
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Clinical presentation and surgical resolution of atypical non-adenomas adrenal tumors
Nicole Lustig1; Pablo Rojas2; Thomas Uslar1,6; Roberto Olmos1; Francisco J Guarda1; Virginia Iturrieta3; Eugenia Ortiz3; Onzalo Méndez4,6; Joaquín Jerez5; Álvaro Zúñiga2,6; Ignacio F San Francisco2,6; René Baudrand1,6*
1 Endocrine Department, University in Santiago, Chile.
2 Urology Department, University in Santiago, Chile.
3 Endocrine Department, University of the Frontier, Chile
4 Pathology Department, University in Santiago, Chile.
5 Internal Medicine Department, University in Santiago, Chile.
6 Program for Adrenal Disorders, CETREN UC, Santiago, Chile.
*Corresponding Author: René Baudrand
Program for Adrenal Disorders, CETREN UC, Santiago, Chile.
Email: rbaudran@uc.cl
Received : Nov 20, 2021
Accepted : Dec 16, 2021
Published : Dec 23, 2021
Archived : www.jcimcr.org
Copyright : © Baudrand R (2021).
Abstract
Adrenal tumors are very common in medical practice, including a wide spectrum of etiologies. Although most of them are adenomas, infrequent lesions can become a diagnostic and therapeutic challenge for clinicians. Here we present two atypical cases of non-adenomas adrenal tumors with specific imaging, biochemical profile, and surgical resolution.
The first case is a 54-year-old woman with a history of hypertension and type 2 diabetes, with an incidentally discovered 7 cm adrenal mass on CT, compatible with a myelolipoma. Biochemical work-up was remarkable for hypersecretion of both cortisol and aldosterone. She underwent laparoscopic adrenalectomy. During follow-up, biochemical cure of hormonal hypersecretion was confirmed.
The second case is a 44-year-old woman in whom a 7 cm left non-adenoma adrenal mass was diagnosed incidentally by magnetic resonance. Complete hormonal screening was normal. Laparoscopic adrenalectomy was performed. Biopsy informed a solid neoplasm separated from normal adrenal tissue, with immunohistochemistry compatible with a Schwannoma.
These case vignettes describe atypical adrenal cases that should be considered in the differential diagnosis of non-adenomas adrenal tumors. They represent uncommon presentations and illustrate the importance of an appropriate multidisciplinary evaluation of adrenal tumors, in order to improve the surgical and clinicalmanagement of these patients.
Keywords: adrenal incidentaloma; adrenal tumor; adrenal myelolipoma; adrenal schwannoma.
Citation: Lustig N, Rojas P, Uslar T, Olmos R, Baudrand R, et al. Clinical presentation and surgical resolution of atypical nonAdenomas adrenal tumors. J Clin Images Med Case Rep. 2021; 2(6): 1507.
Case report
Adrenal tumors are very common in medical practice since abdominal imaging is more commonly performed [1]. Most of these tumors are apparently “non-functioning” adenomas, but less common lesions can be found which can generate difficulties among healthcare professionals [2]. Hence, clinicians need to be aware of these infrequent entities to determine an accurate diagnosis, hormonal profiling, and proper management.
Case I
A 54-year-old woman with a history of arterial hypertension and Type 2 Diabetes Mellitus (T2DM). Abdominal ultrasound showed a right adrenal mass with solid and cystic components. A Computed Tomography (CT) was performed (Figure 1) showing a 7.3 X 5.5 cm very low-density lesion consistent with adrenal myelolipoma. Pre-operative blood tests were requested and impressively displayed mild hypersecretion of both cortisol and aldosterone (Table 1). Laparoscopic right adrenalectomy was performed.

