
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Cardiology fellowship in the era of coronavirus disease (COVID 19)
Mohammad Al Akchar1; Mohsin Salih1; Mukul Bhattara1; Khalid Sawalha2; Abdul Moiz Hafiz1*
1 Division of Cardiology, Southern Illinois University School Of Medicine, Springfield IL, USA
2 Department of Internal Medicine, UMMS Baystate, USA.
*Corresponding Author: Mohammad Al-Akchar
Division of Cardiology, Southern Illinois University,
701 North First Street, Springfield, IL 62781, USA.
Email: mal-akchar68@siumed.edu
Received : Nov 10, 2021
Accepted : Dec 16, 2021
Published : Dec 23, 2021
Archived : www.jcimcr.org
Copyright : © Al-Akchar M (2021).
Citation: Akchar MA, Salih M, Bhattara M, Sawalha K, Hafiz AM. Cardiology fellowship in the era of coronavirus disease (COVID 19). J Clin Images Med Case Rep. 2021; 2(6): 1506.
Introduction
Since Coronavirus disease (COVID-19) was declared a pandemic on 3/12/2020 by the World Health Organization (WHO), diagnosed cases have continued to be on the rise worldwide, even though rates of new case detection seem to be stabilizing here in the United States [1]. This pandemic has impacted delivery of healthcare as well as health care workers in many aspects. In this article we discuss the impact of COVID-19 on cardiology fellowship training, early career concerns of fellows in training, and some suggestions to help training programs to cope with these challenges. It remains unclear how this pandemic will impact our health systems for the foreseeable future and thus a call to action is needed to reassess education needs and strategies of trainees during the pandemic not only in the interest of our FITs but also their future patients.
Education
The medical education of cardiology fellows witnessed academic and clinical changes in terms of quality and quantity. Initially, in our institution at the Southern Illinois University School of Medicine, conferences were halted to meet recommendations of social distancing until deemed safe eventually and alternative educational formats could be instituted. Furthermore, the design of clinical rounds and bedside teaching changed from a bedside rounding strategy to table rounding strategy where staffing of patients occurs over the phone whenever possible to protect the consultant teams. Only primary teams and, when appropriate, non-trainees could physically see patients with confirmed COVID-19 status or those who were high risk patents and under investigation. Following this, recommendations were made over the phone.
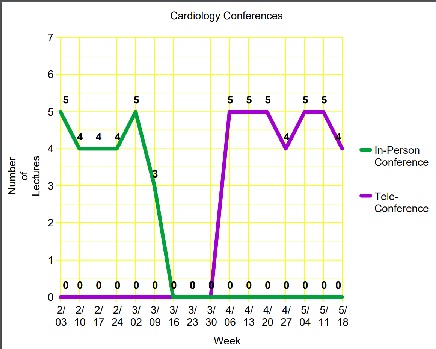
Need for above changes created their own set of challenges for training and medical education. The exposure for the cardiology fellows on the inpatient consultative service decreased and bedside training also decreased. Similar to other institutions [2], this created room for innovation and change. Conferences were re-instituted as tele-conferences, with maintenance of prior conference schedules. Graph in figure 1 one shows weekly conference count before and after changes during COVID-19 pandemic. Several institutions and organizations created and promoted online content and made them available to fellows in-training for example the Iowa local chapter of the American College of Cardiology, and American Society of Nuclear Cardiology [3]. This provided further material available to be incorporated in the educational curriculum of fellows. To mimic the interactive nature of in person meetings, questions were asked through the chat option of the online portals and answered by faculty. In addition, there were numerous regional webinars held by different organizations including one by our own faculty in partnership with the Downstate IL ACC chapter [4].
