
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Definitive guiding flange prosthesis for management of hemimandibulectomy: A case report
Jhalak Thakur*; Swapnil Parlani; Nimit Jain; Shreyans Damade; Kirti Jajoo; Pushkar Dwivedi
Department of Prosthodontics, People’s College of Dental Science and Research Centre, Bhopal, India.
*Corresponding Author: Jhalak Thakur
Department of Prosthodontics, People’s College of Dental Science and Research Centre, Bhopal, India.
Email: jhalakthakur1992@gmail.com
Received : Oct 30, 2021
Accepted : Dec 15, 2021
Published : Dec 22, 2021
Archived : www.jcimcr.org
Copyright : © Thakur J (2021).
Abstract
Management of segmental mandibulectomy defects present a major challenge to the rehabilitation team. Mandibular discontinuity obliterates the equilibrium and mandibular function’s symmetry, which leads to altered mandibular movements, facial disFigurement, incomprehensible swallowing, impaired speech and deviation of the remaining fragment towards the surgical side. While opening the mouth, this deviation intensifies, leading to the opening and closing in the angular pathway. A definitive mandibular guiding flange prosthesis on the resected side can be used productively to stabilize the occlusion and correct the deviation. A new prospective for treating segmental mandibulectomy patients by using only one device both for Physiotherapy and Mastication.
Keywords: flange prosthesis; mandibular defects; mandibular resection; hemimandibulectomy.
Citation: Thakur J. Definitive guiding flange prosthesis for management of hemimandibulectomy: A case report. J Clin Images Med Case Rep. 2021; 2(6): 1502.
Introduction
Odontogenic tumor which are of epithelial origin usually located in the posterior mandible are frequently treated with the surgical excision which is the major cause for mandibular deviation [1]. The treatment of malignant tumors of the oral cavity usually requires the resection of fundamental structures for mastication, deglutition, and speech. As a general rule, the resection of a portion of a mandible without loss of mandibular continuity is not as debilitating as a resection that compromises the mandibular continuity [1,2]. Loss of the proprioceptive sense of occlusion following segmental mandibulectomy leads to the uncoordinated, less accurate movements of the mandible [2]. The basic rehabilitation purpose is to re-educate mandibular muscles to re-establish an acceptable occlusal relationship (physio-therapeutic function) for residual mandible, so that patient could control adequately and repeatedly opening and closing mandibular movements. Guiding Flange Prosthesis (GFP) is a mandibular prosthesis fabricated for the patient who is able to acquire an appropriate mediolateral position of the mandible but is unable to repeat this position consistently for adequate mastication [3].
Cantor and Curtis have classified the mandibular defects into 6 categories [4,5].
Class I: Mandibular resection involving alveolar defect with preservation of mandibular continuity
Class II: Resection defects involve loss of mandibular continuity distal to the canine area
Class III: Resection defect involves loss up to the mandibular midline region
Class IV: Resection defect involves the lateral aspect of the mandible, but is augmented to maintain pseudo articulation of the bone and soft tissues in the region of the ascending ramus
Class V: Resection defect involves the symphysis and parasymphysis region only, augmented to preserve bilateral temporomandibular articulations
Class VI: Similar to class V, except that the mandibular continuity is not restored
Various designs of prostheses either mandibular-based or palatal-based, anchored on natural teeth or the denture flange have been employed to re-establish normal mandibular function. This case report describes the prosthodontic rehabilitation of a patient with hemimandibulectomy using a mandibular definitive cast partial framework prosthesis with a guide flange.