Table 1:
Case 1- Test (normal value) |
Pre-surgery |
Post-surgery |
Aldosterone (1.8-23.2 ng/dL) |
9.35 |
9.93 |
Plasma renin activity (1.3-4 ng/ml/hr) |
0.26 |
1.1 |
Aldo/PRA |
35.9 |
9.02 |
Dexamethasone Supression Test (<1.8 ug/dL) |
2.0 |
|
Nocturnal salivary cortisol I y II (<0.1 ug/dL) |
< 0.02 |
|
Plasma cortisol (6.2-19.4 ug/dL) |
|
5.3 |
ACTH (10-60 pg/mL) |
14 |
72 |
Urinarymetanephrine (52-341 ug/24 hrs) |
35 |
|
Urinary normetanephrine (88-444 ug/24 hrs) |
144 |
|
Table 2:
Case 2 |
|
|
Aldosterone (1.8-23.2 ng/dL) |
23,9 |
|
Plasma renin activity (1.3-4 ng/ml/hr) |
6 |
|
Aldo/PRA |
3,9 |
|
Urinary free cortisol (normal < 110 ug/24h) |
41,2 |
|
DHEAS (< 420 ug/dL) Urinary metanephrine (52-341 ug/24 hrs) |
146
31,9 |
|
Urinarynormetanephrine (88-444 ug/24 hrs) |
|
242 |
|
|
|
Twenty-four hours after surgery, blood tests revealed hypocortisolism, which was successfully supplemented, confirming mild Autonomous Cortisol Secretion (ACS). The patient did not require antihypertensive therapy after surgery and biochemical cure with normalization of renin values was documented.
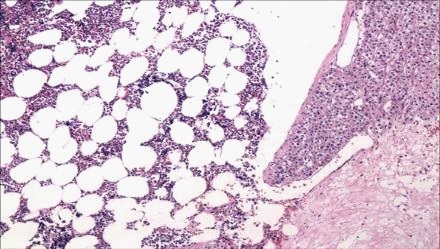
Biopsy (Figure 2) showed an ovoid formation of 7.5 X 6.5 X 3.3 cm, compatible with adrenal co-secreting myelolipoma (mild ACS and mild primary aldosteronism).
Case II
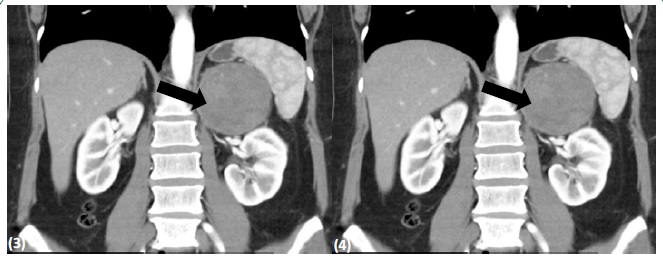
A 44-year-old woman with a four-month history of low back pain, without any other symptoms nor any findings in physical examination. Spinal Magnetic Resonance Imaging (MRI) showed an adrenal mass and an abdominal CT scan confirmed the presence of a homogeneous, non-adenomatous, juxta-adrenal 7 cm mass (Figures 3 and 4). No hypersecretion was observed in the screening tests (Table 1).
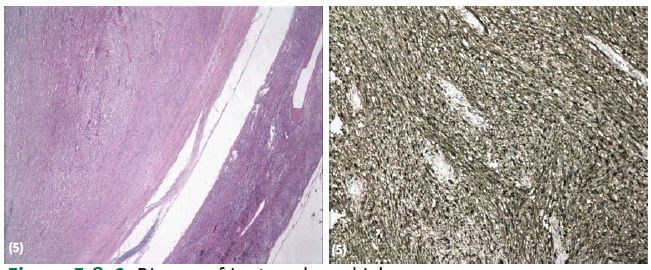
Left laparoscopic adrenalectomy was performed without incidents. Biopsy (Figures 5 and 6) showed a solid neoplasm with Verocay bodies separated from adrenal tissue by a thin capsule. Immunohistochemistry stained positive for protein S-100 (+) and negative for H-caldesmon, CD34, and DOG-1, compatible with Schwannoma. The adjacent adrenal tissue was normal.
Discussion
Our case series describes two uncommon adrenal cases of non-adenomas adrenal tumors; a functional co-secreting myelolipoma and a yuxta-adrenal Schwannoma.
