
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Intramedullary spinal cord abscess: A grave complication of a dermal sinus tract
Edward Goacher; Katerina Apostolopoulou*; Annick Wilson; John Mc Mullan; Patricia De Lacy; Hesham Zaki; Shungu Ushewokunze
Department of Neurosurgery, Sheffield Children’s Hospital NHS Foundation Trust, Sheffield, United Kingdom.
*Corresponding Author: Katerini Apostolopoulou
Department of Neurosurgery, Sheffield Children’s Hospital NHS Foundation Trust, Sheffield, United Kingdom.
Email: Katerina.apostolopoulou@nhs.net
Received : Nov 03, 2021
Accepted : Dec 17, 2021
Published : Dec 24, 2021
Archived : www.jcimcr.org
Copyright : © Apostolopoulou AK (2021).
Abstract
Congenital dermal sinus tracts are an uncommon form of spinal dysraphism. If identified and treated early, outcomes are favourable. If missed, complications can be significant. Intramedullary spinal cord abscess is a rare but catastrophic complication. We report the case of an infantile patient with an intramedullary spinal cord abscess occurring 2-months post treatment for a coliform meningitis with an unidentified dermal sinus tract. We examined the literature on the investigation and management of dermal sinus tracts and conclude that all cases of unexplained, atypical meningitis in an infant should trigger suspicion for an underlying dermal sinus tract. In such cases, an MRI scan of the neuroaxis should be performed urgently.
Keywords: syrinx; dimple; meningitis; dysraphism.
Abbreviations: DST: Dermal Sinus Tract; E. Coli: Escherichia Coliform.
Citation: Goacher E, Apostolopoulou K, Wilson A, Mullan JM, Lacy PD, Zaki H, et al. Intramedullary spinal cord abscess: A grave complication of a dermal sinus tract. J Clin Images Med Case Rep. 2021; 2(6): 1511.
Introduction
Intramedullary spinal cord abscesses can lead to a catastrophic sequalae of complications including paralysis, bowel and bladder dysfunction, sepsis and even death. They may occur anywhere from the craniocervical junction to the filum terminale, with clinical presentation varying, depending on the location and extent of cord compression. Standard treatment is surgical drainage and excision followed be long term intravenous antibiotics therapy. Most commonly, their source is cardiopulmonary with haematogenous spread [1]. However, they may also occur secondary to contiguous infection from a Dermal Sinus Tract (DST) [2,3].
DSTs are an uncommon form of spinal dysraphism occurring in 1 in 2500 births [4,5]. They develop due to incomplete formation of the neuroectoderm in early gestation, occurring most commonly in the lumbar and lumbosacral regions [4]. Associated anomalies include tethered cord, split cord malformations and inclusion tumours [4,6,7]. DSTs may display variable clinical presentation, ranging from an asymptomatic cutaneous lesion to sudden acute neurological deterioration [8]. Intramedullary spinal cord abscess is a rare complication of a congenital dermal sinus tract. More commonly, the infective sequalae of congenital dermal sinus tract may result in soft tissue infection, meningitis, extradural or subdural abscesses.
Here we report the case of a female infant who developed an intramedullary spinal cord abscess 2-months after treatment for an Escherichia Coliform (E. Coli) meningitis, secondary to an unidentified congenital DST.
Case presentation
A 6-month-old female child was referred to the tertiary neurosurgical service with a sudden loss of lower limb tone bilaterally and increasing irritability for 2 days. The child had been treated 2-months previously for E. Coli meningitis. A small sacral dimple had been noted on both her new-born examination and hospital admission for E. Coli meningitis, but not investigated for an underlying DST. Born at term by normal vaginal delivery, the child was previously fit and well prior to her meningitis.
On examination the child displayed flaccid paralysis (MRC power grade 0 throughout) and are flexia of the lower limbs bilaterally. She was found to have a sensory level of T6. A sacral dimple over the spinal midline measuring 1cm by 1cm with a red, crusted centre was found on examination of the spine. No discharge was elicited on digital compression from the lesion. Inflammatory markers were raised on admission (C-Reactive Protein 88, White Cell Count 25.95).
