
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Role of permanent pacing for sinus node dysfunction related to percutaneous coronary intervention of the proximal right coronary artery
Gurjit Singh1*; Gregory Hazergian2
1 Clinical Assistant Professor, Wayne State University, Section of Cardiac Electrophysiology, Henry Ford Heart and Vascular Institute, Henry Ford Hospital, 2799 West Grand Boulevard, Detroit, Michigan 48202, USA.
2 Cardiovascular Medicine, Beaumont Farmington Hills, 28050 Grand River Ave, Farmington Hills, MI 48336, USA.
*Corresponding Author: Gurjit Singh
Clinical Assistant Professor, Wayne State University,
Section of Cardiac Electrophysiology, Henry Ford Heart
and Vascular Institute, Henry Ford Hospital, 2799 West
Grand Boulevard, Detroit, Michigan 48202, USA.
Email: dr_gurjit@yahoo.com
Received : Nov 03, 2021
Accepted : Dec 20, 2021
Published : Dec 27, 2021
Archived : www.jcimcr.org
Copyright : © Singh G (2021).
Keywords: sinus node dysfunction; right coronary artery occlusion; pacemaker; long term outcomes.
Citation: Singh G, Hazergian G. Role of permanent pacing for sinus node dysfunction related to percutaneous coronary intervention of the proximal right coronary artery. J Clin Images Med Case Rep. 2021; 2(6): 1516.
Introduction
There are few case reports relating to sinus node arrest resulting from percutaneous intervention of the proximal right coronary artery with majority showing resolution of normal sinus function within 7 days. Some reports have been published with prolonged recovery time of up-to 40 days [1,2]. The Sinoatrial (SA) node is supplied by the Sinoatrial Nodal (SAN) artery which originates from proximal Right Coronary Artery (RCA) in approximately 68% of patients, from left circumflex artery in 22.1% and from left main artery in 2.7% [3]. SAN artery is usually a single vessel in 95.5% hearts and duplication is seen in 4.3% [3]. Percutaneous Coronary Intervention (PCI) of the proximal RCA has been shown to cause side branch occlusion of the SAN artery in 17.5% of patients with sinus arrest and junctional escape rhythm in 28.6% of those patients [4]. We report long term outcome (3 years) of a patient with prolonged sinus node dys- function after stenting of the proximal RCA and insights into sinus node function recovery through pacemaker interrogations.
Case report
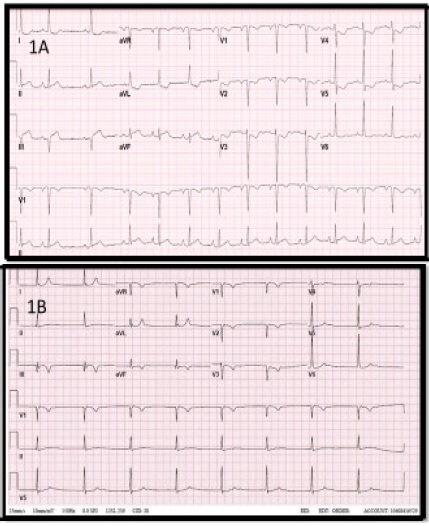
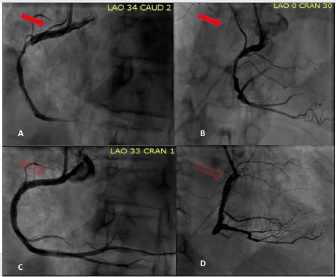
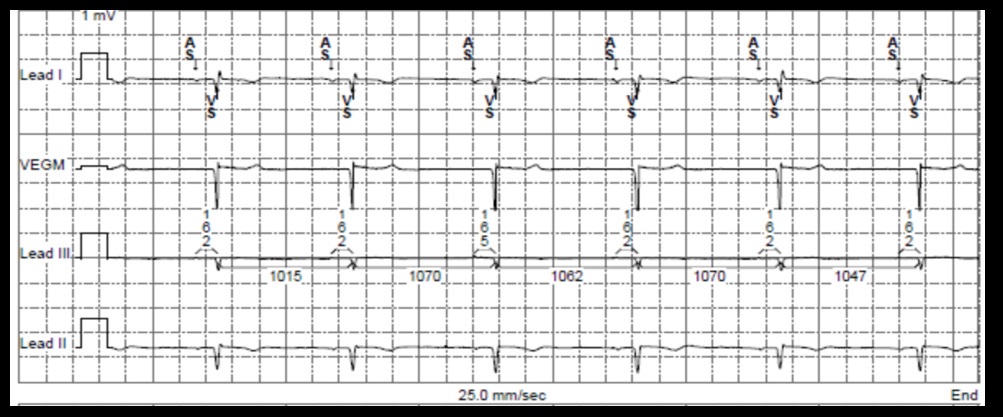
A 69 year old African American female with history of cerebrovascular accident and hypertension presented with chest pain, diaphoresis and shortness of breath. Her cardiac troponin I was elevated at 5.60 ng/ml with Electrocardiogram (ECG) showing an idioventricular rhythm. She progressed to develop ST segment elevation in the inferior limb leads within 3 hours of her presentation (Figure 1) and her troponin I level rose to 28.2 ng/ml. She underwent percutaneous intervention of proximal to distal RCA using 3.5 X 38 mm and 4.0 X 24 mm everolimus eluting stents. She developed an accelerated junctional rhythm (Figure 2) immediately after the procedure with stable hemodynamics which persisted until day 7. Transthoracic echocardiogram revealed an ejection fraction of 67% with mild hypokinesis of the basal-mid inferior wall. Due to uncertainty of recovery of sinus node function and no signs of sinus node activity with ambulation, a dual chamber pacemaker (Medtronic Inc ®) was implanted. Her pacemaker was programmed in AAIR⇔DDDR mode with lower rate limit of 60 bpm. She was discharged home with Aspirin 81 mg, Atorvastatin 80 mg, Clopidogrel 75 mg and Metoprolol succinate 25 mg. Review of the catheterization films revealed iatrogenic occlusion of the sinoatrial nodal artery likely due to side branch jail phenomenon from the proximal stent (Figure 3). An exercise stress test 74 days later revealed sinus rhythm at 70 bpm at baseline with maximal increase to 112 bpm (74 % of the predicted maximal heat rate) by stage IV of Haskell protocol. Her metoprolol dose was escalated to 150 mg dose for management of hypertension over next 3 years. Her atrial pacing requirement progressively increased to > 90 % over 3-year time. At her last pacemaker clinic visit, she continued to have an underlying atrial rhythm at 55 bpm (Figure 3).
