
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Generalized eruptive keratoacanthomas involving the auricles and external auditory canal: A case report and literature review
Lu Zhang1#; Haiying Sun2#; Dakai Lu1*
1 Department of Otorhinolaryngology, Hwa Mei Hospital, University of Chinese Academy of Sciences & Ningbo Institute of Life and Health Industry, University of Chinese Academy of Sciences, Ningbo 315000, Zhejiang, China
2 Department of Otorhinolaryngology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, China.
#Equal contribution: Lu Zhang & Haiying Sun
*Corresponding Author: Da-kai Lu
Department of Otorhinolaryngology, Hwa Mei
Hospital, University of Chinese Academy of Sciences
& Ningbo Institute of Life and Health Industry, University of Chinese Academy of Sciences, Ningbo 315000,
Zhejiang, China.
Email: nbldkai@163.com
Received : Oct 12, 2021
Accepted : Dec 06, 2021
Published : Dec 13, 2021
Archived : www.jcimcr.org
Copyright : © Lu DK (2021).
Abstract
Objective: The aim of this study was to report a case of Generalized Eruptive Keratoacanthomas (GEKA) involving the auricles and external auditory canal and to review the relevant literature.
Methods: A patient with bilateral auricles stenosis and External Auditory Canal (EAC) atresia associated with GEKA is described. We performed a systematic review of the literature to identify and compare similar cases.
Results: This case report described a 54-year-old female patient with external auditory canal stenosis and auriclelesion associated with GEKA. A Computed Tomography scan (CT) of the temporal bone.
Conclusion: Bilateral auricles stenosis and atresia of EAC associated with GEKA is a rare case. It provides a new perspective for the etiological diagnosis of acquired auricles lesion as well as stenosis and atresia of EAC in the future. The surgical strategy is necessary for the management of the acquired stenosis and atresia of the EAC that associated with GEKA. Further research is needed to increase the number of clinical cases to establish whether and when the surgery is necessary for this disease.
Keywords: keratoacanthoma; auricles lesion; ear canal; stenosis; atresia.
Citation: Zhang L, Sun H, Lu DK. Generalized eruptive keratoacanthomas involving the auricles and external auditory canal: A case report and literature review. J Clin Images Med Case Rep. 2021; 2(6): 1469.
Introduction
Keratoacanthoma (KA) is a common cutaneous skin tumor that originates from the hair follicles. It is characterized by unproven position on the border between malignancy and benignity [1]. Solitary KA is the most common form but familial multiple KA, genetically predisposed KA or sporadic multiple eruptive KA also have been described [1]. Generalized Eruptive Keratoacanthomas (GEKA) is an extremely rare condition. Both cutaneous and mucosal are involved in GEKA without certain genetic background. Approximately 40 cases have been reported [2]. But so far, there is no case report of auditory organs lesion associated with GEKA. Here in, we report a rare female case. To our knowledge, this is the first report describing a case of GEKA with external auditory canal stenosis and auricle lesion. We hope this previously uncharacterized clinical association may provide additional in sight on management.