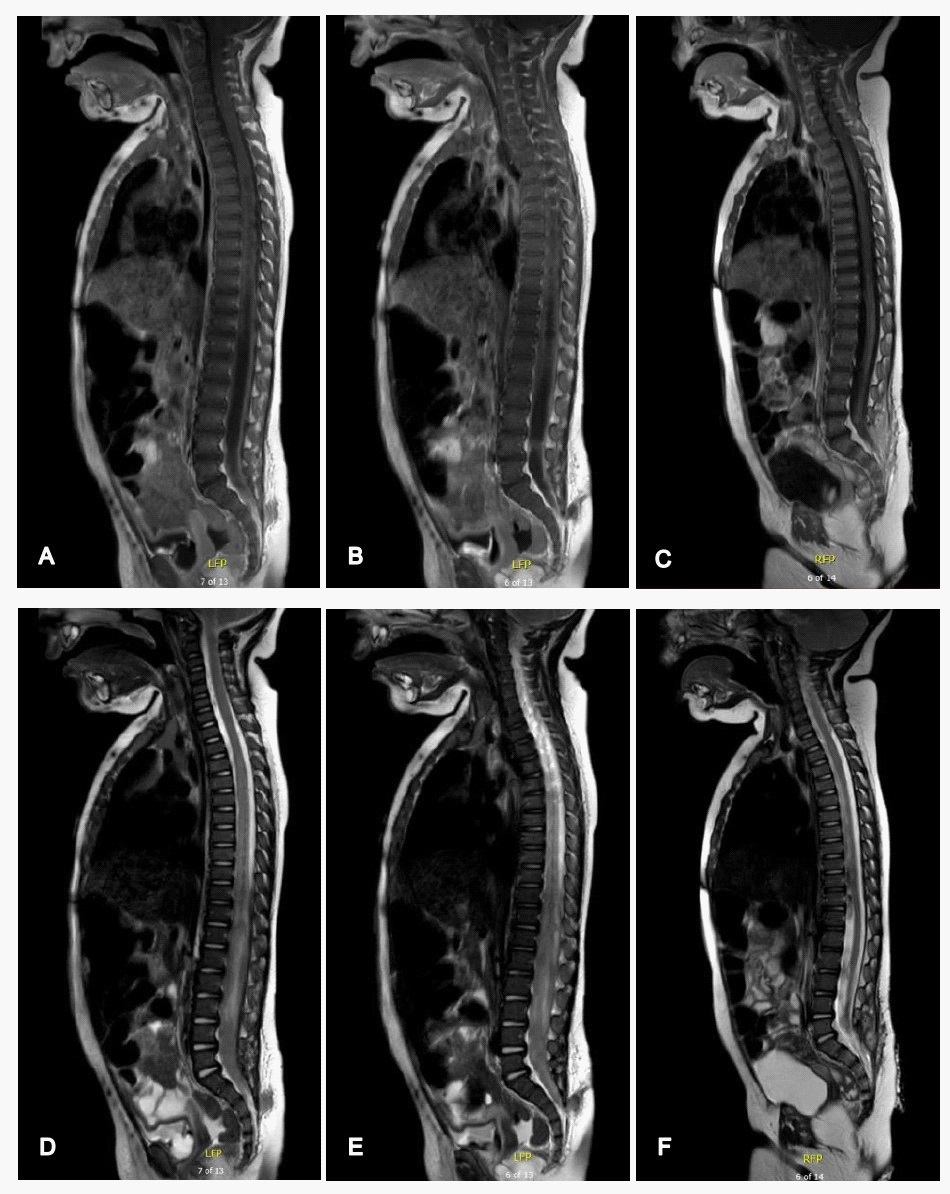
A neural axis MRI scan (Figure 1) revealed a lipomyelomeningocele with a dermal sinus connection to the skin and a cord syrinx containing purulent material from the T4 level down to the conus medullaris. The spinal cord extended directly through the posterior spinal defect and was tethered to the neural placode within the superficial lipoma at the S3 level.
Broad spectrum antibiotics were immediately commenced, and urgent surgical intervention undertaken. Surgical management involved excision of the dermal sinus, lumbosacral laminectomy (L5 – S1) and intradural washout of pus. Analysis of the pus showed a white cell count of 4600 (90% polymorphs) and cultures grew enterococcus, e. coli and anaerobes. A short course (2-weeks) of dexamethasone was administered postoperatively.
A second surgery was performed due to failure to improve, both clinically and radiologically. The syrinx was drained and the intradural space washed out again. Antibiotic therapy was guided by culture sensitivities. A 6-week course of ceftriaxone, amoxicillin and metronidazole was administered following the second surgery. Bladder dysfunction was initially managed with an indwelling catheter which has since been removed and intermittent catheterisation commenced.
Three weeks following presentation and the initial surgical procedure, lower limb power began to improve. On discharge, right hip flexion (MRC grade 3), right knee extension (MRC grade 3) and right ankle dorsiflexion (MRC grade 1) showed an improvement in power. Left hip flexion (MRC grade 2) and left knee extension (MRC grade 1) showed a minor improvement. Intermittent catheterisation is ongoing. Oxybutynin has been started to aid bladder function. Long term follow-up is continuing under the care of the spinal injuries’ unit incorporating both urological and neurological input.