Discussion
Sinus node dysfunction characterized by sinus bradycardia, sinus arrest, sinoatrial exit block, tachycardia-bradycardia syndrome results from either intrinsic disease characterized by replacement of nodal cells with fibrous tissue or extrinsic causes such as ischemia or pharmacologic agents [5]. Permanent injury by infarction or infection is uncommon [5]. The sinus node is a relatively large 13-30 mm subepicardial crescent shaped structure located in sulcus terminalis close to superior vena cava [6]. The SAN artery usually runs as a single vessel along the long axis of the sinus node and gives parallel branches inside, but sometimes the artery can branch outside the sinus node [7]. Occlusion of the sinus nodal artery during PCI does not always produce sinus arrest even when there is a single blood supply to the sinus node [4]. Most descriptions of sinus node arrest as a result of stenting of the proximal right coronary artery show recovery of sinus node function within one week, however there have been two case reports showing prolonged recovery of sinus node function. One case report involved a 75 year old woman who developed junctional escape rhythm after stent deployment with angiography revealing occlusion of the SAN artery [1]. She developed long pauses associated with syncope due to sinus arrest after 7 days which required temporary ventricular pacing followed by a permanent dual chamber pacemaker on day 14. An ectopic atrial rhythm was noted on day 28 and return to normal sinus rhythm was seen on day 40. Coronary angiography 6 months later revealed spontaneous recanalization of the SAN artery. Another report highlighted a 67 year old woman with acute inferior ST elevation myocardial infarction who required two Zotarolimus eluting stents to RCA complicated by SAN artery occlusion [2]. She developed a junctional escape rhythm followed by an atrial rhythm several hours later. This patient had an ectopic atrial rhythm at 3 months and sinus node recovery was documented at 6 months. There are no known long-term studies regarding monitoring and treatment of a junctional rhythm after sinus node arrest. The decision to implant a permanent pacemaker is usually aided by symptoms but in asymptomatic patient with junctional escape rhythm, this decision can be troubling. Our case highlights the natural history of sinus node dysfunction caused by ischemic insult due to SAN artery occlusion. We saw similar trend in recovery of sinus node function as other authors. Sinus node pacemaking activity is eventually restored which could be either due to spontaneous recanalization of SAN artery or development of collaterals. We acknowledge the limitation of not having a follow up coronary angiogram in our patient to show spontaneous recanalization. It has been shown that there is a steady fall in nodal cells and increase in connective tissue in the sinus node with age [7] and small amount of nodal cells are enough to maintain sinus node activity [8]. As such, the ischemic injury could potentially result in loss of some of nodal cells, but enough nodal cells remain intact to preserve the sinus node function. Our case highlights for the first time, long term outcome of ischemic sinus node insult after iatrogenic SAN occlusion. We have shown that the sinus node recovery is usually the norm, which can aid in delaying the decision to implant a permanent pacemaker in absence of any significant symptoms when confronted with escape junctional rhythm after SAN artery occlusion.
Conclusions
Sinus node dysfunction due to iatrogenic closure of sinus nodal artery during percutaneous intervention of proximal right coronary artery usually manifests as asymptomatic stable junctional rhythm. Long term prognosis is usually good with sinus node recovery being the norm and permanent pacemaker can be safely deferred in most patients.
Disclosures: None of the authors have any conflict of interest, financial or otherwise.
References
- Abe Y, A Tamura, J Kadota. Prolonged sinus node dysfunction caused by obstruction of the sinus node artery occurring during coronary stenting. J Electrocardiol. 2008; 41: p. 656-658.
- Nakou E.S., et al. Long-standing sinus arrest due to the occlusion of sinus node artery during percutaneous coronary intervention: Clinical implications and management. Int J Cardiol. 2016; 203: p. 432-433.
- Vikse J, et al. Anatomical Variations in the Sinoatrial Nodal Artery: A Meta-Analysis and Clinical Considerations. PLoS One. 2016; 11: p. e0148331.
- Kotoku M, et al. Sinus arrest caused by occlusion of the sinus node artery during percutaneous coronary intervention for lesions of the proximal right coronary artery. Heart Vessels. 2007; 22: p. 389-392.
- Mangrum J M, J P Di Marco. The evaluation and management of bradycardia. N Engl J Med. 2000; 342: p. 703-709.
- Ho S.Y. and D. Sanchez-Quintana. Anatomy and pathology of the sinus node. J Interv Card Electrophysiol. 2016; 46: p. 3-8.
- Davies M.J. and A. Pomerance. Quantitative study of ageing changes in the human sinoatrial node and internodal tracts. Br Heart J. 1972; 34: p. 150-152.
- Thery C, et al. Pathology of sinoatrial node. Correlations with electrocardiographic findings in 111 patients. Am Heart J. 1977; 93: p. 735-740.