Case report
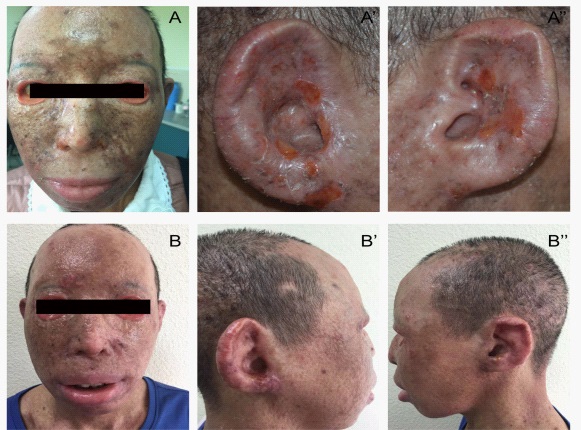
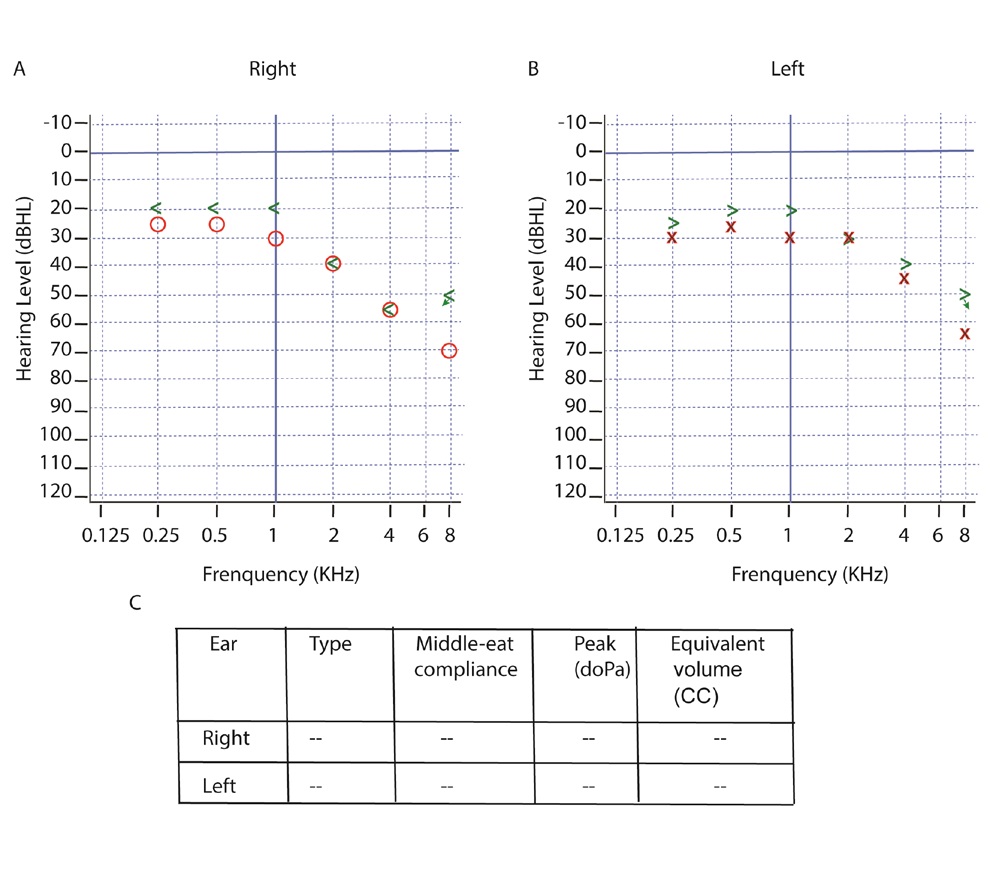
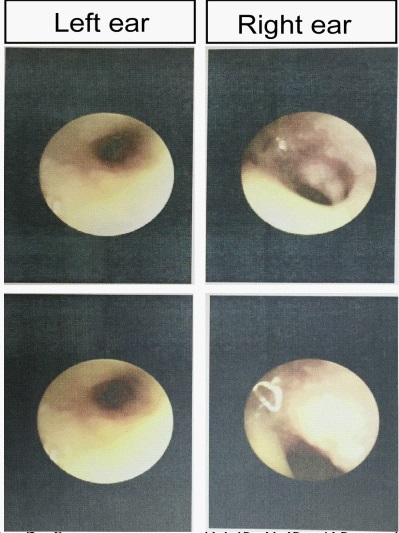
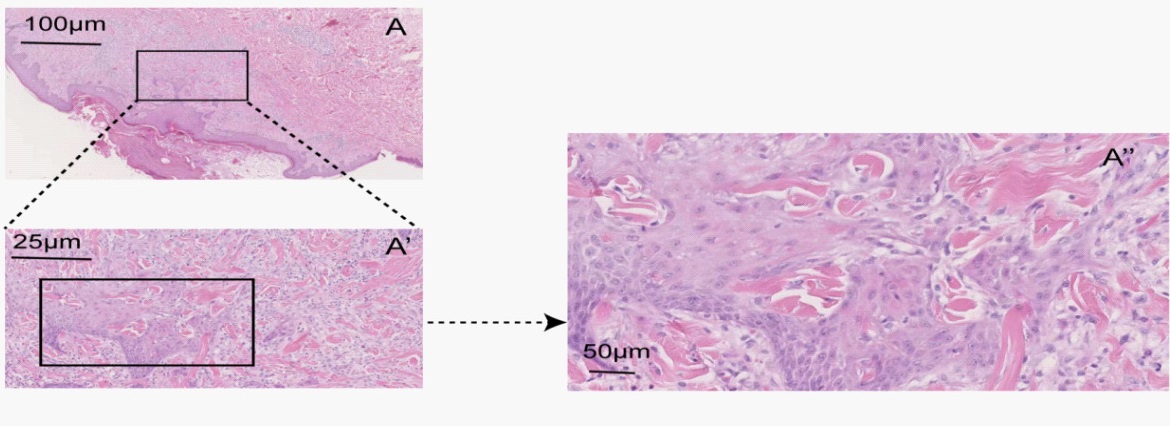
A 54-year-old female patient transferred to the clinic of otorhinolaryngology because of congestion, swelling and lesion of bilateral auricles in December 2018. Her past medical history was unremarkable. She experienced a sudden onset of some scaly papules located on her ears without any identified trigger. There was no history of similar skin disease in her family and the history of ear trauma, chronic inflammation and chemical exposure were all denied. A few months, the lesion was widespread in the whole body, but the enlarged superficial lymph nodes of the whole body were not found. Histopathological examination of the specimen obtained from the patient’s head demonstrated keratinocytes were surrounded by more inflammatory infiltrate and the cells become larger (Figure 1 A-A’’). According to the typical symptoms and histopathological examination the patient was diagnosed as GEKA after admitted to the department of dermatology in December 2016. Then she was followed up by the dermatologist for along time. The dermatologist gave cephalosporin antibiotics and topical corticosteroids to prevent infection and local inflammation. However, the above symptoms improved. The congestion, swelling and lesion of bilateral auricles were aggravated, with obvious hearing loss and ear fullness. The patient was urgently referred to the clinic of otorhinolaryngology for further diagnosis and treatment. The physical examination revealed sclerotic and mask-like facies with marked bilateral eyelid ectropion (Figure 2A); Auricular lesions exhibited congestion and swelling, erythematous papules and keratoacanthoma-like nodules. Structures such as triangular fossa, ear nail boat, opposite tragus, opposite ear wheel disappeared (Figure 2 A’, A’’). There is nothing special else. Otoscopy revealed stenosis of the EAC and intact tympanic membrane of bilateral ear (Figure 