Adrenal myelolipomas are predominantly unilateral, formed by hematopoietic and adipose tissue with an incidence of 0.03% [3]. They are rarely functioning and, to our knowledge, co-secretion of aldosterone and cortisol has not been reported in the literature. These tumors are often found incidentally in imaging studies [4] and can co-exist with Cushing syndrome, pheochromocytoma, primary aldosteronism, and congenital adrenal hyperplasia. Bilateral [5] and hormone-secreting masses [6] are scarcely reported. One report of cortisol secreting myelolipoma and another with DHEA-S secretion have been published [6]. Regarding management, surgical removal is recommended in symptomatic adrenal myelolipomas, secreting lesions and in those larger than 6 cm because of hemorrhage risk. Laparoscopy is the preferred surgical approach. Most cases of small myelolipomas should be followed with imaging techniques.
Regarding Schwannomas, these tumors were first described in 1908 by Verocay. Conventional and cellular schwannomas exhibit strong and diffuse immunohistochemical positivity for S-100 protein. They are usually benign, non-secreting and asymptomatic tumors originating from nerve sheaths formed by Schwann cells. They have been scarcely reported as adrenal lesions [7]. Adrenal schwannoma on CT appears as a homogeneous, round, and well-circumscribed lesión, rarely may present with degenerative changes, such as calcification, hemorrhage, or cystic formation [8].
The differential diagnosis must be done with other non-adenomas tumors such as pheochromocytoma, adrenal carcinoma or adrenal sarcoma. Malignant transformation may be found in association with von Recklinghausen disease or neurofibromatosis [9]. CT image typically appears as a homogeneous lesion as our case; however, calcification, hemorrhage, or cystic formation could lead to heterogeneous enhancement [9]. Laparoscopy is the preferred surgical approach.
Declarations
Acknowledgements: The authors thanks to all collaborators of urology and endocrinology departments.
Conflicts of interest: The authors declare no conflicts of interest.
Ethics approval and consent to participate: Permission to conduct the study was granted by the Biomedical Ethics Research Committee of Pontificia Universidad Católica de Chile.
Consent for publication: All the patients mentioned in this article gave a written informed consent for their data to be published.
Funding: Fondecyt 1190410.
References
- Barzon L, Sonino N, Fallo F, Palu G, Boscaro M. Prevalence and natural history of adrenal incidentalomas. European Journal of Endocrinology. 2003; 149: 273–285.
- Fassnacht M, Arlt W, Bancos I, Dralle H, Newell, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. European Journal of Endocrinology. 2016; 175: G1–G34.
- Bishoff JT, Waguespack RL, Lynch SC, May DA, Poremba JA, Hall CR. Bilateral symptomatic adrenal myelolipoma. J Urol. 1997; 158: 1517-1518.
- Hsu SW, Shu K, Lee WC, Cheng YT, Chiang PH. Adrenal myelolipoma: A 10-year single-center experience and literature review. Kaohsiung J Med Sci. 2012; 28: 377-382.
- Zattoni D, Balzarotti R, Rosso R. The management of bilateral myelolipoma: Case report and review of the literature. Int J Surg Case Rep. 2015; 12: 31-36.
- Brogna A, Scalisi G, Ferrara R, Bucceri AM. Giant secreting adrenal myelolipoma in a man: A case report. J Med Case Rep. 2011; 15: 298.
- Limberg J, Stefanova D, Ullmann T, et al. Not all laparoscopic adrenalectomies are equal: Analysis of postoperative outcomes based on tumor functionality. Surgical Endoscopy. 2020.
- Adas M, Ozulker F, Adas G, Koc B, Ozulker T, Sahin IM, et al. A rare adrenal incidentaloma: Adrenal schwannoma. Case Rep Gastroenterol. 2013; 7: 420-427.
- Thomas MB, Stephen J. Adrenal Schwannoma: A rare adrenal incidentaloma. International Surgery Journal. 2018; 5.5: 1967- 1969.