
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Hypercalcemia and multiple osteolytic bone lesions: A rare presentation of acute lymphoblastic leukemia
Shirin Haghighat1*; Aliasghar Karimi2
1 Hematology and Medical Oncology Department, Shiraz University of Medical Science, Shiraz, Iran.
2 Non-Communicable Diseases Research Center (NCDRC), Fasa University of Medical Science, Fasa, Iran.
*Corresponding Author: Shirin Haghighat
Hematology and Medical Oncology Department,
Namazi Hospital, Shiraz University of Medical Science,
Z and Avenue, Iran.
Email: sh.haghighat2010@yahoo.com
Received : Oct 16, 2021
Accepted : Dec 03, 2021
Published : Dec 10, 2021
Archived : www.jcimcr.org
Copyright : © Haghighat S (2021).
Abstract
Hypercalcemia and osteolytic bone lesions are rare initial presentation of adult Acute Lymphoblastic Leukemia (ALL). This presentation is mainly described in pediatric ALL and information about adult ALL-associated hypercalcemia is limited. We describe a 21 years old woman presented with acute kidney injury, hypercalcemia and osteolytic bone lesions who was later diagnosed to have pre-B ALL. After correction of hypercalcemia and acute kidney injury by intravenous fluid administration, calcitonin, corticosteroid and eventually hemodialysis, the patient was treated by induction chemotherapy followed by complete remission. Unfortunately, she refused hematopoietic stem cell transplantation and relapsed three months after the last cycle of induction chemotherapy and died. In conclusion, this is a rare case report of hypercalcemia and osteolytic bone lesions as an initial presentation of pre-B cell ALL at early adulthood which showed the aggressive behavior and early relapse. So further investigations are needed to establish the role of this initial presentation in the prognosis of patients with ALL.
Keywords: ALL; hypercalcemia and osteolytic bone lesions.
Citation: Haghighat S, Karimi A. Hypercalcemia and multiple osteolytic bone lesions: A rare presentation of acute lymphoblastic leukemia. J Clin Images Med Case Rep. 2021; 2(6): 1467.
Introduction
Malignancy-related hypercalcemia affects 10-30% of all patients with malignancy during the course of their disease [1]. It is clear that hypercalcemia is particularly common in cases of advanced cancer and associated with poor prognosis [2]. This condition is seen in both hematologic and solid malignancies with the foremost common being myeloma, lymphoma, leukemia, breast carcinoma, lung cancer, and renal cell carcinoma [3]. Major underlying mechanisms of hypercalcemia of malignancy are increased tumor secretion of Parathyroid HormoneRelated Peptide (PTHrP), osteolytic bone destruction, tumoral production of 1,25 dihydroxy vitamin D and proinflammatory cytokines [Tumor Necrosis Factor-Alpha (TNFα) and Interlukins (IL)] and Production Of Parathyroid Hormone (PTH) [4,5]. Acute Lymphocytic Leukemia (ALL) presenting with hypercalcemia in conjunction with osteolytic bone lesion could be a rare event, however, most of them are characterized in children affected by B-ALL [6-9]. This condition could be a rare initial manifestation of adult ALL and limited to only some cases reports in the world [10,11]. Here we describe a 21 years old woman presenting with leg pain, hypercalcemia and Acute Kidney Injury (AKI).
Case presentation
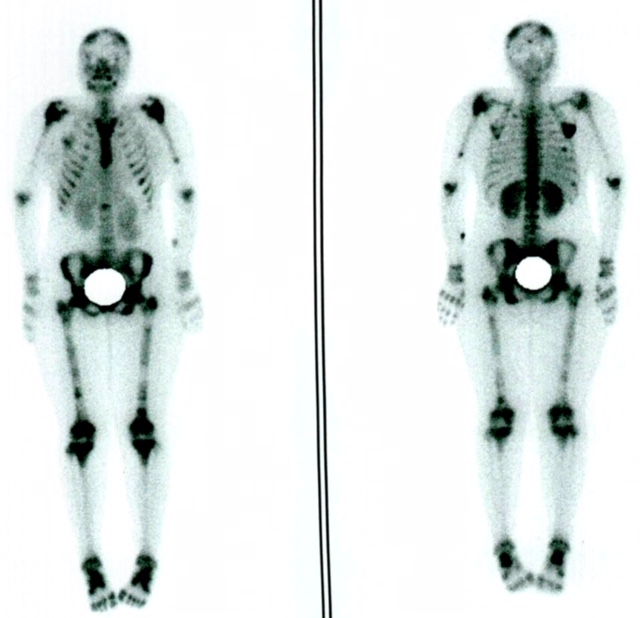
A 21 years old woman presented with both leg pain and weakness brought up to our hospital due to anemia. Her complaints started two months earlier and failed to respond to rest and analgesics. The patient’s medical and family history was unremarkable. In physical examination, diffuse tenderness of pelvic bone and lumbar vertebrae was detected. Initial laboratory studies revealed white blood cell (WBC) of 4900/μl with normal differential, hemoglobin of 5.7 g/dl (normal range 12- 16 g/dl female), platelets of 172000/μl, creatinin of 2.3 mg/dl (normal range 0.6-1.2 mg/dl female), calcium of 15 mg/dl (normal range 8.8-10.2 mg/dl), lactate dehydrogenase of 1880 IU/L (normal range 100-190 IU/L) and PTH of 8 pg/ml (normal range 10-55 pg/ml). The value of liver enzymes and other electrolytes were in normal ranges. Also, severe normocytic anemia was diagnosed in peripheral blood smear, so bone marrow aspiration and biopsy was done. The cellular marrow containing over 70% blast was consistent with pre-B ALL according to flow cytometry markers. The routine management of hypercalcemia including intravenous fluid, corticosteroid, calcitonin and diuretic was started immediately but in continues, the serum calcium level failed to significantly change so hemodialysis was done which was effective in normalization of serum calcium level and renal function. Additionally, whole-body bone scan after injection of 20 mCi Tc-99m-MDP showed multiple areas of increased radiotracer uptake within the skull, spine, both scapula, both humeral bones and both femoral bones in keeping with tumoral infiltration (Figure 1). Regarding the diagnosis of ALL the patient received induction chemotherapy (HyperCVAD protocol) followed by complete remission. Since the patient refused allogeneic hematopoietic stem cell transplantation despite counseling, maintenance chemotherapy (mercaptopurine and methotrexate) was administered. Following three months of maintenance chemotherapy, she was admitted with relapse of ALL and received salvage chemotherapy. Unfortunately, complete remission failed to occur and the patient died 2 months after relapse.