3). At the sametime the tuning fork test was performed: Rinner test of bilateral ear was positive, Weber test sound was heard equally loudly in both ears. Pure tone audiometry revealed sensori neural hearing loss at Frequencies of 2 kHZ, 4 kHZ and 8 kHZ (Figure 4A,B), and there were no tympanometry findings (Figure 4C). At this point, a CT scan was taken in order to complete the auditory canal evaluation (Figure A-A’). Furthermore, upon examination, there was no history of vertigo, tinnitus or facial nerve weakness.
Laboratory evaluation showed anti-thyroglobulin antibody >500 IU/ml (normal <60 IU/ml), anti-peroxidase antibody > 1300 IU/ml (normal < 60 IU/ml). Human Papillomavirus (HPV) DNA, Treponema pallidum and HIV antibodies were all negative on the skin lesions. The antinuclear antibody was 1:320. The anti-SS and anti-Ro antibody was both positive. Chest CT showed no obvious abnormality in the lungs. The patient is suspected to have a history of dry mouth and eyes, and denies the history of joint pain. Sjogren's syndrome could not be excluded since she refused to undergo further examination such as lip gland biopsy.
History of drug treatment: After diagnosed as GEKA, the patient was treated with 30 mg oral isotretinoin, 0.1% tretinoin ointment externally. However, the disease continued to progress and the dose of acitretin was increased to 40 mg/day. Congestion and swelling of bilateral auricle turned better through antibiotics and anti-inflammation treatment. The occurrence of ear fullness and hearing loss was not taken seriously. The auricle lesion continued to progress, but no pathological examination of auricle lesion was given. The dose of acitretin was increased to 50 mg/day, while cyclophosphamide was given by intravenous pulse therapy, with 600 mg once monthly, 6 months as one course of treatment. There were no reports and clinical evidence of auricle lesion, stenosis and atresia of EAC and hearing loss associated with the above drugs. There is no history of drug-induced and noise-induced hearing loss.
