2016. Addis Ababa and Rockville, Maryland: CSA and ICF. 2017. 103-121.
- Tafesse Lamaro Abota and Niguse Tadele Atenafu. Postnatal care Utilization and Associated Factors among Married Women in Benchi-Maji, Zone, Southwest Ethiopia: A Community based cross-sectional study. Ethiop J Health Sci. 2018; 28930: 267-276.