
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Surgical - orthodontic planning of complex cases through the use of 3D models: A case report
Giovanni Guerra*; Domenico Guerra; Olimpia Ferrara; Mario Guerra; Leonardo Palazzo
Ambulatorio Odontoiatrico USL Umbria1 in Gubbio, Italy.
*Corresponding Author: Giovanni Guerra
Ambulatorio Odontoiatrico USL Umbria1 in Gubbio, Italy.
Email: mailgiovanniguerra@gmail.com
Received : Nov 26, 2021
Accepted : Dec 17, 2021
Published : Dec 24, 2021
Archived : www.jcimcr.org
Copyright : © Guerra G (2021).
Citation: Guerra G, Guerra D, Ferrara O, Guerra M, Palazzo L, et al. Surgical - orthodontic planning of complex cases through the use of 3D models: A case report. J Clin Images Med Case Rep. 2021; 2(6): 1512.
Introduction
Stereolithographic models are three-dimensional reproductions of digital data, created using CAD-CAM software. In recent years, the use of these three-dimensional models has increased as an aid in orthodontic diagnostics and in the planning of oral and maxillofacial surgery [1].
Unlike conventional diagnostic imaging techniques, such as Orthopanoramic radiographs and Cone-Beam CT (CBCT), which provide valuable digital information on bone size and geometry, stereolithographic models exhibit a physical three-dimensional reproduction of the anatomical area of interest with maximum accuracy. These truly guide both the diagnosis process and the surgical operation itself, in order to improve preoperative planning and minimize operative and postoperative morbidity.
For the reproduction of these models, a CBCT scan is necessary. Through a 3D printing software, the data is converted into a stereolithographic model in scale. It is produced with transparent resin for better visualization of the bone structures and internal anatomical structures involved, such as the path of the inferior alveolar nerve or, as in this case report, the presence of dental elements totally impacted in the bone [2,3].
The use of these three-dimensional models has demonstrated a series of advantages such as a more accurate planning both orthodontic and surgical treatment, a significant reduction of operating times, a reduction in the time of exposure of the wound, better communication with colleagues and patients and more predictable surgical results [1].
Toothimpaction is defined as the failed eruption of a tooth, which remains embedded in the maxillary or mandibular bone after its period of physiological eruption. It can be partial or total and it most commonly happensto third molars, especially mandibular wisdom teeth, followed by the maxillary canines. Unlike the third molars, the maxillary canines constitute dental elements of great functional importance. They play agreat role of control in the movements of mandibular excursion.
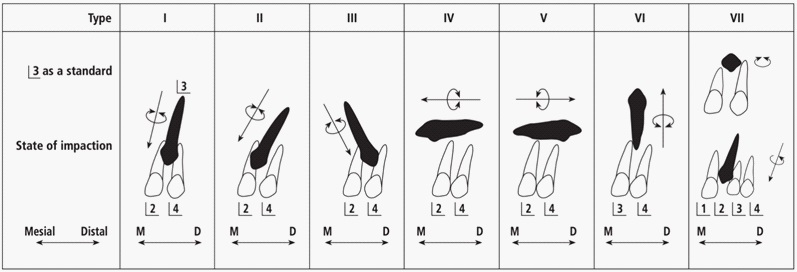
According to the classification of included maxillary canines by Yamamoto et al. there are 7 types (Figure 1), with the first three types showing more predictable results in the surgical orthodontic treatment and the following four types considered untreatable with orthodontic anchorage [4].
Case report
In the following case report, a 15-year-old patient came to visit for orthodontic problems. On intraoral physical examination (Figures 2,3,4), this shows an irregular mixed dentition with delays in the exchange of the upper left deciduous canine and the second upper left deciduous molar. Furthermore, there is a total absence of the deciduous and permanent upper right canine, with closure of the space between the upper right first premolar and lateral incisor.



The orthopanoramic radiograph shows the two permanent canines completely impacted within the maxillary bone and a delay in the eruption of the second upper left premolar. Through digital palpation of the buccal and palatal mucosa no swelling of the bone is detected, suggesting a deep impaction of the canines.
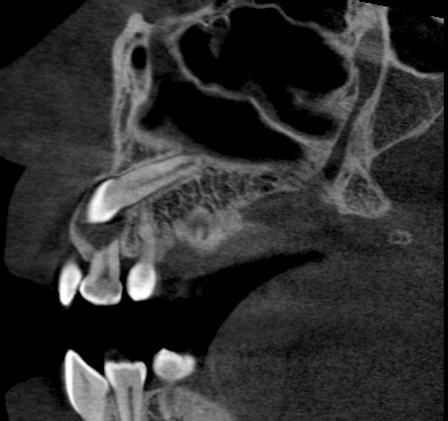
The CBCT scan (Figures 5,6) shows a type IV impaction of the two upper permanent canines [4], in an almost completely horizontal position, with the crowns located at the height of the apical third of the central incisors, in a mesio-buccal direction and the roots fully formed, in a disto-palatal direction.

