
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Unusual case of pseudoaneurysm of ascending aorta eroding presternal soft tissue and sternum in a patient with miliary tuberculosis and a bioprosthetic aortic valve
Sneha Kumar Jayaswal, MBBS*; Siddhant Mehra, MBBS; Rohan Makwana, DNB; Varun Shetty, DNB, FRCS (CTS)
Department of Cardiac Surgery, Narayana Institute of Cardiac Sciences, Bangalore, India.
*Corresponding Author: Sneha Kumar Jayaswal
Department of Cardiac Surgery, Narayana Institute of Cardiac Sciences, Bangalore, India.
Email: drsnehakj@gmail.com
Received : Nov 04, 2021
Accepted : Dec 22, 2021
Published : Dec 29, 2021
Archived : www.jcimcr.org
Copyright : © Jayaswal SK (2021).
Citation: Jayaswal SK, Mehra S, Makwana R, Shetty V.. Unusual case of pseudoaneurysm of ascending aorta eroding presternal soft tissue and sternum in a patient with miliary tuberculosis and a bioprosthetic aortic valve. J Clin Images Med Case Rep. 2021; 2(6): 1523.
Introduction
Ascending aorta pseudo-aneurysms that erode into the presternal soft tissue and sternum are rare. The author describes the surgical approach of a bulging pulsatile suprasternal mass caused by a pseudoaneurysm of the ascending aorta in a patient with miliary tuberculosis and a bioprosthetic aortic valve.
Case report
A 60-year-old patient with an established diagnosis of pulmonary hypertension, rheumatic heart disease and a bioprosthetic aortic valve for 3 years, presented to the OPD with cough and breathlessness for 3 months, neck pain and a pulsatile swelling over the suprasternal region for 2 days.
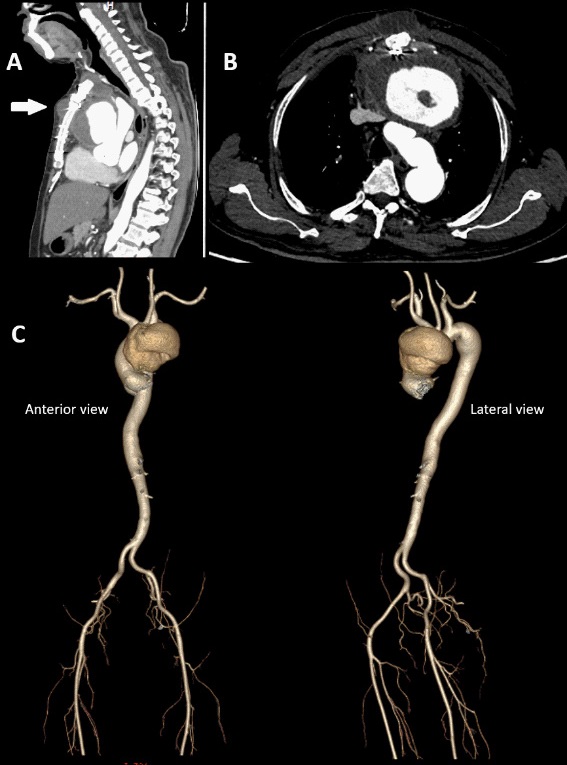
Systemic examination showed coarse inspiratory crepitations over the right infraaxillary and infrascapular regions. Initial investigations showed C-reactive protein of 49.3 mg/L, ESR of 43 mm/hr, AST of 92 U/L, ALT of 88 U/L, ALP of 145 IU/L, GGT of 161 U/L. CT chest revealed miliary nodules in both lungs suggestive of miliary tuberculosis and a well-defined heterogenous dense lesion in the anterior mediastinum adjacent to the anterior wall of the ascending aorta (size 5.5 X 7.3 cm) with hyperdense content (HU 40.0), of concern for pseudoaneurysm with thrombus. He was diagnosed with miliary tuberculosis and started on Anti-tubercular therapy.
On further investigations with Echocardiography, a pseudoaneurysm of ascending aorta, with a large, layered thrombus SEC and a normal functioning bioprosthetic aortic valve with an ejection fraction of 50-55% was seen. The pseudoaneurysm of the ascending aorta was communicating with the soft tissue space anteriorly and contained thrombotic material.
