
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Evaluation of ultrasonographic findings in adults with cervical lymphadenopathy
M Tarhun Yosunkaya1*; Belma Cevik2
1 Department of ENT, Faculty of Medicine, Lokman Hekim University, Ankara, Turkey.
2 Department of Radiology, Faculty of Medicine, Lokman Hekim University, Ankara, Turkey
*Corresponding Author: M Tarhun Yosunkaya
Lokman Hekim Akay Hospital, Büklüm cad. No:4,
Cankaya/Ankara, Turkey.
Email: tarhun.yosunkaya@lokmanhekim.edu.tr
Received : Oct 04, 2021
Accepted : Dec 03, 2021
Published : Dec 10, 2021
Archived : www.jcimcr.org
Copyright : © Yosunkaya MT (2021).
Abstract
Background and aim: It is very important to distinguish benign and malignant cervical lymph nodes and to make an early diagnosis in terms of treatment and prognosis. Ultrasonography (USG) provides an idea in the diagnosis of reactive or non-reactive lymph nodes but also provides benefits in the differential diagnosis of malignant and benign. It is easily accessible, has high-resolution probes, is inexpensive, does not contain radiation, and serves as a guide in aspiration biopsy when necessary. Although fineneedle aspiration cytology (FNAC) has a high degree of sensitivity and specificity in evaluating cervical lymph nodes, in 20% of patients it may give an ambiguous report that does not contribute to treatment. In this study, ultrasonographic findings of patients with cervical LAP diagnosed with FNAC were evaluated. The value of ultrasonographic examination in diagnosing diseases was emphasized.
Materials and methods: In this study, ultrasonographic findings of 178 patients diagnosed with cervical lymphadenopathy by performing FNAC were examined. Ultrasonographic findings, shape, echogenic hilum, nodal matting, L/S ratio and intranodal necrosis characteristics of cervical nodes were evaluated and compared with FNAC diagnoses.
Results: It was found statistically significant between a reactive node and ultrasonographic oval shape, metastasis and L/S ratio, presence of echogenic hilus and reactive node, nodal matting finding and tuberculosis (p<0.05). Although the presence of necrosis was detected at a higher rate in metastasis and tuberculosis than lymphoma and reactive node, it was not found to be statistically significant (p>0.05).
Conclusion: It is thought that B-mode ultrasonography, which has high specificity and sensitivity, is a successful imaging method and can be used frequently in the differential diagnosis of diseases in all patients presenting with cervical lymphadenopathy. In this way, unnecessary biopsy, excision and further examination examinations are prevented.
Keywords: cervical lenfadenopathy; ultrasonographic findings; adults.
Citation: Yosunkaya MT, Cevik B. Evaluation of ultrasonographic findings in adults with cervical lymphadenopathy. J Clin Images Med Case Rep. 2021; 2(6): 1464.
Introduction
Lymphadenopathy (LAP) is the number, size, shape and structural changes that occur in the lymph nodes, mostly as a result of inflammatory and malignancy. Cervical LAP is a common finding in clinical and radiological examinations, and the most common cause is infections [1,2]. Cervical nodes are also frequent sites of head and neck cancer metastases, lymphoma and tuberculosis. Early diagnosis is very important in terms of treatment and prognosis to differentiate benign and malignant lymph nodes. Because the treatments of diseases are different. Delayed diagnosis may lead to the progression of the diseases and render the treatable lesion incurable [3]. In malignant diseases, the presence of metastatic lymph nodes on the same side reduces the 5-year survival rate by 50%, while the presence of lymph nodes on both sides reduces the survival rate to 25%. Metastatic nodes indicate that the neoplasm is more biologically aggressive in head and neck cancer [4].
Clinical examination is important in the evaluation of cervical lymph nodes in practice, but it is insufficient in distinguishing benign and malignant diseases and in treatment planning [5,6]. There are many imaging methods (USG, CT, MRI) that play a role in distinguishing benign and malignant etiology in cervical LAP. Ultrasonography (USG) is a non-invasive method and a valuable diagnostic tool that has been used for a long time to evaluate cervical lymph nodes. While the location, number, size, hilar echogenicity, intra-nodal necrosis, calcification and marginal features of lymph nodes are evaluated with B mode USG, intranodal distribution and vascular resistance measurements can be made with the use of Doppler usg [7,8]. It has been determined that USG has a higher efficiency in detecting lymph node compared to clinical examination and its sensitivity is 90-97% [9]. Although USG is a very valuable imaging method, histopathological examination with aspiration biopsy is the gold standard in the differential diagnosis of Lap and has high sensitivity (97%) and specificity (93%) [10]. Most clinicians rely on fineneedle aspiration cytology (FNAC) for the evaluation of cervical nodes. Although fine aspiration cytology has a high degree of sensitivity and specificity in evaluating cervical lymph nodes, it may give an ambiguous report that does not contribute to treatment in 20% of patients [11]. In this study, ultrasonographic findings of patients with cervical LAP diagnosed with FNAC were evaluated. The value of ultrasonographic examination in diagnosing diseases was emphasized.
