
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Contralateral lumbar plexopathy after minimally invasive transforaminal lumbar interbody fusion: A case report
Ki Dong Baek*; In Suk Bae*; Hee In Kang; Jae Hoon Kim; Cheolsu Jwa
Department of Neurosurgery, Nowon Eulji Medical Center, Eulji University, Seoul, Korea.
*Corresponding Author: In Suk Bae
Department of Neurosurgery, Nowon Eulji Medical
Center, Eulji University, 68, Hangeulbiseok-ro, Nowongu, Seoul 01830, Korea.
Email: tbgitw@eulji.ac.kr
Received : Oct 25, 2021
Accepted : Dec 13, 2021
Published : Dec 20, 2021
Archived : www.jcimcr.org
Copyright : © Bae IS (2021).
Abstract
Introduction: Minimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF) is an effective treatment for patients with degenerative lumbar spinal disease. This modality was devised to reduce approach-related morbidity and complications of open TLIF.
Materials and methods: In this report, we describe a unique case of a 40-year-old woman who developed contralateral lumbar plexopathy one day after the MI-TLIF procedure.
Results: Postoperative Computed Tomography (CT) and MRI showed a left L4 transverse process fracture compressing the psoas muscle, and the lumbosacral fascia and erector spinae muscles were displaced forward. We performed fractured left L4 transverse process bone fragment removal to decompress the psoas muscle and correct the original place of the left lumbar fascia and erector spinae muscles. One month after reoperation, the patient had gradual alleviation of pain; leg weakness also recovered enough to enable locomotion.
Conclusions: In our case, MI-TLIF relieved lower back and right leg pain. However, the patient developed left radicular leg pain with weakness. There was displacement of the lumbosacral fascia and erector spinae muscles. These problems induced displacement of the psoas muscle with compression, which resulted in lumbar plexopathy. If skin incisions are not enough to carry further down through the subcutaneous tissue and the underlying fascia, displacement of both the left lumbosacral fascia and erector muscles can occur while inserting the pedicle screws. Therefore, it is important to make an incision from the skin to the underlying fascia and surgical corridors to insert the pedicle screws during MI-TLIF.
Keywords: transforaminal lumbar interbody fusion; plexopathy; pedicle screw.
Citation: Baek KD, Bae IS, Kang HI, Kim JH, Jwa C. Contralateral lumbar plexopathy after minimally invasive transforaminal lumbar interbody fusion: A case report. J Clin Images Med Case Rep. 2021; 2(6): 1491.
Introduction
Degenerative lumbar spine disease is one of the most prevalent healthcare problems in the world, with chronic lower backpain and radicular symptoms in the lower extremities [1]. Minimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF) is an effective treatment for patients with degenerative lumbar spinal disease. This modality was devised to reduce the approach related morbidity and complications of open TLIF [2]. In addition, MI-TLIF leads to lesser intraoperative blood loss and shorter hospital stay compared to open TLIF and has been widely implemented recently [3].
TLIF is an effective treatment for patients with degenerative spondylolisthesis and degenerative disc disease [4]. High success rates and few complications have been reported. Postoperative radiculopathy has been reported as a common complication of TLIF. However, there are very few cases of lumbar plexopathy following TLIF. Although lumbar plexopathy has been reported following gynecological procedures and transpsoas interbody fusion, there were no reports of this complication following instrumented MI-TLIF [5].
In this report, we describe a unique case of a 40 year old woman who developed contralateral lumbar plexopathy one d after the MI TLIF procedure.
