
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Gluteal-sacrospinous-vaginal fistula as a complication of sacrospinous ligament fixation after a vault prolapse: A case report
Montserrat Mestre Costa1*; Anna Moreno Baró2; Josep Pubill Soler1; Judith Lleberia Juanos1; Natalia Hebrero Torres2; Yolanda Canet Estévez2
1 Pelvic Floor Unit, Department of Obstetrics and Gynecology, Parc Taulí Hospital Universitari, Institut d’Investigació i Innovació Parc Taulí, I3PT, Universitat Autònoma de Barcelona, Sabadell, Barcelona, Spain.
2 Department of Obstetrics and Gynecology, Parc Taulí Hospital Universitari, Institut d’Investigació i Innovació Parc Taulí, I3PT, Universitat Autònoma de Barcelona, Sabadell, Barcelona, Spain.
*Corresponding Author: Montserrat Mestre
Pelvic Floor Unit, Department of Obstetrics and
Gynecology, Parc Taulí Hospital Universitari, Institut
d’Investigació i Innovació Parc Taulí, I3PT, Universitat
Autònoma de Barcelona, Sabadell, Barcelona, Spain.
Email: mmestre@tauli.cat
Received : Oct 18, 2021
Accepted : Dec 06, 2021
Published : Dec 13, 2021
Archived : www.jcimcr.org
Copyright : © Mestre M (2021).
Abstract
Background: Vault prolapse has a negative impact on women’s quality life as a result of associated ano-rectal, urinary and coital dysfunctions. One of the most common surgical procedures for the treatment of vault prolapse is sacrospinous ligament fixation. In this report we present an uncommon case of a gluteal-sacrospinous-vaginal fistula complication after this procedure.
Case presentation: A 63-year-old woman with a history of multiple procedures to repair vault prolapse and cystocele was referred to our institution with a nodule 5 X 4 cm in the left buttock. Magnetic Resonance Imaging and endoanal ultrasound confirmed an extrasphincteric gluteal-sacrospinous-vaginal fistula with purulent drainage in her vagina.
A multidisciplinary approach was performed with Urogynecology, traumatology and colorectal surgeon. A fistulectomy was executed successfully. Posterior controls revealed an asymptomatic patient.
Conclusions: This case report revealed an uncommon complication of sacrospinous fixation and the importance of a multidisciplinary approach and treatment with notable results.
Keywords: complication; sacrospinous fixation; fistula; pelvic organ prolapsed; abscess; gynaecology; mesh.
Abbreviations: POP: Pelvic Organ Prolapse; MRI: Magnetic Resonance Imaging; cm: centimetre.
Citation: Costa MM, Baro AM, Soler JP, Juanos JL, Torres NH, et al. Gluteal-sacrospinous-vaginal fistula as a complication of sacrospinous ligament fixation after a vault prolapse: A case report. J Clin Images Med Case Rep. 2021; 2(6): 1471.
Introduction
Vaginal vault prolapse happens when the top of the vagina (the vault) slips from its normal position and sags down and it sometimes happens after a hysterectomy [1]. Prolapse does have a negative impact on these women’s quality of life due to associated urinary, ano-rectal, as well as coital dysfunction [2].
One of the most common surgical procedures for the treatment of vault prolapse is sacrospinous ligament fixation [2], also referred to as sacrospinous ligament suspension. Utero-sacral ligaments originate over the region of the greater sciatic foramen and lateral sacrum and insert into the side of the cervix as well as the upper one-third of the vagina [2]. The ligament can be identified on pelvic examination by palpating the ischia spine and tracing posteriorly and medially to the sacrum. Marking sutures are placed on the vaginal epithelium at the site where it will attach to the sacrospinous ligament [3].
Known complications of this technique are: buttock pain and recurrent cystocele but there are also rare complications [4]. Long term complications, as anterior vaginal wall defects are reported in less than 20% of the cases [5].
In this report we present an uncommon case of a glutealsacrospinous-vaginal fistula complication after sacrospinous ligament fixation surgery to correct vault prolapse.
Case presentation
A 63-year-old woman with a history of multiple surgeries: An abdominal hysterectomy for myomatous uterus in 2003; an anterior colporrhaphy with a transobturator vaginal tape and a unilateral Richter (by placing polypropylene suture into the sacrospinous ligament using Miya Hook) for a cystocele, vault prolapse and stress incontinence, and an anterior and posterior Vypro II mesh (a large-pore-sized multifilamentous polypropylene) in 2004; a contralateral Richter for recurrent cystocele, vault prolapse and a rectocele in 2005; and an anterior Prolift (monofilament polypropylene mesh) mesh for recurrent cystocele in 2007, presented with a nodule measuring 5 X 4 centimetres in the left buttock compatible with an abscess in 2017 (Figure 1).