Patient care
Out-patient care
Another challenge during this pandemic was taking care of patients in an adequate and safe manner. We used this as an opportunity for innovation. Our medical school had a pre-existing telehealth service line that was not as heavily utilized prior to the pandemic. However, now not unlike other institutions and training programs [5,6], our institution started to lean heavily on tele-medicine platforms to continue to serve the community of central and southern Illinois. We would be remiss to not mention the role played by the updated Centers for Medicare and Medicaid Services (CMS) guidelines relaxing rules regarding delivery of health care via telemedicine, in making telemedicine the mainstream method of healthcare delivery esp in the outpatient arena [7] during the peak of the pandemic. The outpatient weekly fellow half-day clinic adapted to include more patients and have an attending available on site in a different room to staff and communicate with the patient.
In-patient care
On the in-patient side, fellows reading echocardiogram studies and nuclear studies were asked to do so from home. Feedback was given on every study utilizing a built-in form (Figure 2). In addition, communication between fellows and attending to explain certain aspects related to study was done utilizing cell-phone conversation.

The inpatient fellow on consultative service would perform either table-rounds or virtual rounds through video conferencing to discuss patients. Residents rounding on cardiology service were asked to alternate staying home for half of the week to prevent the full team from rounding together and jeopardizing everyone on the team at the same time. Such models aren’t new and have been proposed in, for instance cardiac catheterization laboratory coverage during such crises by SCAI. (e.g. the cluster team call model or the home/hospital model) [8]
Procedures
Many clinical aspects of the cardiovascular medicine fellowship training are weighted more heavily toward acquiring proficiency with certain procedures. These procedures must be repeated and certain volume milestones met for being skilled enough as an independent operator, as reflected in the ACC Core Cardiovascular Training Statement (COCATS) requirements from time to time [9,10]. Thus not surprisingly COVID-19 might dramatically impact training given the drop in a number of procedures including Percutaneous Coronary Interventions (PCI) for ST elevation Myocardial infarction (decrease up to 48%) [11] that happened during the pandemic. In addition, elective procedures were put on hold/cancelled in many institutions including ours, as well as others [12]. This led to an overall decrease in procedural training including coronary angiography and TransEsophegeal Echocardiography (TEE). While the Accreditation Council for Graduate Medical Education (ACGME) did leave it up to the program directors to decide on the competency of procedural skills [13,14], the drop in volumes did create both anxiety and room for innovation amongst programs. For example, procedural rotations (i.e. catheterization laboratory) were rescheduled to later dates during the general cardiology fellowship. In addition, cardiology fellows needing TEE exposure were allowed to scrub in with intraoperative TEE for valvular and bypass procedures. With the slow re-introduction of elective procedures, we anticipate that these numbers will continue to grow. It is out of scope of this paper to discuss the effect on interventional cardiology fellowship training programs, as we only have a general cardiology fellowship at our school.
Recruitment
One additional obstacle that arises is recruitment for the next season of fellowship interviews for the year of 2021-2022 start date. Many innovative solutions have been suggested including an innovative approach by non-cardiology programs in Chicago [15]. The interview process was held online through video conference platforms. In addition, utilizing the institution’s website, short videos of introductions related to the program were done by the faculty. We anticipate that cardiology fellowship programs will do the same when conducting interviews. Not only is this form of interviewing beneficial for this era, but it could also be a potential form of interviewing in the non-covid era, limiting the costs for both the programs and the applicants, and potentially allowing for multiple interviews across different institutions to be conducted in the same day. Our cardiology fellowship program is also considering conducting fellowship interviews online if needed in the upcoming interview season.
Jobs
Another challenge facing soon-to-graduate cardiology fellows is the job hunt given restriction on travel during the pandemic as well the economic impact on hospitals and funding potentially affecting hiring. The pandemic has resulted in several institutes asking physicians for voluntary furlough, as well as seek early retirement [16]. In some cases new hire contracts could be cancelled as the practice might not have the financial backbone any more to add new partners as the financial impact of the pandemic has been felt across the healthcare industry like many others. The full scope of the pandemic might be even more complex. As more patients lose employment, many will cancel or delay elective procedures. In addition it remains unknown what percentage of elective procedures will begin to be offered routinely compared to the past at hospitals which could affect the financial stability of many health care institutions and their ability to provide services and hire or retain staff. While the need for physicians continues to exist, we anticipate that job security will probably still remain, however, the reimbursement and method of recruitment will be affected. For example virtual recruitment will start to rise [17]. In addition, local recruitment of graduates might become more prevalent.