Case presentation
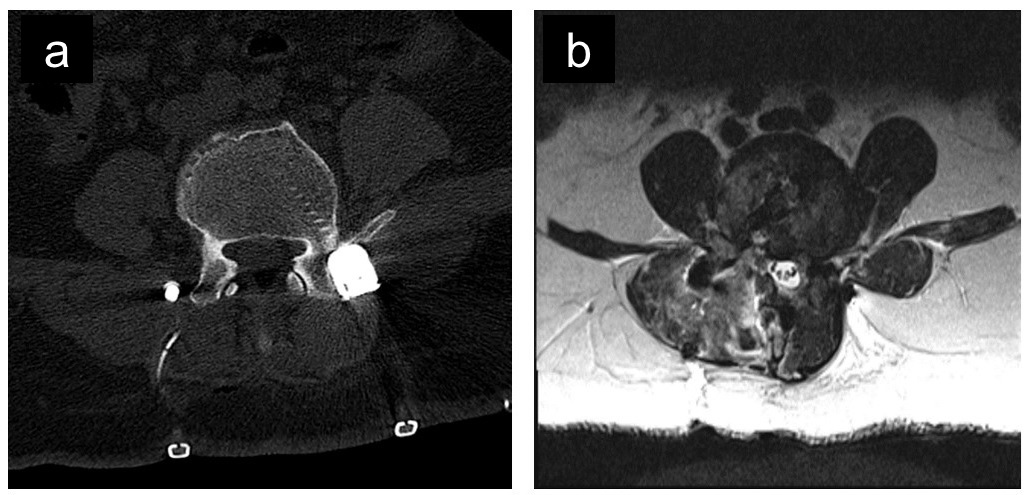
A 40 year old woman presented to our institution with lower back pain and radiating right leg pain. Her symptoms had begun one year previously. Lumbar radiographs and Magnetic Resonance Imaging (MRI) showed for aminal stenosis and spinal segmental instability at the L4-5 level. After failure of conservative treatment, the patient underwent MI-TLIF at L4-5 pathology via a right paramedian incision. Postoperatively, while still in the hospital, the patient reported no right leg pain. However, she complained of left leg pain in the L2,3 nerve distribution one day after MI-TLIF. In addition, hip flexion motor grade was reported as motor grade II, and knee extension motor grade was reported as grade III. Postoperative lumbar radiographs showed no obvious malposition of the instruments. Postoperative Computed Tomography (CT) and MRI showed a left L4 transverse process fracture compressing the psoas muscle, and the lumbosacral fascia and erector spinae muscles were displaced forward (Figure 1A,B). However, no lesions in the spine that could explain left leg weakness were observed on postoperative MRI. We performed fractured left L4 transverse process bone fragment removal to decompress the psoas muscle and correct the original place of the left lumbar fascia and erector spinae muscles. After three weeks of operation, Electromyogram (EMG) and Nerve Conduction Study (NCS) were performed. In NCS, there were decreased sensory amplitudes at the left lateral cutaneous nerve of the L2-3 division of the lumbar plexus and the left saphenous nerve. In addition, motor conduction velocities at both the left femoral nerve and the peroneal portion of the left sciatic nerve were decreased. EMG showed increased insertional activities and positive sharp waves at the left tibialis anterior and left adductor longus.
After reoperation, she was administered symptomatic treatments; analgesics, including opioids and gabapentin, were prescribed for neuropathic pain relief. In addition, rehabilitation was regularly performed for leg weakness. One month after reoperation, the patient had gradual alleviation of pain; leg weakness also recovered enough to enable locomotion.
Discussion
The lumbar plexus is situated within the posterior aspect of the psoas muscle in front of the transverse process of the lumbar vertebrae. It is formed by the anterior division of the first three (L1-3) and a greater part of the fourth lumbar nerve (L4), with a contribution from the last thoracic nerve [5]. It courses posterior to, or mingles with, the fascicles of the psoas muscle before convergence of the lumbar anterior primary rami to form the lumbar plexus; branches are distributed to the psoas muscle and the quadratus lumborum [6].
Lumbar plexopathy is an injury to the nerves of the lumbar plexus. Although this condition is not uncommon,diagnosis and management tend to be difficult [7]. Patients with lumbar plexopathy usually present with lower back and/or leg pain. They can also experience motor weakness, as well as other sensory symptoms such as numbness, paresthesia, and/or sphincter dysfunction [8]. Lumbar plexopathy predominantly causes motor symptoms; however, it also affects the autonomic and sensory components of the plexus [9].
The clinical presentation of a patient depends on which part of the plexus is affected. Historically, the lumbosacral plexus was divided into the upper lumbar plexus (T12-L2), lower lumbar plexus (L2-4), and sacral plexus (L4-S4) [10]. Our patient’s clinical features supported lumbar plexopathy. Moreover, this condition has been reported to occur following instrumented lumbar spinal procedures, such as posterior or transforaminal lumbar interbody fusion [11]. Some authors attributed lumbosacral plexopathy to direct lumbar plexus trauma during instrumentation and lateral paraspinal muscle dissection, occurring just anterior to the transverse processes of the lumbar vertebrae [5]. There are several elements of this case that warrant discussion: the pathophysiologic mechanism in our patient and the evidence base for managing this condition [10].
In our case, the patient underwent MI-TLIF for severe lower back pain and right radicular leg pain. She experienced new symptoms one day after the procedure; contralateral left radicular leg pain and left motor leg weakness, especially left hip flexion motor grade reduced to grade II and knee extension motor grade reduced to grade III. Generally, inadequate pressure support during prone procedures has been advocated as an alternative cause of postoperative neural palsies; the inguinal ligament is a key risk factor. However, branches of the lumbar plexus to the psoas and iliacus are proximal to the inguinal ligament. Hence, any neural compression at the level of the inguinal ligament would not cause hip flexor weakness [5]. Her symptoms suggested that the lumbar plexus was involved. On postoperative imaging, new findings have been confirmed: 1) left L4 transverse process fracture, 2) displacement of the lumbar fascia and left erector spinae muscles, and 3) compression of the left psoas muscle.