Material and methods
In this retrospective study, 102 male and 76 female (22-69) patients who applied to the ENT clinic due to palpable cervical LAP between 2018-2021 were included. Patients diagnosed with reactive node, lymphoma, metastasis and tuberculosis as a result of FNAC were included in the study. Ultrasonographic findings of patients diagnosed with FNAC were retrospectively investigated. Shape, echogenic hilum, nodal matting, L/S ratio, intranodal necrosis characteristics of ultrasonographic cervical nodes were evaluated and compared with FNAC diagnoses.
GE logic S7 B mode USG device was used in the patients. The patients were examined by the same ENT specialist, and ultrasounds were performed by the same radiologist. The shape of the lymph nodes was assessed by the L/S (long axis/short axis) ratio. An L/S ratio <2 indicates a round node where as an L/S ratio >2 indicates an oval or elongated node. The results of the study were evaluated using a statistical analysis program (Statistical Package for the Social Sciences (SPSS) version 22.0, SPSS Inc. Chicago, IL, USA). Chi-Square test was used to assess the differences between groups. Statistical significance level accepted as p<0.05.
Results
In the study, ultrasonographic findings of 178 (102 men, 76 women) patients (Table 1) who were diagnosed with reactive node (67%), lymphoma (14%), metastasis (13%) and tuberculosis (6%) in FNAB due to cervical LAP were evaluated (Figures 1-4).
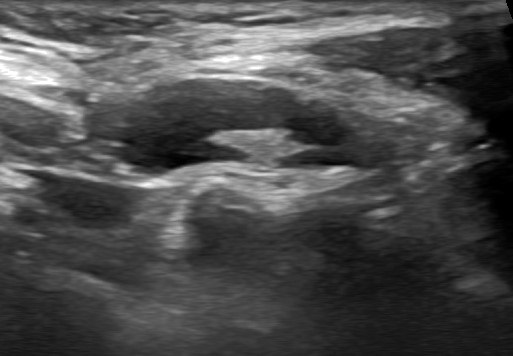
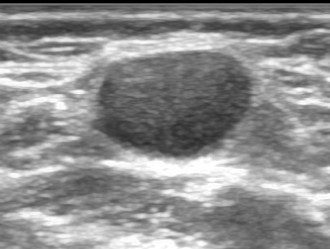
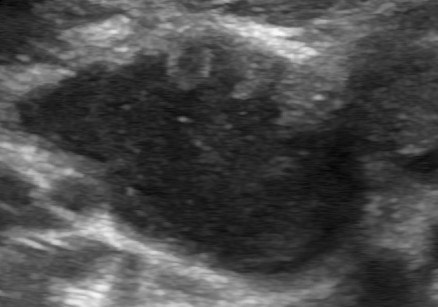
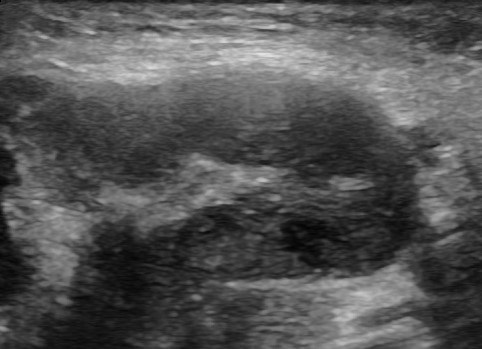
Table 1: Distribution of patients diagnosed with FNAC.
Results of FNAC (n=178) |
n |
Reactive node |
119 (67%) |
Lymphoma |
25 (14%) |
Metastasis |
23 (13%) |
Tuberculosis |
11 (6%) |
When the shapes of the cervical lymph nodes were evaluated ultrasonographically, 108 (91%) of the reactive lymph nodes were oval, while 11 (9%) were found to be round. In lymphoma, 7 (28%) are oval, 18 (72%) are round, in metastases 6 (26%) are oval, 17 (74%) are round, in tuberculosis 3 (27%) are oval, 8 (73%) are round found (Table 2). The relation between the reactive node and the ultrasonographic oval shape was statistically significant (p<0.05).
