
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Two cases of penile fracture with and without associated urethral rupture: Case reports and review of the literature
Federico A Rovegno
Division of Urology, Departament of Surgery, CEMIC University Hospital, Buenos Aires, Argentina.
*Corresponding Author: Federico A Rovegno
Division of Urology, Departament of Surgery, CEMIC
University Hospital, Buenos Aires, Argentina.
Email: federicoagustin605@gmail.com
Received : Oct 15, 2021
Accepted : Nov 30, 2021
Published : Dec 07, 2021
Archived : www.jcimcr.org
Copyright : © Rovegno FA (2021).
Abstract
Penile fracture is a rare lesion that occurs almost exclusively during erection. This lesion may be associated with rupture of the urethra in 20-30% of the cases. We present two cases of a 41-year-old man with a penile fracture complicated by a urethral rupture and a 33 year old man with a penile fracture without urethral rupture. Subsequent repair was done in both cases. For diagnosis it is necessary in most cases a correct anamnesis and physical examination. Early surgical approach and closure of the albuginea´s lesion and repair of the urethral lesion is the best way of treatment.
Citation: Rovegno FA. Two cases of penile fracture with and without asscociated urethral rupture. Case reports and review of the literature. J Clin Images Med Case Rep. 2021; 2(6): 1460.
Introduction
Penile fracture, defined as rupture of the tunica albuginea of the corpora cavernosa, can occur in isolation or in association with a urethral tear [1,2].
Although the diagnosis of penile fracture is mainly clinical, with the patient reporting a “popping” sound followed by pain, rapid detumescence, swelling, and bruising, imaging can play a role in confirming the diagnosis, identifying the exact location of the tunica tear, and ruling out the presence of urethral involvement [3,4].
It is widely accepted that the gold standard management of penile fracture is immediate surgical exploration and repair of the tunica tear and, eventually, of the associated urethral injury to minimize fibrosis deposition in the cavernosal spaces and, in consequence, to lessen the risk of long-term erectile dysfunction [4-6].
Owing to the relatively low incidence of penile fracture, many aspects of the diagnostic process and of the surgical and functional outcomes are described in case series because the number of systematic reviews on this topic is very limited [7].
Case presentation
A 41-year-old man reported to the emergency room 4 hours after striking his erect penis against his partner’s perineum during sexual intercourse. This was accompanied by immediate pain and detumescence. Significant penoscrotal swelling ensued.
Physical exam revealed a swollen, ecchymotic penis without blood at the meatus (Figure 1). Appropriate concern for penile fracture led to operative management.

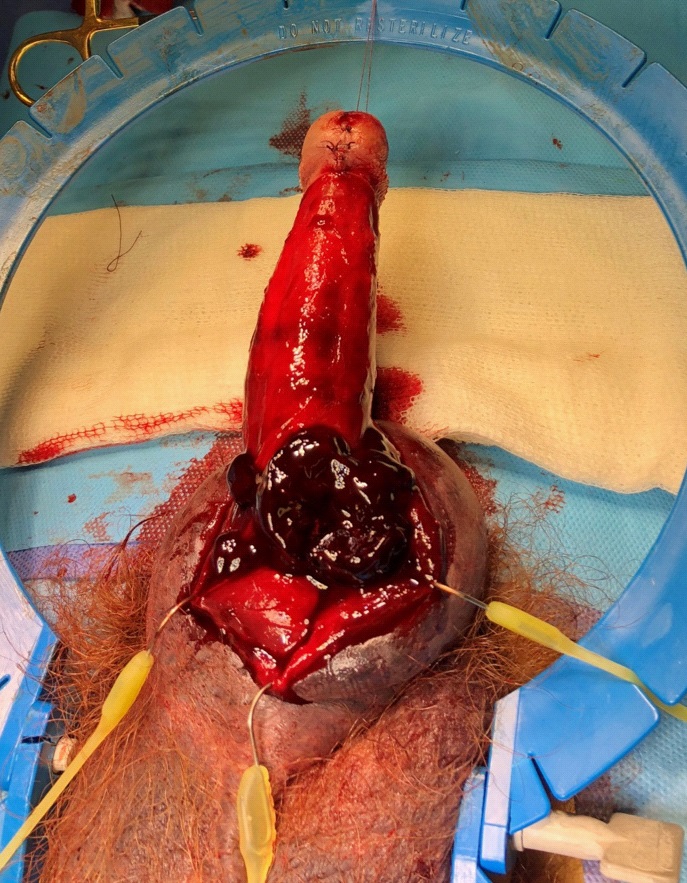
At the time of operation, a subcoronal circumcising incision was made and the penis was degloved. After evacuation of a large hematoma (Figure 2), a significant defect was identified in the left corpus cavernosum. The defect was ventralin location though lateral of midline. Additionally, a large injury involving the ventral half of the urethra was identified (Figure 3). A 16 French catheter was introduced through the meatus, maneuvered across the defect and into the bladder. The urethra was then closed in a watertight fashion over the catheter using 4-0 Vicryl suture. The cavernosal injury was repaired in an interrupted fashion using 3-0 PDS suture (Figure 4). A circumcision was then performed and the skin edges were reapproximated using interrupted 4-0 Vicryl suture. The urethral catheter was left in place for 4 weeks and then removed.
