
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Umbilical cord hemangioma diagnosed at 31 weeks of amenorrhea: A rare case report
Saloua Tanouti*; Chaymae Chemlal; Hafsa Taheri; Hanane Saadi; Ahmed Mimouni
Gynecology and Obstetrics Department, Faculty of Medicine Oujda, Mohammed VI University Hospital, Mohammed First University Oujda, Morocco.
*Corresponding Author: Saloua Tanouti
Gynecology and Obstetrics Department in Mohammed
VI University Hospital Oujda, Morocco.
Email: Saloua.tanouti@gmail.com
Received : Oct 21, 2021
Accepted : Dec 13, 2021
Published : Dec 20, 2021
Archived : www.jcimcr.org
Copyright : © Tanouti S (2021).
Abstract
Umbilical cord hemangioma is a rare benign vascular tumor, not always detected prenatally, several fetal complications can occur such as fetal prematurity, intra uterine growth restriction, fetal malformations, intra uterine death. We describe a case of Umbilical cord hemangioma diagnosed at 31 weeks of amenorrhea complicated with an intra-uterine growth restriction and preterm delivery at 31 weeks of amenorrhea with good maternal and fetal outcome. We reviewed the literature data.
Keywords: umbilical cord hemangioma; benign; rare; fetal complications.
Citation: Tanouti S, Chemla C, Taheri H, Saadi H, Mimouni A. Umbilical cord hemangioma diagnosed at 31 weeks of amenorrhea: A rare case report. J Clin Images Med Case Rep. 2021; 2(6): 1494.
Introduction
Umbilical cord hemangioma is a benign vascular tumor rarely described, several complications of which can occur including fetal prematurity, fetal death in utero [1,2] and intrauterine growth retardation [3] a second localization, hydramnios, intrauterine hemorrhage as well as fetal malformations may be associated with this tumor [4,5]. We describe a case of umbilical cord hemangioma diagnosed at 31SA complicated with an IUGR and preterm delivery at 31 SA, we reviewed the data of literature.
Case report
We present the case of 28-year-old patient, gestation 1, para 0, the gestational age of the current pregnancy was estimated at 31 weeks of amenorrhea. without pathological history, the ultrasound of the first trimester was without peculiarity. The screening of trisomy 21 and alpha foeto-protein biochemical marker were not done. The patient consulted in the emergency room for uterine contractions at 31 weeks of amenorrhea. Obstetric examination objectified a parturient at the beginning of labor. Pelvic ultrasound objectified a fetus in presentation of breech, fetal biometrics lower than the 3rd percentile with an estimate fetal weight of 1300 g. We discovered a voluminous mass of the free segment of the umbilical cord near its placental insertion. In axial section of the cord, we visualized cystic images anechogenic non-vascularized with a hyperechogenic component measuring 109 X 100 mm.
The mass was clearly distinguished from the surrounding tissues (wharton’s jelly) which appeared enlarged and edematous (Figure 1).

The biological assessments were without peculiarity. The recording of the fetal heart rate was normal.
She spontaneously has progressed to the second stage of labor hence the decision of a delivery by cesarean out of fear of mechanical dystocia during a vaginal delivery if the tumor were engaged at the same time as the abdomen, given the large size of the tumor as well as the presentation breech which was an added factor for our decision.
The male newborn weighed 1292 g, the Apgar score was 9 to 5 minutes of life with harmonious growth restriction. He was admitted in neonatology unit for further management. The physical examination showed no birthmarks, and an ultrasound examination that was performed the second day postpartum to exclude any haemangiomas in the baby’s liver was normal. The infant is currently healthy with 5 months of hindsight.
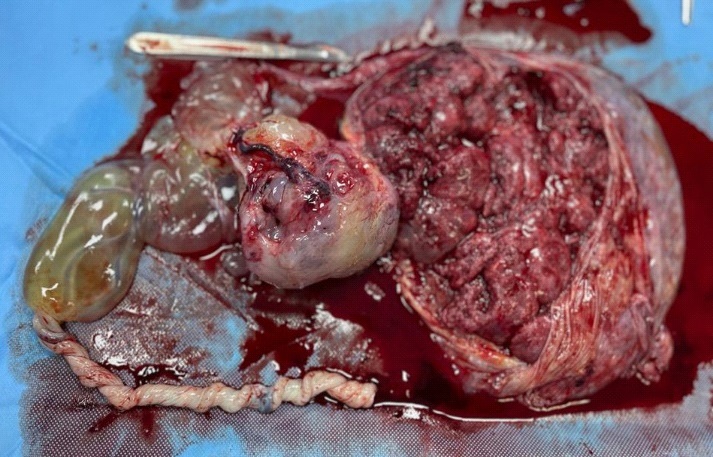
The grossing of the placenta identified a 10 X 10 X 6 cm mass on the umbilical cord near the placental insertion of the cord which measured 39 cm (Figure 2), the cord was gelatinous and edemated near the tumor. On cut section, the mass was heterogenous showing foci of hemorrhage and cystic degeneration.