Table 2:Distribution of ultrasonographic shape finding according to diseases.
Shape (n) |
Ovale |
Round |
Reactive node |
108 (91%) |
11 (9%) |
Lymphoma |
7 (28%) |
18 (72%) |
Metastasis |
6 (26%) |
17 (74%) |
Tuberculosis |
3 (27%) |
8 (73)% |
As a result of the ultrasonographic evaluation of the shapes of the cervical lymph nodes, 108 (91%) of the reactive lymph nodes were oval, while 11 (9%) were found to be round. In lymphoma 7 (28%) oval, 18 (72%) round, in metastasis 6 (26%) oval, 17 (74%) round, in tuberculosis 3 (27%) oval, 8 (73%) round found (Table 2). The relation between the reactive node and the ultrasonographic oval shape was statistically significant (p<0.05).
When the L/S ratio of cervical lymph nodes was evaluated, it was found 2.3 ± 0.8 in reactive node, 1.6 ± 0.3 in lymphoma, 1.3 ± 0.5 in metastasis, 1.8 ± 0.4 in tuberculosis (Table 3). The relation between metastasis and L/S ratio was statistically significant since values above 2 L/S ratio were considered malignant (p<0.05).
Table 3:Distribution of ultrasonographic L/S ratio according to diseases.
L/S ratio |
Mean |
Reactive node |
2,3± 0,8 |
Lymphoma |
1,6± 0,3 |
Metastasis |
1,3± 0,5 |
Tuberculosis |
1,8 ± 0,4 |
The presence of echogenic hilum was examined. While it was positive in 110 (92%) reactive nodes, it was negative in 9 (8%) nodes. In lymphoma positive 5 (20%), negative 20 (80%), metastasis positive 2 (9%), 21 (91%) negative. In tuberculosis, 1 (10%) positive and 10 (90% negative) were found (Table 4) The relation between the presence of echogenic hilum and reactive node was statistically significant (p<0.05).
Table 4:Distribution of ultrasonographic echogenic hilus presence according to diseases.
Echogenic hilum |
Positive |
Negative |
Reactive node |
110 (92%) |
9 (8%) |
Lymphoma |
5 (20%) |
20 (80%) |
Metastasis |
2 (9%) |
21 (91%) |
Tuberculosis |
1 (10%) |
10 (90% |
The nodal matting sign was positive in 5 (4%) reactive nodes and negative in 114 (96%) nodes. In lymphoma 2 (8%) positive, 23 (92%) negative, in metastasis 1 (4%) positive, 22 (96%) negative, in tuberculosis 9 (82%) positive and 2 (18%) negative (Table 5). The relation between nodal matting finding and tuberculosis was statistically significant (p<0.05).
When the finding of necrosis was investigated (Table 6), necrosis was not observed in any of the reactive nodes and lymphomas, while it was found 18 (78%) positive, 5 (22%) negative in metastasis, 7 (63%) positive and 4 (37%) negative in tuberculosis. Although the presence of necrosis was detected at a higher rate in metastasis and tuberculosis than lymphoma and reactive node, it was not found to be statistically significant (p>0.05).
Discussion
Reactive node, lymphoma, metastasis and tuberculosis are common causes of cervical LAP. USG provides an idea about the diagnosis of reactive or non-reactive lymph nodes, as well as provides usefulness in the differential diagnosis of benign and malignant diseases [12,13]. In our study, the relation between a reactive node and ultrasonographic oval shape, between metastasis and L/S ratio, between the presence of echogenic hilus and reactive node, between nodal matting finding and tuberculosis was found statistically significant (p<0.05). The presence of necrosis was detected at a higher rate in metastasis and tuberculosis compared to lymphoma and reactive node, but it was not found to be statistically significant (p>0.05).
USG has features such as easy accessibility, high-resolution probes, being inexpensive and free of radiation, and serving as a guide in aspiration biopsy when necessary. Although FNAC is a valuable diagnostic method, it also has some disadvantages. Tuberculous lymph nodes may be reported as reactive or granulomatous lymphadenitis. This result leaves clinicians hesitant to start tuberculosis treatment. Similar problems may arise in the evaluation of metastatic lymph nodes. While the lymph node selected during the procedure has an inflammatory feature, the features carrying the disease may be in other lymph nodes. Apart from that, FNAC is also unreliable in differentiating between metastatic and lymphomatous lymph nodes. However, a biopsy from cervical lymph nodes is often difficult. Due to their small size, the vascular structures around the node may be damaged during the procedure [14,15]. USG has high sensitivity when compared with clinical examination (92% and 70% respectively) and high specificity when combined with FNAC (95%) [16,17].