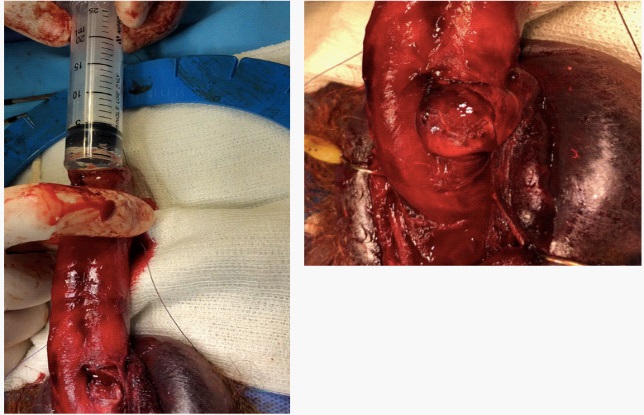
The other patient is a 33 year old man that presented to the emergency with history of penile swelling for 6 hours. The incident happened during sexual intercourse when he struck the perineum of his partner. He heard a cracking sound and a severe pain in the penis followed by swelling. Physical examination showed severely swollen penis without blood in the meatus. Palpable hematoma with tenderness was noted over the ventral aspect of the penis. Ultrasound showed a 3 cm hematoma at the base of the penis between the albuginea´s tunica and the skin. He was submitted to surgery and a subcoronal circumcising incision was made and the penis was degloved. After evacuation of a large hematoma a defect was identified in the right corpus cavernosum, without urethral damage (Figure 5). The cavernosal injury was repaired in an interrupted fashion using 3-0 PDS suture.


Both patients voided without difficulty and were able to regain erectile function. Patients reported good erection with no curvature of the penis and good urine flow during follow-up visits after 6 months. Patients were scheduled for further followup visits to evaluate the long term results.
Discussion
A penile fracture consists of the rupture of the tunica albuginea of the corpora cavernosa and it almost always occurs when the shaft is in the erect state. In the erect state, the thickness of the tunica albuginea, which in flaccidity is around 2 mm, decreases to 0.25–0.50 mm [6,8]. A widely held view is that the ‘woman on top’ position poses the greatest risk to penile fracture although no systematic review has corroborated this [1].
The albugineal tears are mainly unilateral and transversal, and they tend to occur ventrally as the three layers that form the tunica albuginea become two ventrally and because the neurovascular bundle provides further support and protection dorsally [6,8].
Because of the practice of taqaandan, which consists of forcefully bending the shaft of the erect penis to achieve sudden detumescence, the prevalence of penile fracture in the Middle East and northern Africa is greater than in the rest of the world [9].
In 3 of the largest studies in the Eastern literature, success rates vary from 91.8% to 100% after early repair. In these studies, between 40% and 76.4% of the injuries were self-inflicted [10].