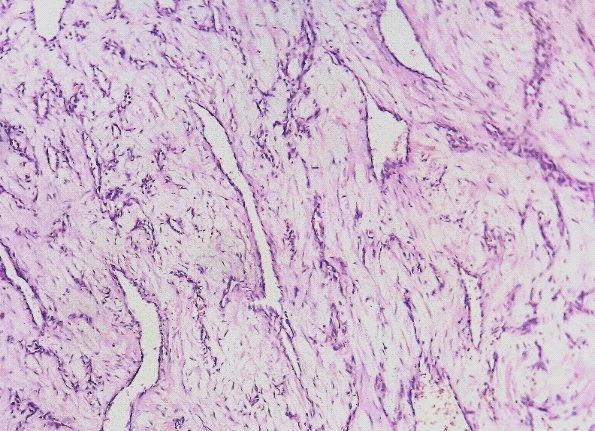
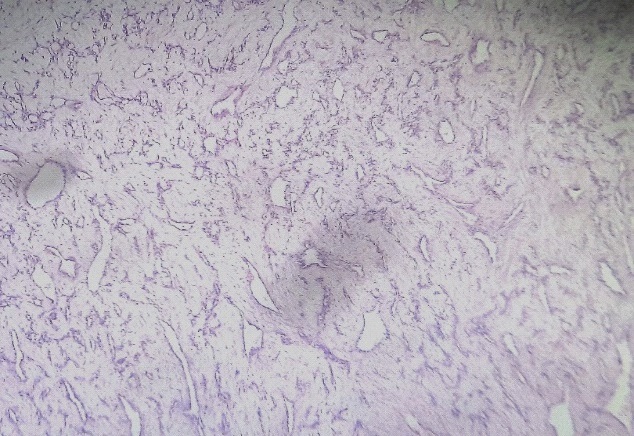
Microscopic examination of samples taken from the mass has shown a benign vascular proliferation made of small vascular channel. Endothelial cells showed no atypia or mitotic activity. The surrounding stroma was myxoid with presence of rare inflammatory cells. Some calcifications were observed in the lumen of umbilical vessels. Chorangiosis lesions was also observed. These observations are consistent with a capillary hemangioma of the umbilical cord (Figures 3,4).
Discussion
Cord hemangioma is a rare tumor, only 40 cases have been described in the literature including our case, which are summarized in the table below (Table 1).
Table 1:Review of the literature of cases of hemangioma of the cord.