Ahuja et al. reported that B mode usg was 96.8% successful in differentiating benign-malignant cervical pathology round shape, contour lobulation, hilus echogenicity and presence of necrosis and size play an important role in the differentiation of malignant and benign lymph nodes [18].
The shape of lymph nodes has been used to differentiate normal or reactive nodes from malignant nodes. The abnormal shape is a consistent finding in differentiating reactive nodes from other abnormal nodes [9,10]. Metastatic, lymphomatous and tuberculous nodes commonly appear round with an L:S ratio ≤2, whereas normal or reactive nodes are usually oval shaped with L:S ratio ≥2. Metastatic nodes are ultrasonographically characterized by a smaller long axis to short axis ratio (L/S ratio), absence of hilus and a hypoechoic center. Steinkamp HJ et al report that 95% of metastatic nodes had L/S ratio of less than 2 . The ultrasonographic characteristics of tubercular lymph nodes are multiple lymph nodes, fusion tendency of adjacent nodes and a hypoechoic center with posterior enhancement. An additional feature, which has great specificity for tubercular lymphadenitis is strong echoes within the mass. The strong echoes are calcification within the node [19-22]. Metastatic nodes may look homogeneous or heterogeneous. Lymph nodes involved with lymphoma usually look homogeneous, and tuberculous nodes are commonly heterogeneous. Malignant nodes, such as metastases and lymphoma tend to have sharp borders, whereas benign nodes (reactive node and tubercular) usually have unsharp borders [23-26]. The presence of a central echogenic hilus within lymph nodes is usually considered as a sign of benignity, but lymphomatous and tuberculous nodes tend to have absent hilus [27].
In studies, lymph nodes with positive round shape, loss of hilar echogenicity, contour lobulation and presence of necrosis according to B mode ultrasound findings in the differential diagnosis of cervical lymph nodes were accepted as malignant, and as a result, 75-94% sensitivity and 82-94% specificity were reported [28]. In studies, it has been stated that when the malignant process progresses, there will be an increase in nodal size and the shape of the lymph node will become round [29,30]. In the study of Rubaltelli et al, the presence of central echogenicity alone was evaluated in the differentiation of malignant and benign lymph nodes. It is stated that the central echogenicity finding indicates malignancy. They found that, there was no echogenic hilus in any of the malignant lymph nodes, while the presence of 83% echogenic hilus in the benign lymph nodes was detected [31]. Contrary to this study, Evans et al. suggested that echogenic hilum is not a reliable parameter for benign nodes and that it can be seen in 58% of malignant nodes [32].
Conclusion
It is thought that B-mode ultrasonography, which has high specificity and sensitivity, is a successful imaging method and can be used frequently in the differential diagnosis of diseases in all patients presenting with cervical lymphadenopathy. In this way, unnecessary biopsy, excision and further examination examinations are prevented.
References
- Park JE, Ryu YJ, Kim JY, Kim YH. et al. Cervical lymphadenopathy in children: A diagnostic tree analysis model based on ultrasonographic and clinical findings. 2020; 30(8): 4475-4485.
- Bazemore AW, Smucker D.R.American Family Physician. 2002; 66: 2103-10.
- Haque MA, Talukder SI: Evaluation of fine needle aspiration cytology (FNAC) of lymphnodes in (Mymensingh. Mymensingh Med J. 2003; 12(11): 33-5.
- Som PM. Lymphnodes of the neck. Radiology. 1987; 165: 593- 600.
- Lee YY, Van Tassel P, Nauert C, North LB, Jing BS. Lymphomas of the head and neck: CT findings at initial presentation. Am J Roentgenol.1987; 149(3): 575–581.
- Reede DL, Bergeron RT. Cervical tuberculous adenitis: CT manifestations. RADİOLOGY.1985; 154(3): 701–704.
- Ahuja A, Ying M. An overview of neck node sonography. Invest Radiol. 2002; 37: 333-42 (2.5)
- Ahuja A, Ying M. Sonographic evaluation of cervical lymph nodes. AJR Am J Roentgenol. 2005; 184: 1691-9.
- Luigi S, Giorgio R. Ultrasound of Superficial Structures. Edinburg, Churchil Livingstone. 1995; 517-29.
- Van den Brekel MW, Castelijns JA,Stel HV, Luth WJ, et al. Occult metastatic neck disease: detection with US and US-guided fineneedle aspiration cytology. Radiology. 1997; 180: 457-61.