Discussion
Although hypercalcemia associated with osteolytic bone lesions is a common complication of adult malignancies it is a rare presentation of ALL. Most information regarding the incidence of hypercalcemia and osteolytic bone lesions related to ALL comes from reports in pediatric patients. Within the largest series, related to St Jude Children's Research Hospital, only 0.3% of patients with lymphohematopoietic malignancy had presented with hypercalcemia. 12 Pediatric ALL patients presenting with osteolytic bone lesion and hypercalcemia seem to be older and have a lower White Blood Cell (WBC) count and circulating blast [13]. Our patient also did not have any blast cell in peripheral blood. Inukai et al. retrospectively analyzed 22 cases of childhood ALL associated with hypercalcemia and revealed five patients with t (17;19) ALL. They found the incidence of this cytogenetic abnormality was more than 20%, suggesting the common association of t (17;19) with event of hypercalcemia in ALL patients. In this study excluding t (17;19) ALL who relapsed very early, the prognosis of ALL patients presented with hypercalcemia was like other patients with ALL without hypercalcemia [14]. Unfortunately, in our patient, possible cytogenetic abnormality was not detected due to low specimen cell yield. Because we did not carry out PTHrP and IL testing, the underlying mechanism of hypercalcemia and osteolysis in this patient could not be established.
Conclusion
This case shows the rare association of hypercalcemia and osteolytic bone lesions with the initial presentation of ALL. Although this presentation is not common in adults, possibly is often a crucial prognostic factor and identify patients in danger of early relapse. However further investigations are required to determine the prognostic implication of this presentation.
Declarations
Patient consent: The authors declare that informed consent was taken for this study.
References
- Rosner MH., Dalkin AC. Onco-nephrology: The Pathophysiology and Treatment of Malignancy-Associated Hypercalcemia. Clin J Am Soc Nephrol. 2012; 7: 1722–1729.
- Goldner W. Cancer-related hypercalcemia. J Oncol Pract. 2016; 12: 426-432.
- Sternlicht H, Glezerman IG. Hpercalcemia of malignancy and new treatment options. Ther Clin Risk Manag. 2015; 11: 1779- 1788.
- Mirrakhimov AE. Hypercalcemia of Malignancy: An Update on Pathogenesis and Management. N Am J Med Sci. 2015; 7: 483- 493.
- Sohi R, Sheppard G. Hypercalcemia of malignancy: an emergency medicine simulation. Cureus. 2017; 9: e1847.
- Lokadasan R, Prem S, Koshy SM, Jayasudha AV. Hypercalcaemia with disseminated osteolytic lesions: a rare presentation of childhood acute lymphoblastic leukaemia. Ecancermedicalscience. 2015; 9: 542.
- Oliveira CC., Kucko L., Hirama EJ., Guerra HM., Terra SA., Santiago LM., et al. Acute lymphoblastic leukemia: primary bone manifestation with hypercalcemia in a child. J Bras Patol Med Lab. 2017; 53: 61-64.
- Oloomi Z. Acute lymphoblastic leukemia without circulating blasts presenting as severe hypercalcemia. Acta Medica Iranica. 2007; 45: 76-78.
- Madhu BJ, Chithambaram NS, Harish G, Vijaya S. Atypical Presentation of Acute Lymphoid Leukemia as Hypercalcemia and Bilateral Renal Calculi. Glob J Endocrinol Metab. 2018; 2: 1-2.
- Granacher NCP, Berneman ZN, Schroyens W, Van de Velde ALR, Verlinden A, Gadisseur APA. Adult acute precursor B-cell lymphoblastic leukemia presenting as hypercalcemia and osteolytic bone lesions. Exp Hematol Oncol. 2017; 6: 9.
- Mahmood K, Ubaid M, Taliya Rizvi S. Multiple Osteolytic Lesions Causing Hypercalcemia: A Rare Presentation of Acute Lymphoblastic Leukemia. Case Rep Med. 2017; 2017: 1-3.
- McKay C, Furman WL. Hypercalcemia complicating childhood malignancies. Cancer. 1993; 72: 256-260.
- Trehan A, Cheetham T, Bailey S. Hypercalcemia in acute lymphoblastic leukemia: an overview. J Pediatr Hematol Oncol. 2009; 31: 424-427.
- Inukai T, Hirose K, Inaba T, Kurosawa H, Hama A, Inada H, et al. Hypercalcemia in childhood acute lymphoblastic leukemia: frequent implication of parathyroid hormonerelated peptide and E2A-HLF from translocation 17; 19. Leukemia. 2007; 21: 288- 296.