Reference |
Case number |
Size(cm) |
Diagnosis |
Localisation |
Alpha-fœtoprote´ine |
Diagnosis term |
Delivery |
Associated anomalies |
Barryandal.1951 |
1 |
12 |
Postnatal |
Placental |
– |
P |
– |
Neonatal death/ liver angioma |
|
|
|
|
|
|
|
|
|
Benirschke1967 |
1 |
7 |
Postnatal |
Placental |
– |
P |
vaginal delivery40AW |
1Atrophic UO |
Carvounis1978 |
1 |
6 |
Postnatal |
Placental |
– |
P |
vaginal delivery |
– |
Fortune1980 |
1 |
10 |
Postnatal |
Placental |
– |
P |
IUFD at |
– |
Barson1980 |
1 |
1.5 |
Postnatal |
Placental |
H |
P |
30AW |
– |
|
|
|
|
|
|
|
|
|
Heifetz1983 |
4 |
9.5/0.5/0.2/NA |
Postnatal |
Placental(1case) |
– |
P |
2 IUFD |
IUFD+PE |
|
|
|
|
|
|
|
|
|
Seifer and al.1985 |
1 |
_ |
prenatal |
Fetal |
– |
30AW |
Urgent CS31AWfor AFHR |
IUFD+abruption |
|
|
|
|
|
|
|
|
|
Dombrowski1987 |
1 |
NA |
Postnatal |
Fetal |
– |
P |
Metrorrhagia and AFHR |
Cord rupture,DIC,ileal atresia, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mishriki1987 |
1 |
13 |
prenatal |
Placental |
– |
30AW |
– |
RDS,NEC,Hydrocephalous |
Restaandal. 1988 |
1 |
3.2 |
prenatal |
Placental |
H |
17AW |
IUFD20AW |
IUFD–cordstenosis |
|
|
|
|
|
|
|
|
|
Yavner1989 |
1 |
5 |
prenatal |
Fetal |
H |
20AW |
38AW |
– |
Pollack1989 |
1 |
4.5 |
prenatal |
Placental |
H |
20AW |
vaginal delivery term |
– |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ghidini1990 |
1 |
3.7 |
prenatal |
Fetal |
– |
34AW |
vaginal delivery37AW |
Hypospadias |
Jauniaux1990 |
1 |
8 |
prenatal |
Placental |
H |
20AW |
scheduled CS 37AW |
Skin lesion,cord oedema |
Tekant1993 |
1 |
7 |
Postnatal |
Fetal |
– |
P |
vaginal deliveryterm |
– |
Weyerts etal.1993 |
1 |
4.8 |
prenatal |
Fetal |
N |
33AW |
scheduled CS37AW |
Anteriorwallhemangioma |
|
|
|
|
|
|
|
|
|
Armes1994 |
1 |
1.5 |
prenatal |
Placental |
– |
32AW |
Urgent CS34AW |
NND-Twins,limbdeformities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sondergaard1994 |
1 |
4 |
Postnatal |
Placental |
– |
P |
IUFD28AW |
– |
Carles1994 |
1 |
_ |
prenatal |
– |
– |
21AW |
Urgent CS 28AW |
Neonatal death,foetoplacentary anasarch |
|
|
|
|
|
|
|
|
|
Wilson1994 |
1 |
5 |
prenatal |
Fetal |
– |
17AW |
vaginal delivery36AW |
Oligoamnios |
Shipp1995 |
1 |
6 |
prenatal |
Placental |
– |
33AW |
36AW |
Oligoamnios |
Miller1997 |
1 |
2 |
Postnatal |
Fetal |
H |
15AW |
vaginal delivery38AW |
– |
|
|
|
|
|
|
|
|
|
Tennstedt 1998 |
1 |
8 |
prenatal |
Fetal |
N |
18AW gemellar pregnancy |
scheduled CS 36AW |
– |
Kamitomo1999 |
1 |
2.5 |
prenatal |
Placental |
H |
16AW |
IUFD17AW |
– |
Caldarella2003 |
1 |
13 |
prenatal |
Placental |
N |
32AW |
Urgent CS32AWfor |
Fetal anasarch |
|
|
|
|
|
|
|
end UD |
|
Daniel-Spiegelandal.2005 |
1 |
2.5 |
prenatal |
Placenta |
N |
27AW |
vaginal delivery38AW |
Multiple skin angiomas |
|
|
|
|
|
|
|
|
|
Vougiouklakis2006 |
1 |
|
Postnatal |
Fetal |
– |
P |
IUFD38AW |
Cordrupture |
|
|
|
|
|
|
|
|
|
Lyoob2006 |
1 |
8 |
prenatal |
Placental |
N |
31AW |
Urgent CS31AW severPE |
Hydramniosis,UUA |
Nataluci2007 |
1 |
4 |
prenatal |
Fetal |
H |
33AW |
vaginal delivery38AW |
– |
|
|
|
|
|
|
|
|
|
Malliahandal.2007 |
1 |
2 |
prenatal |
Placental |
– |
19AW |
Urgent CS 37AW |
Hydramnios,Skin angioma |
|
|
|
|
|
|
|
|
|
Papadopoulost andal.2009 |
1 |
4 |
prenatal |
Placental |
N |
22AW |
scheduled CS37AW |
– |
Sathiyathasan and al. 2011 |
1 |
2 |
prenatal |
– |
– |
22AW |
IUFD26AW |
– |
Matsudaandal.2011
Jacques and Qureshi 2013 Smulian2015 Hara and al. 2015
M. Berar and all2018 Our serie 2021 |
1
1 1 1
1 1
|
4
NA NA 5
10 10 |
Prenatal
Postnatal Prenatal Prenatal
Prenatal prenatal |
Fetal
Placental Fetal Placental
Placental placental |
–
_ _ H
H _ |
18AW
Postnatal 22 AW 26 AW
31 AW 31 AW |
vaginal delivery39AW
IUFD26AW Urgent CS 36SAforAFHR Urgent CS 29AW for heart failure |
–
Right lung: 2 lobes
– –
|
Abbreviations: NA: Not available; MTP: medical termination of pregnancy; IUFD:intra uterine fetal death; UD: umbilical diastole; AFHR: abnormal fetal heart rate; UUA: unique umbilical artery; IUGR: Intrauterine growth retardation; CS: cesarean section.