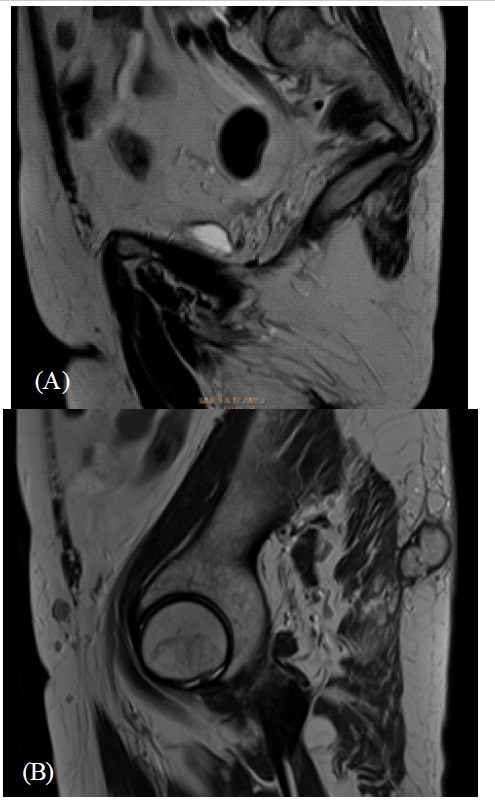
At the same time, the patient presented with purulent drainage in her vagina. Oral Antibiotic treatment was given to the patient and the patient improved. After several similar episodes a pelvic MRI was performed. The MRI showed an extrasphincteric fistula arising from the inferior rectum at 1 o'clock (left anterolateral) with an ascendent path crossing the left major incisura ischiatica and ending in a cul de sac at the sacrum ischiatic major level (Figure 2).
An endoanal ultrasound was performed and no internal or external fistula appeared.
A fistulectomy was performed with collaboration of urogynecologists, colorectal surgeon and traumatologist.
Firstly, the reproduction of vaginal dissection for sacrospinous fixation failed to allow for visualization of the offending sutures, meshes, fistula or purulent drainage.
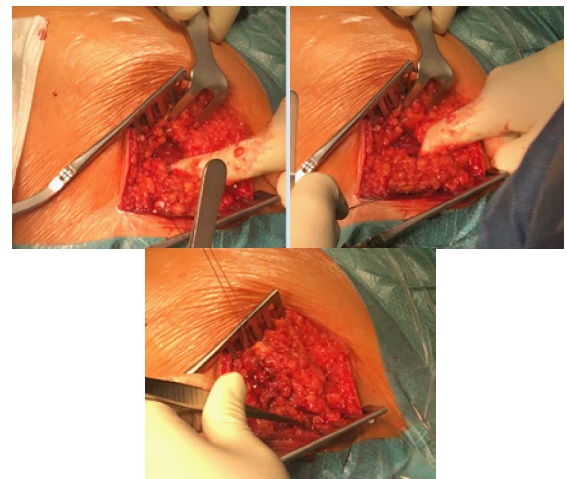
After that, a curvilinear incision on the left sacroiliac joint with the patient in left lateral decubitus was performed, following a dissection and it was identified a subcutaneous pocket as a reaction to odd body. Subsequently, a dissection through the gluteal fascia and excision of the subcutaneous pocket was performed. Presence of fistula emanating from permanent polypropylene through major incisura ischiatica was identified. After the placement of drainage, a communication with the vaginal ceiling was identified (Figure 3,4). The last step was closing by planes and closure of vagina.

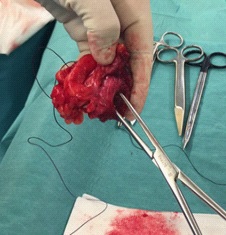
Afterward, the pathology results showed findings were compatible with a fistulous tract (Figure 5). In the culture of the fistula´s cavity grew Streptococcus constellatus.
At the last follow up visit, the fistula was healed and the patient presented a mild asymptomatic prolapse.
Discussion
Pelvic Floor Prolapse (POP) is due to the weakness of supporting tissues of pelvis, and associated with risk factor like age, parity, postmenopausal estrogenic deprivation, obesity, instrumental vaginal delivery, congenital defects, race, smoking, cronical disease that increase intrabdominal pressure (chronic constipation, pulmonary disease) or surgical removal of the uterus [6].
Recurrence rates after surgical correction of pelvic organ prolapse are not clear, but it’s estimated to 2 and 3.6 for 1000 women/year [7]. Risk of vaginal vault prolapse is 11-19% throughout women’s life post hysterectomy surgery.
Vaginal vault prolapse is the descent of the vaginal cuff below a point that is 2 cm less than the total vaginal length above the plane of the hymen [8].
It has a negative impact on women’s quality life as a result of associated ano-rectal, urinary and coital dysfuntions [2]. Main known symptoms are: Vaginal Bleeding, pressure in the pelvis, urinary incontinence, constipation.