Case report
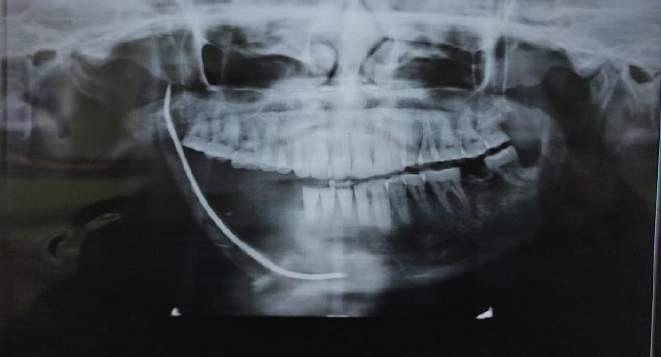
A male patient, 55 years of age, visited the Department of prosthodontics, peoples college of dental sciences and research centre, Bhopal. The chief complaint was of deviation of mandible to the right when closing his mouth and inability to chew properly, following mandibular surgery 3 years ago. Preoperative history and examination revealed that the patient was diagnosed with Ameloblastoma involving the right side of the mandible. The patient had undergone surgical removal of the right half of mandible. Postsurgical radiographs revealed no grafts were placed to reconstruct the defect, but the discontinuity of the mandible was restored using kischner wire (Figure 3). Intraoral examination revealed a complete absence of mandibular left segment. Also, revealed thick freely movable soft tissue scar formation, loss of alveolar ridge, and obliteration of buccal and lingual sulci on the right side (Figure 4). On opening, the mandible showed about 8-9 mm of deviation from midline toward the resected side due to the effect of normal right mandibular depressor muscle (Figure 1 and 2). The defect crossed the midline and hence could be classified as Cantor and Curtis classification-III. No immediate treatment such as inter-maxillary fixation and/or physiotherapy program was provided to the patient. Therefore, dual purpose definitive metal guidance prosthesis was fabricated to provide the patient with proper function and esthetics and to re-educate the mandibular muscles into an acceptable occlusal relationship.



Designing of the prosthesis
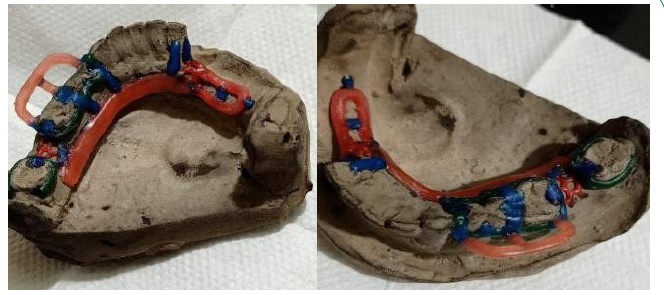
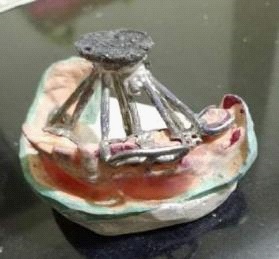
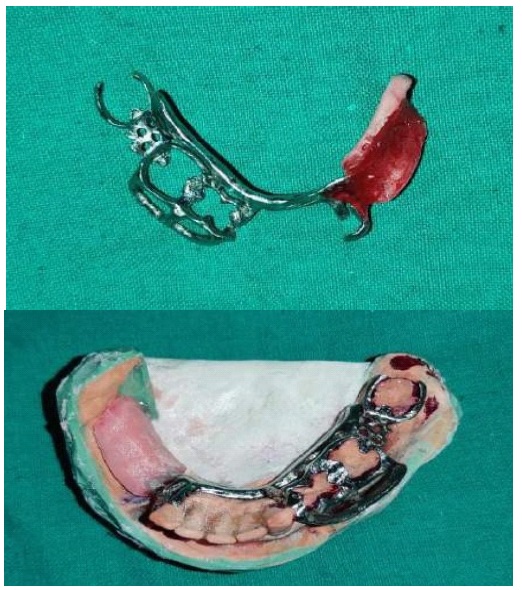
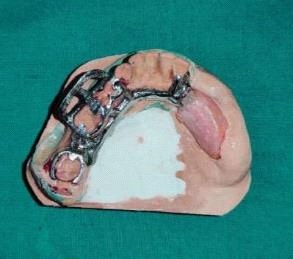
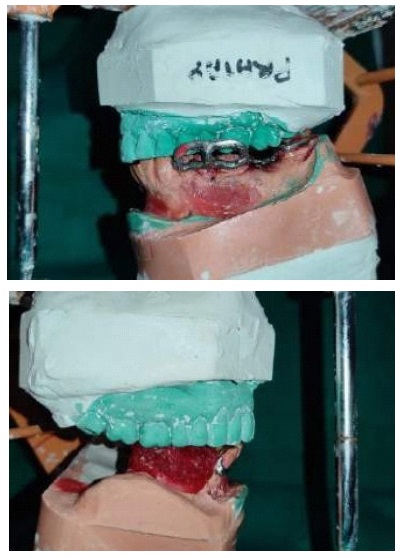
Fabrication started with the impression made from alginate and formation of suitable mandibular and maxillary casts (Figures 5 and 6). The diagnostic casts were surveyed (Figure 7) and undercuts were blocked. The design of the partial denture framework was outlined (Figure 8) and mouth preparation was done. Final impression was made in light body and rubber base material and master cast is poured (Figure 9). The master cast was duplicated in agar and refractory