We note that the postnatal diagnosis was made in 15 cases, the majority of which were carried out before 1999 (10 cases) [1,6,5], while antenatal diagnosis has been made in most recent studies, this is explained by the change in the quality of the screening ultrasound
Usually the diagnosis of umbilical cord hemangioma is made In the 2nd and 3rd trimester except in one case where the diagnosis was made at 16 WA leading to an intra-uterine fetal death (IUD) at 17 WA [5]. The tumor is located almost twice more frequently towards the placental than the fetal end of the cord [5]. The differential diagnosis must include hematomas and teratomas of the umbilical cord, placental masses, and abdominal wall defects [7-9] near the placental insertion, the distinction with a placental chorioangioma can be problematic because these two tumors look similar to ultrasound [5]. The nodule size ranged from 0.2 to 13 cm in literature [10].
Hemangiomas have been associated with raised MS-AFP, congenital anomalies, hydramnios, preterm labor and increased perinatal mortality, especially intrauterine deaths (IUDs). One of the cases reported in 1987 by Dombrowski et al. was revealed by rupture of the cord causing intrauterine hemorrhage in the context of premature rupture of membranes in a patient with heroin addiction, whose pregnancy had not been followed [11,12]. A case has been mistaken for an omphalocele [13].
There is an increase in alpha-foeto-protein in the presence of this tumor in the literature, the mechanism of which has not been identified. There are several probabilities in the literature regarding the increase in AFP levels including rupture of the foeto-amniotic barrier similar to the omphaloceles and neural tube defects mechanism [14,15], with leakage of AFP from the fetus to the Amniotic Fluid (AF) via the hemangioma. This implies that at the level of the fine tumor vessels, there is the passage of fetal serum an additional flow to the amniotic fluid through the permeable amniotic membrane and a subsequent increase in maternal serum.
The findings of increased levels of AFP in the AF [15,16] as well as in the cystic lesion surrounding the tumor [15] support this speculation.
In the literature review (Table 1), this was the case in 10 cases [17,5,18]. There are 11 cases of childbirth between 28 and 36 weeks including our case (Table 1). Of these, only three were presented with the spontaneous onset of labor as is the case for our patient, however the establishment of a direct relationship between this tumor and preterm delivery is an unsupported fact [19,20,8].
In total, out of series of 41 cases, including our case, there were 12/41 (29%) children born alive without any associated anomaly [5]. Nine cases of IUDs [1,2,5,13] have been documented. We only notice a growth below the 3rd percentile in five cases, ours included. We noted five cases of associated hemangiomas (four cutaneous [11,21,4,5 ] and one of the anterior abdominal wall [22]) one case of hypospade [5], two cases of fetal hydrops [21,5], one case of only two lobes of right lung,one case of gastrointestinal malformation [5], one case of heart faillure[18], two cases of oligoamnios [5], and three cases of hydramnios [4,5].
In our case, a cesarean was performed for the rapid evolution of labor at 31 weeks and the large size of the mass; in the literature there are no precise indications for the delivery. The maximum size of umbilical cord hemangioma for which delivery was vaginal was 70 mm [5] and for cesareans, 130 mm [18].14 deliveries out of 28 were carried out by cesarean section, 9 of them were urgent CS for AFCR, fetal hydrops [11] severe preeclampsia [5]All scheduled cesarean sections were performed after 36–37 weeks.
Conclusion
In our case, a cesarean was performed for the rapid evolution of labor at 31 weeks and the large size of the mass; in the literature there are no precise indications for the delivery. The maximum size of umbilical cord hemangioma for which delivery was vaginal was 70 mm [5] and for cesareans, 130 mm [18].14 deliveries out of 28 were carried out by cesarean section, 9 of them were urgent CS for AFCR, fetal hydrops [11] severe preeclampsia [5]All scheduled cesarean sections were performed after 36–37 weeks.