The correction of vaginal vault prolapse, with the aim of restoring normal vaginal support should primarily be determined by the patient's symptoms and should be fully discussed with the woman before the procedure.
A variety of procedures exist for surgical treatment, one of most common and used procedures is Sacrospinous fixation. Described for the first time by Richter in 1968, who modified the Amreich procedure in 1951.
Several systematic reviews have shown that sacrospinous fixation is an effective therapy for vault prolapse with low recurrence and complication rates [9].
Haemorrhage is the most common complication during the procedure, because of the damage of the pudenda artery or hypogastric venous plexus. Other postoperative complications described are: Gluteal pain, vault haematoma, anterior wall defect, urinary tract infection, sensory loss [10]. The use of non-absorbable sutures (polypropylene) contributes better long-term results and anatomical support. The suture could act as a foreign body and lead to the formation of a fistula [11,12].
The treatment options consist of fistulotomy or fistulectomy. [5].
Conclusion
Gluteal-sacrospinous-vaginal fistula is an uncommon complication after sacrospinous fixation.
Few cases are described in the literature. Optimal treatment for a fistula involves reducing the risk of recurrence and increasing the quality of life.
As is shown in our case, pelvic MRI is important in the diagnosis also an endoanal ultrasound in order to detect those which could present an anorectal involvement.
This previous evaluation is important to offer an accurate diagnosis, an appropriate treatment and a multidisciplinary approach.
Declarations
Acknowledgements: We thank Alejandro Carballo M.D for his collaboration on the surgery.
Author’s contributions: MMC writing, editing of manuscript and figure preparation. AMB writing and figure preparation. NHT writing, editing of manuscript. All authors read and approved the final manuscript.
Funding: No sources of funding to declare.
Availability of data and materials: Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study
Ethics approval and consent to participate: Parc Taulí Commission noted that this report does not require consent to participate.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the consent is available for review by the Editor-in-Chief of this journal.
Conflicts of interest: The authors declare that they have no competing interests
This work has been presented at a prior meeting congress in 11th Annual Meeting EUGA in Milan 25-27 October 2018.
References
- Royal College of Obstetricians and Gynaecologists (RCOG), The British Society of Urogynaecology (BSUG) Joint Guideline. PostHysterectomy Vaginal Vault prolapse. Green-top Guideline No. 46. July 2015.
- Uzoma A, Farag K.A. Vaginal vault prolapse. Obstet Gynecol Int. 2009; 2009: 275621.
- Karram MM, Walters MD. Surgical treatment of vaginal vault prolapse and enterocele. Urogynecology and Reconstructive Pelvic Surgery, 3rd ed, Mosby Elsevier, Philadelphia. 2007: 267.
- Hibner M, Cornella JL, Magrina JF, Heppell JP. Ischiorectal abscess after sacrospinous ligament suspension. Am J Obstet Gynecol. 2005; 193: 1740-1742.
- Kadam PD. Rectocutaneous fistula with transmigration of the suture: A rare delayed complication of vault fixation with the sacrospinous ligament. Int Urogynecol J. 2016; 27: 155-157.
- Monk B.J, Ramp J.L, Montz F.J, Lebherz T.B. Sacrospinous Ligament Fixation for vaginal Vault prolapsed Complications and Results. Journal of Gybecologic Surgery. 7: 87-92.
- Martínez Franco E, Amat Tardiu L, Rodríguez Mias N, Cortés Laguna L, Laïlla Vicens JM. Tratamiento quirúrgico del prolapso de órganos pélvicos mediante Malla Prolift en pacientes con riesgo de recidiva. Arch Esp Urol. 2012; 65: 616-622.
- Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology. 2003; 61: 37-49.
- Cvach K, Dwyer P. Surgical management of pelvic organ prolapse: abdominal and vaginal approaches. World J Urol. 2012; 30: 471-477.
- Hefni MA, El-Toukhy TA. Long-term outcome of vaginal sacrospinous colpopexy for marked uterovaginal and vault prolapse. Eur J Obstet Gynecol Reprod Biol. 2006; 127: 257-263.
- Karram MM, Walters MD. Surgical treatment of vaginal vault prolapse and enterocele. In: Urogynecology and Reconstructive Pelvic Surgery, 3rd ed, Walters MD, Karram MM (Eds), Mosby Elsevier, Philadelphia. 2007. p.267.
- Salimans S, Speksnijder L, Vos L, Shekary-Moonen M, van Bavel J. Gluteal abscess and fistula after release of sacrospinous fixation sutures. Int J Gynaecol Obstet. 2017; 138: 127-128.
- Gafni-Kane A, Goldberg RP, Spitz JS, Sand PK. Extrasphincteric perianal fistulae after sacrospinous fixation for apical prolapse. Obstet Gynecol. 2011; 117: 438-440.