First year follow-up: On November 25, 2019, the patient visited to the clinic of otorhinolaryngology for the first-year followup. She complained that the fullness and hearing loss of bilateral ear were more serious than before. Physical examination revealed the mask-like facial expression and marked ectropion were the same with one year before (Figure B). The congestion, swelling and lesion of the auricle were almost no development (Figure B’,B’’). However, the EAC became narrower. Cerumen embolism could be seen at the external orifice of the EAC and we could not see the tympanic membrane because of the narrowed EAC. CT scan revealed minimum anteroposterior diameter of EAC (Right ear: 3.05 mm. Left ear: 3.25 mm) thickening of soft tissue in the bilateral EAC especially near the tympanic membrane (Figure B,B’).
The patient was continuously given regular follow-up. However, she died of multiple organ failure syndrome on November 20, 2020.
Discussion
The occurrence of KA in the ear is very rare. At present, only 2 cases of auricle KA have been reported, both of which are regional and well treated after surgical resection [3,4]. However, there is no report of GEKA in the ear and its related lesions. Therefore, it is the first case report of bilateral auricles lesion and stenosis and atresia of EAC associated with GEKA.
Management of acquired stenosis of EAC.
The surgical techniques used in the management of acquired stenosis of EAC have varied over the years [5,6]. In the early years, it was suggested to widen the bony canal by excision of the stenotic tissue. Adkins et al covered the skin-deficient canal with a transposition flap in eight cases, with no recurrence [7]. Moore et al lined the canal with a full thickness skin graft in one case that not recurrence [8]. Mc Donald et al used a split thickness skin graft in 22 cases, with two recurrence [9]. Bell used bilateral rotation skin flaps in 9 cases, with no recurrence [10]. Mc Cary et al used split thickness grafts in 18 cases, with one recurrence [11]. However, it seems that the use of skin flaps or grafts is not necessary in acquired stenosis, unlike acquired atresia. More recent studies have demonstrated that a meatoplasty alone is sufficient to treat acquired stenosis. Once the anatomical narrowing has been corrected by enlargement of the canal and excision of the thickened tissue in acquired stenosis, the condition of the ear is stable. This would suggest that the normal function of EAC is restored, enabling a normal cycle of ear cleaning and preventing poor canal patency leading to inflammatory episodes [12].
Management of acquired atresia of EAC
EAC atresia can be divided into congenital or acquired. Otitis externa is the most common cause of acquired EAC [13]. Males are generally more likely to be diagnosed with acquired EAC, with a male: female ratio of 2-3:1 [13]. In acquired atresia, patients’ main complaint was hearing loss. Surgery was aimed at improving this deficit by restoring and maintaining the patency of the ear canal. Compared with surgical outcomes for acquired stenosis, those for acquired atresia were not good. In many cases, a hearing aid may be a better alternative. Surgical techniques for the management of acquired atresia have evolved since 1966. All agree that removing the fibrous plug alone is inadequate. Unlike acquired stenosis, the denuded canal wall should not be allowed to granulate, as this will lead to recurrence of the atresia; some form of canal lining is required. Different techniques have been used including transposition flaps, full thickness skin grafts and split skin grafts, but all used techniques have some degree of recurrence [13,14]. Regardless of technique used, recurrence has been seen at 6-month, 1- year, 3- years and 9- years. This demonstrates that acquired atresia produces an instable ear canal, but whether this is secondary to the underlying disease process or due to the operative procedure, or a combination of both is still unclear. Long-term follow up is required.
In this case, erythematous papules and nodules are widely seen in the skin of the whole body, causing irreversible skin lesions, especially in exposed areas such as the face, and the failure rate of skin transplantation is high. For acquired stenosis and atresia of EAC in the patient, the use of the above treatments may not be able to achieve better long-term results, and the patient's GEKA is still in progress, which brings more difficulties and challenges to our treatment.