Three of the largest studies in the Western literature, from Spain, Germany and Croatia, and Switzerland contained 15, 22, and 29 patients, respectively, and were secondary to sexual trauma in 54.4-89% of patients. Good erectile function, including the lack of significant curvature, was seen in 80-94.7% of patients with immediate repair [11,12]. The metaanalysis of Amer et al. is about 3.213 patients, but Middle Eastern cases are included, influenced by etiology by the taqaandan maneuver.
The utility of preoperative imaging in penile fracture has been controversial because of cost, delay of surgical intervention, false-negative rate, and the inability to change clinical decision-making in many cases [5]. Ultrasonography has been found to be able to determine the location of the albuginea tear, especially in larger injuries, allowing for improved operative planning [13] and can be accurate in as high as 86% of patients in a small series [14].
In addition to tunica albuginea tears, other structures can be injured during sexual trauma, including the urethra, superficial dorsal penile vein, deep dorsal vein, dorsal artery, or nonspecific bleeding from the dartos tissue [15].
Conservative management of a fractured penis consists of measures that promote a quicker healing process, such as compressive dressings, elevation and administration of antiandrogens to suppress erections until the tunical tear has healed [15]. This approach is associated with significant complications, including corporeal fibrosis, delayed chordee and plaque formation, which can occur in up to 50% of cases [6].
Immediate repair in patients presenting with clinical history of penile fracture has become the standard of care because of the excellent outcomes reported [10].
Conclusion
Penile fracture with urethral section is a rare urological emergency, the most frequent cause of which in occident is violent sexual activity. Although its diagnosis is essentially clinical, US plays an important role in confirming the diagnosis and identifying the site of the injury and an associated urethral laceration. Early surgical approach and closure of the albuginea´s lesion and repair of the urethral lesion is the best way of treatment.
References
- Amer T, Wilson R, Chlosta P, et al. Penile fracture: A metaanalysis. Urol Int. 2016; 96: 315-329.
- Sawh SL, O’Leary MP, Ferreira MD, et al. Fractured penis: a review. Int J Impot Res. 2008; 20: 366-369.
- Guler I, Ödev K, Kalkan H, et al. The value of magnetic resonance imaging in the diagnosis of penile fracture. Int Braz J Urol. 2015; 41: 325-328.
- Lee SH, Bak CW, Choi MH, et al. Trauma to male genital organs: a 10-year review of 156 patients, including 118 treated by surgery. BJU Int. 2008; 101: 211-215.
- Swanson DEW, Polackwich AS, Helfand BT, et al. Penile fracture: outcomes of early surgical intervention. Urology. 2014; 84: 1117-1121.
- Lumen N, Kuehhas FE, Djakovic N, et al. Review of the current management of lower urinary tract injuries by the EAU Trauma Guidelines Panel. Eur Urol. 2015; 67: 925-929.
- Wong N, Dason S, Bansal R, et al. Can it wait?—A systematic review of immediate versus delayed surgical repair of penile fracture. Can Urol Assoc J. 2017; 11: 53-60.
- Gontero P, Muir GH, Frea B. Pathological findings of penile fractures and their surgical management. Urol Int. 2003; 71: 77–82.
- Zargooshi J. Penile fracture in Kermanshah, Iran: the long-term results of surgical treatment. BJU Int. 2002; 89: 890-894.
- Zargooshi J. Sexual function and tunica albuginea wound healing following penile fracture: an 18-year follow-up study of 352 patients from Kermanshah, Iran. J Sex Med. 2009; 6: 1141-1150.
- Sierra JM, Garcia GH, Perez FC, et al. Surgical repair and analysis of penile fracture complications. Urol Int. 2011; 86: 439-443.
- Persec Z, Persec J, Puskar D, et al. Penile injury and effect on male sexual function. Andrologia. 2011; 43: 213-216.
- Kervancioglu S, Ozkur A, Bayram MM. Color Doppler sonographic findings in penile fracture. J Clin Ultrasound. 2005; 33: 38-42.
- Koga S, Saito Y, Arakaki Y, et al. Sonography in fracture of the penis. BJU. 1993; 72: 228-229.
- Pariser JJ, Pearce SM, Patel SG, Bales GT. National patterns of urethral evaluation and risk factors for urethral injury in patients with penile fracture. Urology. 2015; 86: 181–5.