Conclusion
COVID-19 pandemic has definitely created many challenges to training programs across different avenues including patient care, medical education, and procedural training. At the same time, it has created room for innovation and collaboration in both medical education and patient care.
Disclosures: All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
References
- Prevention CfDCa. Coronavirus Disease 2019 (COVID-19). 2020.
- Potts JR, 3rd. Residency and Fellowship Program Accreditation: Effects of the Novel Coronavirus (COVID-19) Pandemic. Journal of the American College of Surgeons. 2020; 230:1094-1097.
- Cardiology ASoN. ASNC Nuclear Cardiology Virtual Elective. 2020.
- ACC DIC. COVID 19 Downstate IL Chapter ACC. 2020.
- Chick RC, Clifton GT, Peace KM, Propper BW, Hale DF, Alseidi AA, et al. Using Technology to Maintain the Education of Residents During the COVID-19 Pandemic. Journal of surgical education. 2020.
- Oldenburg R, Marsch A. Optimizing teledermatology visits for dermatology resident education during the COVID-19 pandemic. Journal of the American Academy of Dermatology. 2020; 82: e229.
- CMS.gov. Additional Background: Sweeping Regulatory Changes to Help U.S. Healthcare System Address COVID-19 Patient Surge. 2020.
- Szerlip M, Anwaruddin S, Aronow HD, Cohen MG, Daniels MJ, Dehghani P, et al. Considerations for cardiac catheterization laboratory procedures during the COVID-19 pandemic perspectives from the Society for Cardiovascular Angiography and Interventions Emerging Leader Mentorship (SCAI ELM) Members and Graduates. Catheterization and cardiovascular interventions : Official journal of the Society for Cardiac Angiography & Interventions. 2020.
- King SB, 3rd, Babb JD, Bates ER, Crawford MH, Dangas GD, Voeltz MD, et al. COCATS 4 Task Force 10: Training in Cardiac Catheterization. Journal of the American College of Cardiology. 2015; 65: 1844-1853.
- Ryan T, Berlacher K, Lindner JR, Mankad SV, Rose GA, Wang A. COCATS 4 Task Force 5: Training in Echocardiography. Journal of the American College of Cardiology. 2015; 65: 1786-1799.
- Solomon MD, McNulty EJ, Rana JS, Leong TK, Lee C, Sung SH, et al. The Covid-19 Pandemic and the Incidence of Acute Myocardial Infarction. The New England journal of medicine. 2020.
- Gupta T, Nazif TM, Vahl TP, Ahmad H, Bortnick AE, Feit F, et al. Impact of the COVID-19 pandemic on interventional cardiology fellowship training in the New York metropolitan area: A perspective from the United States epicenter. Catheterization and cardiovascular interventions : Official journal of the Society for Cardiac Angiography & Interventions. 2020.
- Education ACf GM. ACGME Response to the Coronavirus (COVID-19) 2020.
- Sawalha K, Al-Ali M, Sawalha A, Ko H, Abdelli I, El-Shawish S, Hussien A. Factors influencing academic motivation among UOS medical students. Journal of Health Science. 2017; 5: 177-180.
- Vining CC, Eng OS, Hogg ME, Schuitevoerder D, Silverman RS, Yao KA, et al. Virtual Surgical Fellowship Recruitment During COVID-19 and Its Implications for Resident/Fellow Recruitment in the Future. Annals of surgical oncology. 2020: 1-5.
- AMA. Pandemic significantly alters the job market for residents, fellows. 2020.
- KAISER PERMANENTE SCPMG. Coronavirus and COVID-19. 2020.