New insights into the management of the acquired stenosis and atresia of the EAC
Nowadays, none of the publications found in the literature addresses the possibility of an underlying systemic etiology when managing this condition. Acquired atresia of the EAC is often regarded as a regional disorder and it is usually managed. However, when we consider the possibility of underlying systemic causes, the theoretical basis that supports current treatments will change, with the goal of correcting underlying conditions, such as immune-mediated diseases or other diseases. Obviously, extensive examination is not required when the clinical cause is clear (traumatic, postoperative, recurrent otitis media). When a tumor is suspected, appropriate radiological and pathological examinations are recommended. When the cause is unknown, we recommend a complete test and ANA screening. If the initial laboratory examination is tough, a biopsy from the EAC is required before surgical treatment. The patient refuses ear biopsy, which is very regrettable for the accurate diagnosis and management of the disease [6].
Conclusion
Case of bilateral auricles lesion and stenosis and atresia of EAC associated with GEKA is very rare. But it provides a new insight into the etiological diagnosis of acquired stenosis and atresia of EA. The surgical strategy for the management of the acquired stenosis and atresia of the EAC consists of the excision of the fibrous plug, application of the cutaneous flaps and/ or transplants to cover the bare parts of the bone portion of the affected external canal. Even though, the state of the EAC remains instable, and its re-stenosis and re-atresia may occur.
Declarations
Author contribution: DKL conceived, designed, and supervised the study. LZ and HYS conceived and designed the study. LZ and HYS drafted the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments: This work was supported by National Nature Science Foundation of China #81600801 (H.Y.S.).
References
- Kwiek B, Schwartz RA. Keratoacanthoma (KA): An update and review. J Am Acad Dermatol. 2016; 74: 1220-1233.
- Mascitti H, De Masson A, Brunet-Possenti F, Bouaziz JD, Laly P, Mourad N et al. Successful Treatment of Generalized Eruptive Keratoacanthoma of Grzybowski with Acitretin. Dermatol Ther. (Heidelb) 2019; 9: 383-388.
- Moriyama M, Watanabe T, Sakamoto N, Suzuki M, Mogi G, et al. A case of giant keratoacanthoma of the auricle. Auris Nasus Larynx. 2000; 27: 185-188.
- Grinspan Bozza NO, Totaro, II, Pocovi M, Reizner A, Sanchez G. [Keratoacanthoma centrifugum of Miedzinski and Kozakiewicz]. Med Cutan Ibero Lat Am. 1989; 17: 234-238.
- Tirelli G, Nicastro L, Gatto A, Boscolo Nata F. Stretching stenoses of the external auditory canal: A report of four cases and brief review of the literature. Acta Otorhinolaryngol Ital. 2015; 35: 34- 38.
- Kmeid M, Nehme J. Post-inflammatory acquired atresia of the external auditory canal. J Otol 2019; 14: 149-154.
- Adkins WY, Osguthorpe JD. Management of canal stenosis with a transposition flap. Laryngoscope. 1981; 91: 1267-1269.
- McDonald TJ, Facer GW, Clark JL. Surgical treatment of stenosis of the external auditory canal. Laryngoscope. 1986; 96: 830-833.
- Grundfast KM, Camilon F. External auditory canal stenosis and partial atresia without associated anomalies. Ann Otol Rhinol Laryngol. 1986; 95: 505-509.
- Bell DR. External auditory canal stenosis and atresia: dual flap surgery. J Otolaryngol. 1988; 17: 19-21
- McCary WS, Kryzer TC, Lambert PR. Application of split-thickness skin grafts for acquired diseases of the external auditory canal. Am J Otol. 1995; 16: 801-805.
- Jacobsen N, Mills R. Management of stenosis and acquired atresia of the external auditory meatus. J Laryngol Otol. 2006; 120: 266-271.
- Adhershitha AR, Anilkumar S, Rajesh C, Mohan DC. Prosthetic management of posttraumatic external auditory canal atresia: A rare cause of conductive hearing loss. J Indian Prosthodont Soc. 2016; 16: 390-394.
- Jotdar A, Dutta M, Kundu S, Mukhopadhyay S. Advancing Cholesteatoma Secondary to Acquired Atresia of the External Auditory Canal: Clinical Perspectives. J Clin Diagn Res. 2017; 11: MD01-MD03.