
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Autopolypectomy
LPL Gilissen1*; GMC Adriaans1; CJR Huysentruyt2
1 Department of Gastroenterology and Hepatology, Catharina Hospital Eindhoven, the Netherlands
2 Department of Pathology, Laboratory for Pathology and Medical Microbiology (PAMM), Eindhoven, the Netherlands.
*Corresponding Author: Lennard PL Gilissen
Gastroenterologist and Hepatologist, Department of
Gastroenterology and Hepatology, Catharina Hospital
Eindhoven, Michelangelolaan 2 5623 EJ Eindhoven,
the Netherlands.
Email: lennard.gilissen@catharinaziekenhuis.nl
Received : Nov 08, 2021
Accepted : Dec 10, 2021
Published : Dec 17, 2021
Archived : www.jcimcr.org
Copyright : © Dominguez MS (2021).
Citation: Gilissen LPL, Adriaans GMC, Huysentruyt CJR. Autopolypectomy. J Clin Images Med Case Rep. 2021; 2(6): 1490.
Report
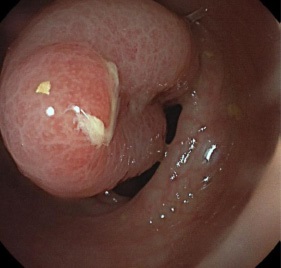
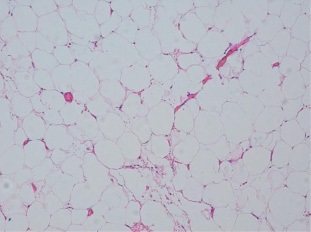
A 50-year-old man with a negative medical history except obesity visited the Emergency Unit because of acute anal blood loss, lower abdominal pain, constipation and a collapse. He mentioned the anal expulsion of a ‘meat chunck’ prior to the bleeding episode. He carried a glass jar with the collected specimen, which measured 5 X 4 X 2 cm and had a pink-yellowish colour (Figure 1). On physical examination he was hemodynamically stable (blood pressure 150/95 mmHg, heart rate 85 beats per minute), with no signs of anaemia neither abdominal tenderness. Rectal toucher showed dark, old blood. He was admitted and treated with intravenous tranexamic acid while being prepared for colonoscopy. His hemoglobin levels decreased from 9.1 to 8.1 mmol/l (8.5-11.0) in the first eight hours after admission, with mild leukocytosis (12.1/nL). Colonoscopy showed an ulcerated residual stalk of approximately two centimeters in the sigmoid colon (Figure 3). Histopathological examination of the specimen collected by the patient showed only benign adipocytes, in accordance with a giant lipoma (Figure 2).

The patient recovered quickly, but presented two months later again with a sigmoid perforation, surgically treated with an open sigmoid resection. Histopathology of the resected specimen showed a perforated benign ulcer. We concluded this should have been related with the previous autopolypectomy, because no diverticulosis was seen during colonoscopy, neither in the resected segment. No complications of surgery occurred.
This case demonstrates an autopolypectomy of a giant lipoma in the left-sided colon, presumably due to torsio and necrosis of the stalk. Lipomas are benign, submucosally located lesions, which may be found in any part of the gastrointestinal tract, with an incidence of 4.4% in the colon [1]. Only 6% of individuals with a lipoma have been estimated having any symptoms [2,3].
This case demonstrates an autopolypectomy of a giant lipoma in the left-sided colon, presumably due to torsio and necrosis of the stalk. Lipomas are benign, submucosally located lesions, which may be found in any part of the gastrointestinal tract, with an incidence of 4.4% in the colon [1]. Only 6% of individuals with a lipoma have been estimated having any symptoms [2,3]. In case of a diameter larger than 2 centimeters symptoms occur in 21% of patients: colic pain in the abdomen (51%), blood loss (46%), changes bowel habits (29%), sub)obstruction and/or invagination (25%), and perforation [4]. Lipomas rarely deteriorate to malignancy.
Endoscopically three signs may be present in case of a lipoma: 1) the pillow sign: by pushing the lesion with a closed biopsy forceps this can be impressed like a pillow; 2) the tenting sign: by grasping the overlying mucosa a fold may be easily pulled away, and 3) naked fat sign: fatty tissue appears when a biopsy is taken from the lesion [5]. The need for and type of therapy of a lipoma depends on the size, complications and possibility of malignancy in the lesion. Asymptomatic lipomas less than 2 cm should not be treated. In case of lesions of 2-4 cm that cause symptoms an endoscopic resection is appropriate, although resection with a hot wire is not advised, because adipocytes may accumulate the energy leading to increased chance of perforation. Probably the easiest and safest way of removing a large lipoma is by endoscopic insertion of an adjustable plastic loop around the stalk. This loop will strangulate the stalk leading to thrombosis of the vessels and necrosis of the lesion that will fall off in the end. No histological examination is possible then, but this is in fact not necessary. Lipomas larger than 4 cm should be considered for surgical resection [6]. In our patient the process of necrosis of the stalk occurred automatically, without any medical intervention, possibly due to torsio of the stalk No case reports on autopolypectomy of a giant lipoma have been described in literature.
Diagnosis: Spontanous anal loss of a giant, benign lipoma due to autopolypectomy.
References
- Jiang L, Jiang LS, Li FY, Ye H, Li N, Cheng NS, et al. Giant submucosal lipoma located in the descending colon: A case report and review of the literature. World J Gastroenterol. 2007; 13: 5664- 5667.
- Ghidirim J, Mishin I, Gutsu E, Gagauz I, Danch A, Russu S, et al. Giant submucosal lipoma of the cecum: Report of a case and review of literature. Rom J Gastroentero. 2005; 14: 393-396.
- Ho Huu An, Trieu Trieu Duong, Nguyen Van Truong, Le Van Quoc et al. A large lipoma of the descending colon: A rare case report. Radiology Case Reports. 2021; 16: 3396-3399.
- Crocetti D, Sapienza P, Sterpetti AV, Paliotta A, Gori ADE, Pedullà G, et al. Surgery for symptomatic colon lipoma: A systematic review of the literature. Anticancer Res. 2014; 34: 6271- 6276.
- Cartelle AL, Uy PP, and Ya JEL. Giant Colonic Lipoma Presenting as Intermittent Colonic Obstruction With Hematochezia. Cureus. 2020; 12: e11434.
- Farfour AN, AbuOmar NA, Alsohaibani FI. Large lipoma of the ascending colon: A case report and review of literature. J Surg Case Rep. 2020; 9: 1-3.