Given the complexity of the case, a 3D model is requested in order to accurately establish the final treatment plan.
Through the analysis of the 3D model (Figures 7,8,9) and the in-depth study of the therapeutic alternatives, the impossibility of proceeding with the orthodontic surgical disinclusion by anchorage of the two permanent canines is evident, due to their position within the maxillary bone, in relation with the adjacent dental elements and their deep impaction. The presence of a discrete crowding with an important lack of space in the arch for all the dental elements and the horizontal position of the retained teeth leads, therefore, to opt for the surgical extraction of both canines through vestibular access.



The surgical operation begins with the injection of local anesthetic into the vestibule of the anterosuperior sector to induce analgesia (Figure 10). It proceeds with the realization of two sulcular incisions and full-thickness flaps along the teeth, from the central incisor to the first premolar of both arches, with two distal relief incisions at the level of said premolars (Figures 11,12).



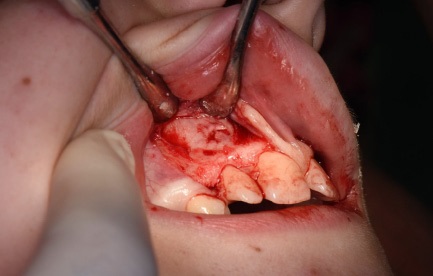
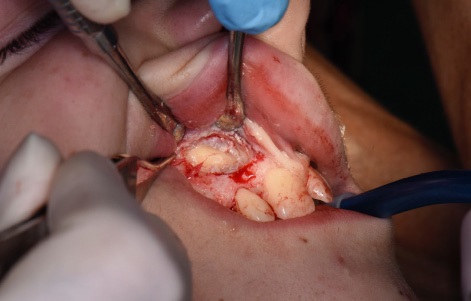
The flaps are then lifted with the periosteal elevator to expose the vestibular wall of the maxillary bone (Figures 13,14,15) and through the guide of the 3D model an ostectomy is carried out around the crowns of the two included canines with round bur mounted on straight handpiece (Figure 16).



Once the two crowns have been sufficiently exposed, the two elements are luxated using a straight lever and subsequently extracted (Figures 17,18,19,20).



Finally, the two flaps are repositioned with a simple suture and the prescription of adequate pharmacological therapy is given: Antibiotic therapy for the following five days and analgesic therapy at need.
The sutures are removed after 15 days and the patient is sent back for a follow-up visit to plan the fixed orthodontic treatment.
Conclusion
The stereolithographic model proved to be of great help both in the orthodontic diagnosis and in the preoperative and operative phases. The direct view of the impacted dental elements was decisive in taking the extraction route. Similarly, the frequent consultation of the model during the surgical operation, especially in the stages of incision and drawing of the flap and during the ostectomy, facilitated the identification of the crowns of the two elements and gave maximum precision to the surgery itself.
Therefore, the possibility of having such a diagnostic aid, in addition to those typically used, makes it possible to overcome the inevitable uncertainties in cases that show particular complexity and become decisive in guiding the final diagnostic and therapeutic decisions.
References
- Mehra P, Miner J, D’Innocenzo R, Nadershah M. Use of 3-D Stereolithographic Models in Oral and Maxillofacial Surgery. Journal of Maxillofacial and Oral Surgery. 2011; 10: 6–13.
- Ballard DH, Mills P, Duszak R, Weisman JA, Rybicki FJ, Woodard PK, et al. Medical 3D Printing Cost-Savings in Orthopedic and Maxillofacial Surgery: Cost Analysis of Operating Room Time Saved with 3D Printed Anatomic Models and Surgical Guides. Academic Radiology. 2020; 27: 1103–1113.
- Nayar S, Bhuminathan S, Bhat WM. Rapid prototyping and stereolithography in dentistry. Journal of Pharmacy and Bioallied Sciences. 2015; 7: 218.
- Yamamoto G, Ohta Y, Tsuda Y, Tanaka A, Nishikawa M, Inoda H, et al. A new classification of impacted canines and second premolars using orthopantomography. Asian J Oral Maxillofac Surg. 2003; 15: 31–37.