
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Placement of a metallic Y stent to address a large tracheoesophageal fistula on the carina
Konstantinos Kotsifas*; Stavroula Boulia; Georgia Eleni Chrysou; Arxontoula Antonoglou; Evangelos Balis
Pulmonary Medicine Department, Evaggelismos General Hospital, Athens, Greece.
*Corresponding Author: Konstantinos Kotsifas
Pulmonary Medicine Department, Evaggelismos
General Hospital, Athens, Greece.
Email: kotsifaskostas@yahoo.com
Received : Nov 03, 2021
Accepted : Dec 20, 2021
Published : Dec 27, 2021
Archived : www.jcimcr.org
Copyright : © Kotsifas K (2021).
Abstract
We report a case of a 43-year-old woman who presented with a large tracheoesophageal fistula involving the main carina after chemo-radiotherapy for lung adenocarcinoma. A self-expanding fully covered metallic Y stent was placed with the use of both rigid and flexible bronchospopy and fluoroscopic guidance. An esophageal stent was placed subsequently. The patient survived 8 months without relevant symptoms.
Keywords: tracheoesophageal fistula; metallic stent; esophageal stent; lung cancer.
Citation: Kotsifas K, Boulia S, Chrysou GE, Antonoglou A, Balis E. Placement of a metallic Y stent to address a large tracheoesophageal fistula on the carina. J Clin Images Med Case Rep. 2021; 2(6): 1515.
Description
Tracheoesophageal fistulae represent a severe complication of lung cancer and result in significant morbidity, while severely affecting patient’s quality of life.
A 43 year old woman presented with a right upper lobe adenocarcinoma and extensive mediastinal adenopathy. After chemotherapy with Cisplatin and Paclitaxel combined with Radiotherapy she continued on maintenace treatment with Durvalumab. However she gradually developed dysphagia, cough after swallowing and recurrent chest infections. A CT of the thorax revealed the presence of a large tracheoesophageal fistula at the level of the carina. It was confirmed both by bronchoscopy and esophagoscopy. Placement of a self expanding fully covered metallic Y stent was selected. Rigid bronchoscopy under general anesthesia secured the airway and ventilation. Under fluoroscopic guidance and flexible bronchoscopy two guidewires were advanced at the left and right bronchial tree respectively. The Y stent was then deployed over the guidewires, its position checked and the patient awakened and succescully extubated. An esophageal stent was placed the following day under sedation with esophagoscopy.
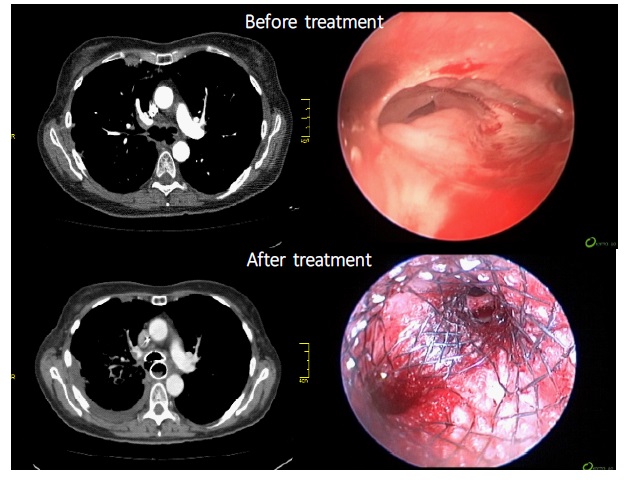
Representative CT and endoscopic images before and after the stents placement are shown in pictures.
The patient was relieved from symptoms and resumed oral intake without complications. Last follow up bronchoscopy 7 months later confirmed stent patency. Small granulomas on the stent edges were treated by cryotherapy. The patient succumbed to metastatic disease a month later.
Stenting is necessary as palliative treatment in cases of malignant tracheoesophageal fistalae to improve quality of life and prolong survival. Double stenting of both esophagus and airway is prefered as it has been shown to offer better results. Even if there is not airway stenosis, this complication may occur very soon as a result of the malignant process, or compression by the esophageal stent itself. Therefore airway stenting should be ideally performed before or concurrently with esophageal stenting.
Metallic airway stents offer advantages over silicone stents for malignant tracheoesophageal fistulae: they are more easily placed and conform better to the airway wall with much less risk of migration. Being fully covered they do not allow spillage of esophageal contents through the stent. Malignant or granulomatous ingrowth at the edges can be managed endoscopically. Risk of stent fracture and difficulty in removing, both disadvantages of metallic stents, are rarely an issue due to restricted patient survival. If however prolonged survival is anticipated, then a silicone airway stent should be equally considered.
References
- Freitag L, Tekolf E, Steveling H, et al. Management of Esophagotracheal Fistulas With Airway Stenting and Double Stenting. Chest. 1996; 110: 1155-1160.
- Ke M, Wu X, Zeng J. The Treatment Strategy for Tracheoesophageal Fistula. J Thorac Dis. 2015; 7: S389-S397.
- Zhou C, Hu Y, Xiao Y, Yin W. Current Treatment of Tracheoesophageal Fistula. Ther Adv Respir Dis. 2017; 11: 173-180.
- Khan A, Hashim Z, Neyaz Z, et al. Dual Airway and Esophageal Stenting in Advanced Esophageal Cancer With Lesions Near Carina. J Bronchol Intervent Pulmonol. 2020; 27: 286-293.