CT angiogram and 3D rendered imaging of the thoracic aorta showed a large pseudoaneurysm arising from the ascending aorta in the anterior mediastinum (Figure 1A,1B). It measured 7.5 X 10.5 X 8 cm with its neck measuring 2.5 cm. It also showed a layered thrombus with a maximum thickness of 2.5 cm and an irregular enhancing wall. Two small extra thoracic extensions with peripheral enhancing wall and internal thrombus was seen in the anterior chest wall-measuring 1.5 X 1.5 cm in the suprasternal region and 1.5 X 3.5 X 2.5 cm just below the sternal angle. It was seen to cause a mass effect over the right ventricular outflow tract, main pulmonary artery, proximal arch of aorta and left innominate vein.
Re-do emergency surgery for ascending aorta repair was planned.
The Left Common Carotid Artery (LCCA) and right femoral vein were exposed, and heparin was administered. The LCCA was cannulated with an 8 mm Dacron graft and the right femoral vein cannulated. The patient was put on Cardiopulmonary Bypass (CPB), cooled at 26 degrees, and systemic thiopental sodium and potassium was administered. Selective Anterograde Cerebral Perfusion (SACP) was started via the LCCA and the sternotomy was done using an oscillating saw. Following sternotomy there was anorganized thrombus in the mediastinum, with a big rent in the previous aortic suture line. There was a pulsatile mass over the proximal portion of the aorta and a contained rupture of the ascending aorta aneurysm. The previous valve was seen with no signs of degeneration. The aortic sinus was normal in size. There was a single origin of the innominate artery and the left common carotid artery.
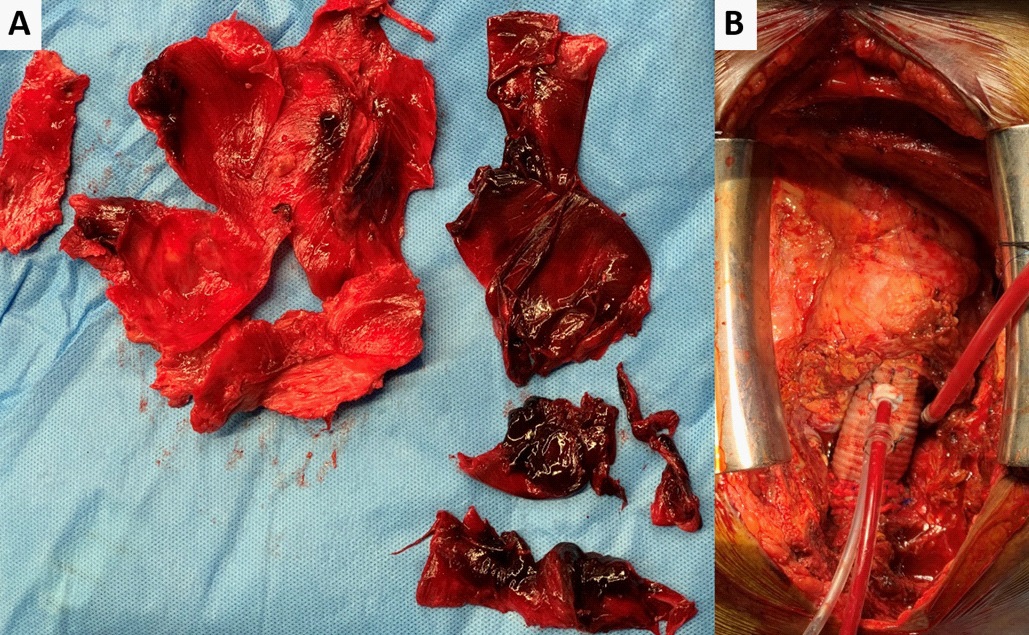
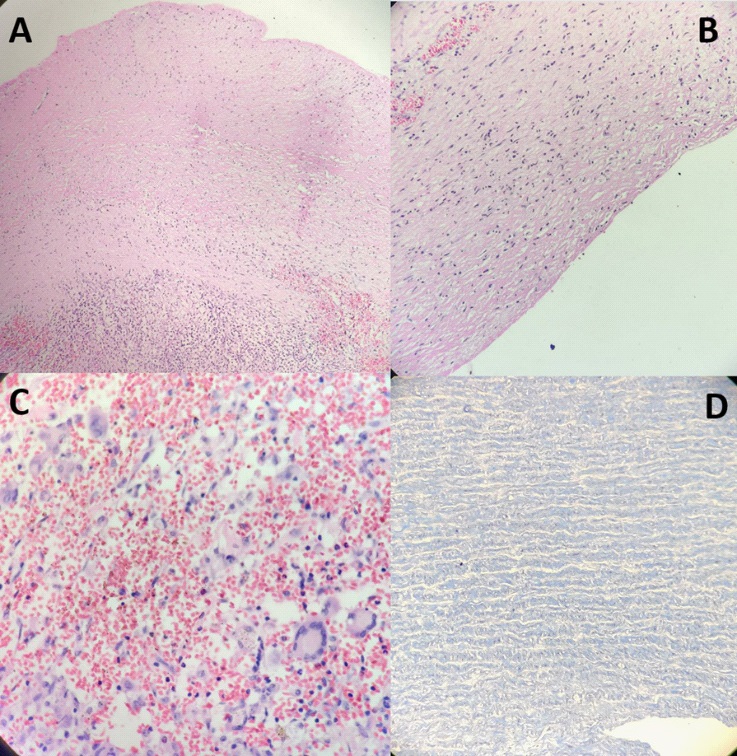
The thrombus was removed, and the aorta exposed to the level of the hemiarch (Figure 2A). The common neck artery was cannulated with a 16Fr SACP cannula following which ostial cardioplegia was given. The hemiarch was exposed and the aortic anastomosis was done with a 26 Fr Gelweave graft using continuous 4-0 polypropylene sutures. The circulation resumed with the LCCA graft and rewarming was done. The aorta de-aired and the X clamp applied to the graft. The proximal aorta dissected from the surrounding structures. The heart vented via the right superior pulmonary vein. The bioprosthetic valve was left in place and the ascending aorta graft was attached proximally just after the coronary ostia opening (Figure 2B). The aortic anastomosis was done at the level of the sinotubular junction using interrupted pledgeted mattress sutures. The specimen of the aorta was sent for histopathological examination. Histopathology section showed fibroelastic wall with ulceration of endothelial lining with fibrino-hemorrhagic material and hyalinization of media (Figure 3A,3B,3C). Post-operatively the neck pain and suprasternal swelling resolved. The patient is continuing to do well one-monthpost-surgery.