Left L4 transverse process fracture occurred during the course of MI-TLIF: percutaneous pedicle screw insertion by small skin incision. However, we made small and shallow incisions of approximately 1 cm for minimal scarring in this patient. When inserting the percutaneous pedicle screw, displacement of the left lumbar fascia and left erector spinae muscles occurred because of small and insufficient deep incisions. This caused a strong pressure on the screw entry site, that is, the junction of the transverse process and the superior facet. The pressure induced a fracture of the left L4 transverse process, and fractured bone fragments induced severe psoas muscle compression. These problems indirectly caused strengthened damage to the lumbosacral plexus.
MI-TLIF leads to lesser intraoperative blood loss and shorter hospital stay than open TLIF. In addition, it can cause minimal scarring and is reported to have a lower complication rate compared to open TLIF [3]. During MI-TLIF, ipsilateral screws are inserted in a dorsoventral fashion with a vertical vector using a retractor. Moreover, contralateral pedicle screws are inserted in a percutaneous fashion through small stabincisions under fluoroscopic guidance [12]. When pedicle screws are inserted at the contralateral side, surgeons should focus on incisions to be carried further down through the subcutaneous tissue and the underlying fascia rather than minimal scarring. In addition, surgeons should try blunt dissection using a finger to create a surgical corridor for percutaneous screw insertion.
In this patient, we performed fractured left L4 transverse process bone fragment removal for decompressing the psoas muscle and correcting the original place of the left lumbar fascia and erector spinae muscles. After the procedure, the patient presented with mildly improved symptoms, which still remained due to a strengthened injury of the lumbar plexus. In painful forms, our patient received a neuropathic agent (pregabalin) and regular physiotherapy. In addition, we used a nonsteroidal anti-inflammatory drug in combination with opioids. In the acute stage of lumbar plexopathy, corticosteroid therapy is administered to the patient. Finally, our patient had gradual alleviation of pain, and the leg weakness recovered enough to be able to walk independently
Conclusion
In our case, MI-TLIF relieved lower back and right leg pain. However, the patient developed left radicular leg pain with weakness. There was displacement of the lumbosacral fascia and erector spinae muscles. Strong pressure occurred and caused fracture of the left L4 transverse process. These problems induced displacement of the psoas muscle with compression, which resulted in lumbar plexopathy. If skin incisions are not enough to carry further down through the subcutaneous tissue and the underlying fascia, displacement of both the left lumbosacral fascia and erector muscles can occur while inserting the pedicle screws. Therefore, it is important to make an incision from the skin to the underlying fascia and surgical corridors to insert the pedicle screws during MI-TLIF. In addition, surgeons should be mindful of the possibility of plexopathy after TLIF.
Compliance with ethical standards
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
- Gooch CL, Pracht E, Borenstein AR. The burden of neurological disease in the United States: A summary report and call to action. Ann Neurol. 2017; 81: 479–484.
- Deutsch H, Musacchio MJ. Minimally invasive transforaminal lumbar interbody fusion with unilateral pedicle screw fixation. FOC. 2006; 20: 1–5.
- Garg B, Mehta N. Minimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF): A review of indications, technique, results and complications. Journal of Clinical Orthopaedics and Trauma. 2019; 10: S156–S162.
- Potter BK, Freedman BA, Verwiebe EG, et al. Transforaminal lumbar interbody fusion: Clinical and radiographic results and complications in 100 consecutive patients. J Spinal Disord Tech. 2005; 18: 337–346.
- Sekharappa V, James I, Amritanand R, et al. Lumbar plexopathy following instrumented posterior lumbar interbody fusion: A complication with use of Hohmann’s retractor. Eur Spine J. 2013; 22: 2039–2046.
- Levin KH, Said G, Dyck PJB, et al. New Insights in Lumbosacral Plexopathy. 124
- Ng PS, Dyck PJ, Laughlin RS, et al. Lumbosacral radiculoplexus neuropathy: Incidence and the association with diabetes mellitus. Neurology. 2019; 92: e1188–e1194.
- Dydyk AM, Hameed S. Lumbosacral Plexopathy. In: Stat Pearls. Stat Pearls Publishing, Treasure Island (FL) 2021.
- Rubin DI. Brachial and lumbosacral plexopathies: A review. Clin Neurophysiol Pract. 2020; 5: 173–193.
- Tulloch I, Ali R, Papadopoulos MC. Contralateral lumbosacral plexopathy following lumbar microdiscectomy. British Journal of Neurosurgery. 2020; 34: 357–361.
- Davis TT, Bae HW, Mok JM, et al. Lumbar plexus anatomy within the psoas muscle: implications for the transpsoas lateral approach to the L4-L5 disc. J Bone Joint Surg Am. 2011; 93: 1482– 1487.
- Reinshagen C, Ruess D, Walcott BP, et al. A novel minimally invasive technique for lumbar decompression, realignment, and navigated interbody fusion. J Clin Neurosci. 2015; 22: 1484– 1490.