Discussion
Congenital DSTs occur in 1 in 2500 births secondary to a persistent connection between the neuroectoderm and the cutaneous ectoderm [4,5]. They may occur anywhere from the nasion to the sacrum. The tract may persist from the skin down to neural elements or may terminate in the deep fascia [9]. The most common features of congenital DSTs are cutaneous abnormalities, neurological deficits and infection [4]. Subtle cutaneous abnormalities include midline pits, skin tags, abnormal pigmentation and subcutaneous lipoma. Optimal imaging for DST remains MRI imaging, however ultrasound is becoming increasingly available and has demonstrated a specificity of up to 98% in neonates [10]. In cases where DSTs are identified or suspected, an urgent MRI of the neuroaxis is essential to further characterise the DST and assess for any neural involvement which may require urgent neurosurgical intervention.
Whilst intramedullary spinal cord abscess secondary to DST remains rare, it is not a new phenomenon [2]. In 2018, Prasad et al. reviewed 50 reported cases globally of intramedullary spinal cord abscess secondary to DST, finding Staphylococcus aureus to be the most common causative organism [3]. Common presenting features include fever, acute flaccid lower limb weakness, urinary disturbances, and meningitis. Fever and weakness at presentation were associated with a significantly worse outcome [3]. To our knowledge, this is the first reported case that had been precipitated by a coliform meningitis with an associated sacral dimple.
Sacral dimple incidence is between 1.8-7.2% of new-born infants [11,12]. Visual examination of the dimples alone is not enough to exclude underlying occult dysraphism [13]. Dimples measuring less than 5 mm, within 25 mm of the anus in the midline, not associated with any other cutaneous anomaly are at less risk of underlying occult dysraphism than dimples not adhering to these criterion [14]. A true DST does not occur in the sacrococcygeal region, another useful feature to help guide clinicians distinguish between true DSTs and simple dimples/ pits attached to the tip of the coccyx that are of no dysraphic significance [15]. Despite this, some clinicians feel that exclusion of underlying pathology in any midline cutaneous lesion in the neuroaxis, including sacral dimples, above the gluteal cleft is essential [4]. Advances are being made in investigations of such lesions using sonography, however MRI of the neuroaxis remains the gold standard [13,16,17]. Despite being the gold standard, even MRI may be unreliable at demonstrating the extent of the tract and any associated pathology [15,18].
Investigation of sacral dimples remains debated with some authors suggesting that the low yield of positive findings on sonography renders routine ultrasounds for simple sacral dimples unnecessary. A systematic review of 5166 patients with simple sacral dimples who underwent spinal sonography found only 3.4% had an abnormal finding [19]. An international survey of 62 paediatric neurosurgeons by Ponger et al. found that 48% would not obtain imaging for a patient with a simple sacral dimple, 30% would obtain a spine ultrasound and 22% would obtain an MRI scan [20]. Underlying dermal sinus tracts, the most common differential diagnosis of such dimples, display a favourable outcome in cases of early identification and treatment [14]. However, when missed the complications can be catastrophic, including meningitis, brain abscess, intramedullary spinal cord abscess, missed tethered spinal cords and even death [21,22]. The low yield of positive findings when investigating such dimples must be balanced against the potential devastating sequalae of potential complications from unidentified DSTs.
Bacterial meningitis is a life-threatening condition in which the meninges of the central nervous system become inflamed due to bacterial infiltration. Occurring in 5 - 7 per 100.000, neurological complications are seen in up to 20% of cases [23]. In developed countries, the causative organism in children aged >3 months is either Streptococcus pneumoniae or Neisseria meningitidis in over 80% of cases [24]. Thus, infection with an atypical organism such as E. Coli in this cohort should prompt further investigation as to the underlying mechanism of infection. In neonates <72 hours of age, rates of E. Coli meningitis have been shown to be as high as 30%, however this rate drops to 5% in those infants >72 hours old [25].Whilst bacterial meningitis secondary to E. Coli is notatypical in a neonatal population, an explanation as to the mechanism of infection should still be sought and a DST considered for causative organisms associated with the gastrointestinal tract [24].
Conclusions
This case highlights a number of valuable learning points for clinicians. Firstly, infantile cases of meningitis due to a typical pathogens should undergo a thorough examination of their spine and consideration should be given to spinal MRI. Similarly, unexplained recurrent cases of infantile bacterial meningitis should trigger suspicion for DSTs. Secondly, the gold standard method of investigating for an underlying DST in cases of sacral dimples is via MRI scanning, failure to recognise and treat such DSTs early may lead to catastrophic neurological complications. Finally, to conclude, all cases of DST, either suspected or confirmed with sonography, should undergo MRI imaging of the neuroaxis to assess for neural involvement and guide management.
Conflicts of interest: The authors declare no conflicts of interest. This case report received no funding of any sort.