- Ahuja A, Ying M,Ho SY, et al.Ultrasound of malignant cervical lymph nodes. Cancer Imaging. 2008; 8: 48-56.
- Pattanayak S, Chatterjee S, Ravikumar R, Nijhawan VS, Vivek Sharma, Debnath J. Ultrasound evaluation of cervical lymphadenopathy: Can it reduce the need of histopathology/ cytopathology? Med J Armed Forces India. 2018 ; 74(3): 227- 234.
- Prativadi R, Dahiya N, Kamaya A, Bhatt S. Chapter 5 Ultrasound Characteristics of Benign vs Malignant Cervical Lymph Nodes. Semin Ultrasound CT MR. 2017; 38(5): 506-515.
- Ying M, Ahuja A, Evans R, et al: Cervical lymphadenopathy: sonographic differentiation between tuberculous nodes and nodal metastases from non-head and neck carcinomas. J Clin Ultrasound. 1998; 26: 383-389.
- Asai S, Miyachi H, Suzuki K, Shimamura K, Ando Y: Ultrasonographic differentiation between tuberculous lymphadenitis and malignant lymphnodes. J Ultrasound Med. 2001; 20: 533-538.
- Bruneton JN, Roux P, Caramella E, Demard F, et al. Ear, nose and throat cancer: ultrasound diagnosis of metastasis to cervical lymph nodes. Radiology. 1984; 152: 771-773.
- Gooding GA. Malignant carotid invasion: sonographic diagnosis. J orinolaryngol Relat Spec. 1993; 55: 263-272.
- Ahuja AT, Ying M, Ho SY, et al. Ultrasound of malignant cervical lymphnodes. Cancer IMAGING. 2008; 8(1): 48–56.
- Steinkamp HJ, Cornehl M, Hosten N, Pegios W, Vogl T, Felic R: Cervical lymphadenopathy: ratio of long to short axis diameter as a predictor of malignancy. Br J Radiol. 1995; 68(807): 266-70.
- Ying M, Ahuja A, Evans R, et al: Cervical lymphadenopathy: sonographic differentiation between tuberculous nodes and nodal metastases from non-head and neck carcinomas. J Clin Ultrasound. 1998; 26: 383-389.
- Asai S, Miyachi H, Suzuki K, Shimamura K, Ando Y: Ultrasonographic differentiation between tuberculous lymphadenitis and malignant lymph nodes. J Ultrasound Med. 2001; 20: 533-538.
- Brucoli M, Borello G, Boffano P, Benech A. Tuberculous neck lymphadenopathy: A diagnostic challenge. J Stomatol Oral Maxillofac Surg. 2019; 120(3): 267-269.
- Chang DB,YangPC, LuhKT, etal. Ultrasonic evaluation of cervical lymphadenopathy. J Formos Med Assoc.1990; 88: 286-292.
- Lee N, Inoue K, Yamamoto R. Patterns of internalechoes in lymphnodes in the diagnosis of lung cancer metastasis. World J Surg 1992; 16: 986-993.
- J.N. Bruneton, F. Normand, C. Balu-Maestro et al. Lymphomatous superficial lymphnodes: US detection. Radiology.1987; 165: 233-235.
- Pombo F, Rodriguez E, Mato J. Patterns of contrast enhancement of tuberculous lymphnodes demonstrated by computed tomography. ClinRadiol. 1992; 46: 13-17.
- R. M. Evans, A. Ahuja, C. Metreweli. The linear echogenichilusin cervical lymphadenopathy-asign of benignity or malignancy? ClinRadiol. 1993; 47: 262-264.
- Ahuja A, Ying M. An overview of neck node sonography. Invest Radiol. 2002; 7: 333-42.
- Vassallo P, Wrnecke K, Roos N, Peters PE. Differentiat in of benign from malignant superficial lymphadenopathy: the role of high resolution US. Radiology. 1992; 183: 215-20.
- Wu CH, Chang YL, Hsu WC, Ko JY, et al. Usefulness of Doppler spectral analysis and power Doppler sonography in the differention of cervical lymphadenopathies. AJR Am J Roentgenol. 1998; 171: 503-9.
- Rubaltelli L, Prota E, Salmaso R, Bortoletto P, at al. Sonography of abnormal lymph nodes in vitro : correlation of sonographic and histologic findings. Am J Roentgenol. 1990; 155(6): 1241-44.
- Evans Rm, Ahuja A, Metreweli C. The linear echogenic hilus in cervical lymphadenopathy a sign of benignity or malignancy ? Clin Radiol. 1993; 47(4): 262-64.