Discussion
Similar case reports of an ascending aorta aneurysm eroding into the sternum and anterior soft tissue caused by trauma [1] or related to infection with luetic disease [2] have been published. However the etiology in our patient is due to infectious miliary tuberculosis and cough causing increased intrathoracic pressure transmitting to the aorta. [3]
The management of this emergency condition was challenging, and an important surgical consideration was protecting the cerebral circulation while reopening the chest with the aneurysm at the front. We used hypothermia for Circulatory arrest along with antegrade cerebral perfusion to extend the safety margin [4]. Reports have stated that unilateral Anterograde Cerebral Perfusion (ACP) combined with hypothermic circulatory arrest had the same neurological outcomes as a bilateral ACP with hypothermic circulatory arrest [5,6]. Since the time from reopening the sternum to managing the arch branches was dependent on the severity of adhesions from the previous operation, direct cannulation of the left common carotid artery with a separate neck incision was chosen in this patient. The antegrade brain perfusion technique allowed direct cannulation of the arch vessels after opening the aorta or clamping the origin of the innominate.
References
- Porapakkham P. Impending rupture of aortic aneurysm eroding skin and sternum: A rare condition. Asian Cardiovascular and Thoracic Annals. 2019; 27: 307-309.
- Bodhey NK, Gupta AK, Neelakandhan KS, Unnikrishnan M. Early sternal erosion and luetic aneurysms of thoracic aorta: Report of 6 cases and analysis of cause–effect relationship. European journal of cardio-thoracic surgery. 2005; 28: 499-501.
- Wei JY, Harris WS. Heart rate response to cough. Journal of Applied Physiology. 1982; 53: 1039-1043.
- Veeragandham RS, Hamilton Jr IN, O’Connor C, Rizzo V, Najafi H, et al. Experience with antegrade bihemispheric cerebral perfusion in aortic arch operations. The Annals of thoracic surgery. 1998; 66: 493-499.
- Özatik MA, Küçüker ŞA, Tülüce H, Sartıaş A, Şener E, et al. Neurocognitive functions after aortic arch repair with right brachial artery perfusion. The Annals of thoracic surgery. 2004; 78: 591- 595.
- Lu S, Sun X, Hong T, Yang S, Song K, et al. Bilateral versus unilateral antegrade cerebral perfusion in arch reconstruction for aortic dissection. The Annals of thoracic surgery. 2012; 93: 1917- 1920.