cast was poured. On the refractory cast the wax pattern was adapted (Figure 10). The metal framework wax pattern consisted of major connector i.e., lingual bar, embrasure clasps on posterior teeth on the unresected side. The guide flange was extended 7-10 mm laterally and superiorly on the buccal aspects of the bicuspids and molars from the shoulder portion of the direct retainer on the un-resected side. This flange would engage the maxillary teeth during the mandibular closure, thereby directing the mandible into an appropriate intercuspal position. The angulations of the guiding ramp were fabricated using wax records of the posterior teeth with approximately 3 mm separation and mandible deflected maximally toward the un-resected side. The sprues were attached, wax pattern was invested and casting was done (Figure 11). The casting was retrieved, it was finished and polished (Figure 12). The partial denture framework was verified in the mouth and adjusted using rouge and chloroform or disclosing wax. For performing altered cast technique, the double spacer wax adapted over minor connector and a record base was fabricated (Figure 13). Final impression was made using tissue conditioner (Figure 14). Master cast was sectioned and adaption was checked by placing the framework over it (Figure s 15 and 16). Serration were made on master cast for better interlocking of the sectioned pieces (Figure 17). Beading and boxing (Figure 18) were done to pour altered cast and final framework was seated to check its adaptation over the altered master cast (Figure 19). Bite registration was done use bite registration tray (Figure 20) and jaw relation done and cast was mounted over mean value articulator (Figure 21). Teeth arrangement and try in was done and checked for the occlusion (Figure 22). The complete framework was processed in heat-polymerized acrylic resin (Dental Products of India, Mumbai, India) (Figure 23). Selfcure acrylic was adapted over the metal guide flange present in the framework and buccal indentation was recorded of opposing maxillary teeth in occlusion to guide the mandible in certain closing point (Figure 24). The final prosthesis was delivered after checking the proper seating of framework and angulation of guide flange (Figure 25).
