References
- Fortune DW, Ostor A. Angiomyxomas of the umbilical cord. Obstet Gynecol 1980; 55: 375–8.
- Sondergaard G. Hemangioma of the umbilical cord. Acta Obstet Gynecol Scand. 1994; 73: 434–6.
- Smulian JC, Sarno AP, Rochon ML, Loven VA. The natural history of an umbilical cord hemangioma. J Clin Ultrasound. 2016; 44: 455–8.
- Malliah R, Shah V, Heller DS. Umbilical cord hemangioma associated with multiple cutaneous hemangiomas in a newborn. Int J Gynecol Obstet 2007; 99: 58.
- Papadopoulos VG, Kourea HP, Adonakis GL, Decavalas GO. A case of umbilical cord hemangioma: Doppler studies and review of the literature. Eur J Obstet Gynecol Reprod Biol 2009; 144: 8–14.
- Barry FE, McCoy CP, Callahan WP. Hemangioma of the umbilical cord. Am J Obstet Gynecol. 1951; 62: 675–80.
- Malliah R, Shah V, Heller DS. Umbilical cord hemangioma associated with multiple cutaneous hemangiomas in a newborn. Int J Gynecol Obstet 2007; 99: 58.
- Mishriki YY, Vanyshelbaum Y, Epstein H, Blanc W. Hemangioma of the umbilical cord. Pediatr Pathol. 1987; 7: 43–9.
- Caldarella A, Buccoliero AM, Taddei A, Savino L, Taddei GL. Hemangioma of the umbilical cord: Report of a case. Pathol Res Pract 2003; 199: 51–5.
- Heifetz SA, Rueda-Pedraza ME. Hemangiomas of the umbilical cord. Pediatr Pathol 1983; 1: 385–98.
- Daniel-Spiegel E, Weiner E, Gimburg G, Shalev E. The association of umbilical cord hemangioma with fetal vascular birthmarks. Prenat Diagn 2005; 25: 300–3.
- Sathiyathasan S, Jeyanthan K, Hamid R. Umbilical hemangioma: a case report. Arch Gynecol Obstet. 2011; 283: S15–7.
- Jacques SM, Qureshi F. Hemangioma of the umbilical cord with amnionic epithelial inclusion cyst. Fetal Pediatr Pathol. 2013; 32: 235–9.
- Resta RG, Luthy DA, Mahony BS. Umbilical cord hemangioma associated with extremely high alpha-fetoprotein levels. Obstet Gynecol. 1988; 72: 488–91.
- Pollack MS, Bound LM. Hemangioma of the umbilical cord. Sonographic appearance. J Ultrasound Med. 1989; 8: 163–6
- Barson AJ, Donnai P, Ferguson A, Donnai D, Read AP. Haemangioma of the cord: further cause of raised maternal serum and liquor alpha-fetoprotein. Br Med J. 1980; 281: 1252.
- Resta RG, Luthy DA, Mahony BS. Umbilical cord hemangioma associated with extremely high alpha-fetoprotein levels. Obstet Gynecol. 1988; 72: 488–91.
- Hara K, Fukumura Y, Saito T, Arakawa A, Okabe H, Takeda S, et al. A giant cord hemangioma with extramedullary hematopoiesis and elevated maternal se- rum human chorionic gonadotropin: a case report and review of the literature. Diagn Pathol. 2015; 10: 154.
- Barry FE, McCoy CP, Callahan WP. Hemangioma of the umbilical cord. Am J Obstet Gynecol. 1951; 62: 675–80.
- Dombrowski MP, Budev H, Wolfe HM, Sokol RJ, Perrin E. Fetal hemorrhage from umbilical cord hemangioma. Obstet Gynecol. 1987; 70: 439–42.
- Seifer DB, Ferguson IIJE, Behrens CM, Zemel S, Stevenson DK, Ross JC. Nonim- mune hydrops fetalis in association with hemangioma of the umbilical cord. Obstet Gynecol. 1985; 66: 283–6.
- Weyerts LK, Jones MC, Grafe M, Scioscia AL. Umbilical cord haemangioma associated with an eruptive cutaneous haemangioma in a female infant. Prenat Diagn. 1993; 13: 61–4.