References
- Murphy KJ, Brunberg JA, Quint DJ, Kazanjian PH. Spinal cord infection: Myelitis and abscess formation. AJNR Am J Neuroradiol. 1998; 19: 341-348.
- Vankipuram S, Sahoo SK, Srivastava C, Ojha BK. Spinal cord abscess secondary to infected dorsal dermal sinus in an infant: Uncommon presentation of a known entity. BMJ Case Rep. 2017; bcr-2017-222366.
- Prasad G, Hegde A, Divya S. Spinal Intramedullary Abscess Secondary to Dermal Sinus in Children. Eur J Pediatr Surg. 2019; 29: 229-238.
- Ackerman LL, Menezes AH. Spinal congenital dermal sinuses: A 30-year experience. Pediatrics. 2003; 112: 641-647.
- Park SW, Yoon SH, Cho KH, Shin YS, Ahn YH. Infantile lumbosacral spinal subdural abscess with sacral dermal sinus tract. Spine (Phila Pa 1976). 2007; 1: 52-55.
- Jindal A, Mahapatra AK. Spinal congenital dermal sinus: An experience of 23 cases over 7 years. Neurol India. 2001; 49: 243- 246.
- Singh I, Rohilla S, Kumar P, Sharma S. Spinal dorsal dermal sinus tract: An experience of 21 cases. Surg Neurol Int. 2015; 7: 429- 434.
- Nejat F, Dias MS, Eftekhar B, Roodsari NN, Hamidi S. Bilateral retro-auricular dermal sinus tracts with intradural extension: Case report. J Neurosurg. 2003; 99: 163-166.
- Elton S, Oakes WJ. Dermal sinus tracts of the spine. Neurosurg Focus. 2001; 10: e4.
- Foster MT, Moxon CA, Weir E, Sinha A. Dermal sinus tracts. BMJ. 2019; 366: l5202.
- Henriques JGDB, Pianetti G, Henriques KSW, Costa P, Gusmão S. Minor skin lesions as markers of occult spinal dysraphisms - Prospective study. Surg Neurol. 2005; 63: 8-12.
- Solak SS, Altunay IK, Demirci GT, Can B. Prevalence of Congenital Cutaneous Anomalies in 1000 Newborns and a Review of the Literature. Am J Perinatol. 2015; 33: 79-83.
- Choi JH, Lee T, Kwon HH, You SK, Kang JW. Outcome of ultrasonographic imaging in infants with sacral dimple. Korean J Pediatr. 2018; 61: 194-199.
- Zanello M, Zerah M, Di Rocco F. Quelle conduite devant une fossette sacrée ? Arch Pediatr. 2015; 22: 1298-1301.
- Tisdall MM, Hayward RD, Thompson DNP. Congenital spinal dermal tract: How accurate is clinical and radiological evaluation? J Neurosurg Pediatr. 2015; 15: 651-656.
- Kucera JN, Coley I, O’Hara S, Kosnik EJ, Coley BD. The simple sacral dimple: Diagnostic yield of ultrasound in neonates. Pediatr Radiol. 2015; 45: 211-216.
- Kriss VM, Desai NS. Occult spinal dysraphism in neonates: Assessment of high-risk cutaneous stigmata on sonography. Am J Roentgenol. 1998; 171: 1687-1692.
- Barkovich AJ, Edwards MSB, Cogen PH. MR evaluation of spinal dermal sinus tracts in children. Am J Neuroradiol. 1991; 12: 123- 129.
- Albert GW. Spine ultrasounds should not be routinely performed for patients with simple sacral dimples. Acta Paediatr Int J Paediatr. 2016; 105: 890-894.
- Ponger P, Ben-Sira L, Beni-Adani L, Steinbok P, Constantini S. International survey on the management of skin stigmata and suspected tethered cord. Child’s Nerv Syst. 2010; 26: 1719-1725.
- Khairy S, Azzubi M. Sacral Dimple. World Neurosurg. 2017; 101: e7-811.
- Mostafa M. Acute flaccid paralysis in a patient with sacral dimple. World J Clin Pediatr. 2013; 8: 26-30.
- Edmond K, Clark A, Korczak VS, Sanderson C, Griffiths UK, Rudan I. Global and regional risk of disabling sequelae from bacterial meningitis: A systematic review and meta-analysis. Lancet Infect Dis. 2010; 10: 317-328.
- Tacon CL, Flower O. Diagnosis and Management of Bacterial Meningitis in the Paediatric Population: A Review. Emerg Med Int. 2012; 2012: 320-330.
- Ku LC, Boggess KA, Cohen-Wolkowiez M. Bacterial meningitis in infants. Clin Perinatol. 2015; 42: 29-45.