Discussion
Mandibular discontinuity leads to deviation of residual mandibular segment toward the defected side and rotation of the mandibular occlusal plane inferiorly [1,2]. This mandibular deviation is due to the uncompensated effect of the contra-lateral muscles, particularly the medial pterygoid muscle. If this effect is left uncompensated, the reduction of the cicatricial tissue on the resected side will fix the remaining fragment in its deviated position. This situation causes facial deformity and functional loss [2,5]. The earlier the mandibular guidance therapy is started in the course of treatment the more successful the patient’s definitive occlusal relationship is restored [6]. The primitive rehabilitation purpose in this case was to retrain mandibular musculatures to regenerate a satisfactory occlusal relationship for residual mandible and to reinsate the mastication [6,7]. There are various treatment modalities for such patients are maxilla mandibular fixation, implant supported prosthesis, removable mandibular guiding flange and palatal based guidance restorations. An implant supported prosthesis cannot be a treatment of choice as bone grafting is not done [8,9]. The removable appliances can be adjusted according to the patient’s need. Mandibular guide flange is given for hemimandibulectomy cases, it consists of a removable partial denture framework with a flange extending 7–10 mm laterally and superiorly on the buccal aspect of the premolars and molars on the non-defect side. This flange engages the maxillary teeth during mandibular closure, thereby directing the lower jaw to an appropriate intercuspal position. The guidance flange may be fabricated either of cast chrome-cobalt metal or acrylic resin. The material of choice will depend on the pre-existing occlusal relationship of the patient and the need for adjustment. The success of the mandibular guidance rehabilitation depends on the nature of the surgical defect, patient co-operation, and prosthetic management with early physiotherapy program [10]. The prime concern before treating this case were that no immediate treatments such as inter-maxillary fixation or physiotherapy was given, the amount of time intervened from surgery, procrastination in rehabilitation procedures, and loss of muscle co-ordination in the lower jaw, which prevented the normal functions. In spite of all these cons the factors that helped us to attain the required outcome were the patient motivation, remaining tongue, floor of the mouth, and its adjoining soft tissues. The patient had all his teeth, expect those on the resected side that helped him to have well proprioceptive sense and acquire the functional position after the insertion of the prosthesis. Definitive mandibular guidance therapy would help the patients in such cases to re-establish a satisfactory occlusion by re-educating the mandibular muscles and undergo normal function and mastication [2]. The GFP can be regarded as a training type of prosthesis. If the patient can successfully repeat the mediolateral position, the GFP can often be discontinued.
Conclusion
Rehabilitation of a long standing hemimandibulectomy case without any earlier intervention is a challenging task, due to the lack of bone support and loss of muscle co-ordination. Mandibular guidance prostheses are normally employed on an intermediate basis. However, in a long-standing case, definitive mandibular guidance prosthesis with a metal guiding flange and acrylic teeth on the resected side to stabilize the occlusion can be given to re-adjust the deviation and acquire acceptable occlusion for normal mandible functioning.
References
- Beumer J III, Curtis TA, Marunick MT. Maxillofacial Rehabilitation. Prosthodontic and Surgical consideration. St. Louis: Ishiyaku. Euro America. 1996; 113-224.
- Taylor TD. Diagnostic considerations for prosthodontic rehabilitation of the mandibulectomy patient. In: Taylor TD, editor. Clinical maxillofacial prosthetics. Chicago: Quintessence Publishing. 2000; 155–170.
- Patil PG, Patil SP. Guide flange prosthesis for early management of reconstructed hemimandibulectomy: A case report. J Adv Prosthodont. 2011; 3: 172–6.
- Fonsica RJ, Davis WH. Reconstruction Preprosthetic oral and maxillofacial surgery, 2nd Ed. WB Saunders Company. 1063-7
- Curtis DA, Plesh O, Miller AJ, Curtis TA, Sharma A, Schweitzer R, Hilsinger RL, Schour L, Singer M. A comparison of masticatory function in patients with or without reconstruction of the mandible. Head Neck. 1997; 19: 287–296.
- Desjardins RP. Occlusal considerations for the partial mandibulectomy patient. J Prosthet Dent. 1979; 41: 308-15.
- Mathew A, Thomas S. Management of a hemi-mandibulectomy defect with a definitive guiding flange prosthesis. Pushpagiri Med J. 2012; 3: 132–4.
- Sahu SK. Mandibular guide flange prosthesis following mandibular resection; a clinical report. J Clin Diagn Res. 2010; 4: 3266– 70.
- Robinson JE, Rubright WC. Use of a guide plane for maintaining the residual fragment in partial or hemimandibulectomy. J Prosthet Dent. 1964; 14: 992–9.
- McGarry TJ, Nimmo A, Skiba JF, Ahlstrom RH, Smith CR, Koumjian JH, et al. Classification system for partial edentulism. J Prosthodont. 2002; 11: 181–93.